
記住我
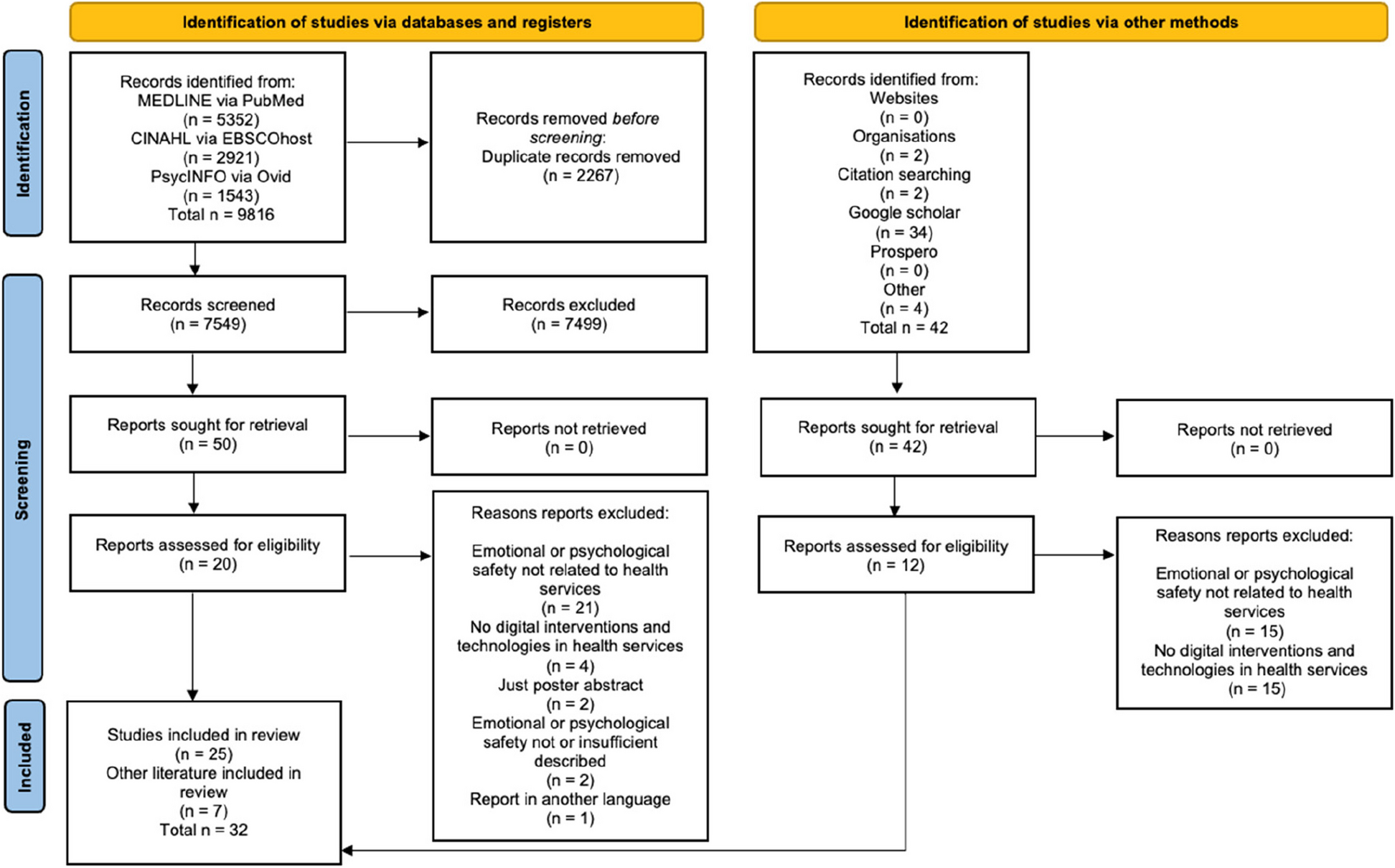






The literature search identified 3565 potentially relevant citations, 509 of which were included at the abstract screening level. From these, a total of 443 abstracts were excluded, leaving 66 publications for full-text review. See Fig. 1 for the flow and online Additional file 1: Appendix 5 for a list of excluded studies from the full-text review. Details of included publications are available in the evidence table online Additional file 1: Appendix 4.
Fig. 1
We identified 18 publications that met the inclusion criteria, all of which were observational. Two of these [21, 22] were propensity-matched for patient characteristics such as age, sex, comorbidities, severity of surgical disease, and surgical approach. The majority of the studies were single-institution designs (N = 14). Most studies evaluated DAPT management at the time of CABG (N = 12), 3 studies evaluated surgeries categories as non-cardiac, and 1 study combined cardiac and non-cardiac surgery. Lastly, there was 1 study each evaluating hip fracture surgery and renal transplant outcomes. The strategies for perioperative management of DAPT varied: the most common approach compared different durations of time between stopping an antiplatelet agent prior to surgery (N = 11). Other comparisons included discontinuing 1 or both antiplatelet agents compared to continuing. One study compared a P2Y12 inhibitor discontinuation with IV tirofiban infusion (N = 1).
Risk of biasFor the 18 observational studies, the quality of the studies was variable. Only 1 study was at low risk of confounding and the remainder were at medium or high risk. See online Additional file 1: Appendix 3 for the ROBINS-I assessment of studies. The studies that did not include consecutive, random, or a full sample of patients were considered at moderate risk for selection bias (N = 10). There was an overall low risk of bias in the classification of the interventions and deviation from these intended interventions (we judged retrospective chart review of drugs a patient received and the surgical procedure to be accurate). Missing data was not considered a significant source of bias given the use of retrospective chart reviews as the data source and the short-term (perioperative) outcomes of most studies. Finally, several studies were at moderate or high risk of measurement bias, usually due to using unvalidated or non-standard measures of bleeding(N = 8), such as varied methods of measuring intraoperative or postoperative blood loss. Several studies did not report cardiovascular outcomes and did provide a rationale for why clinically useful outcomes were not included. We felt that these may be at risk for reporting biases (N = 7).
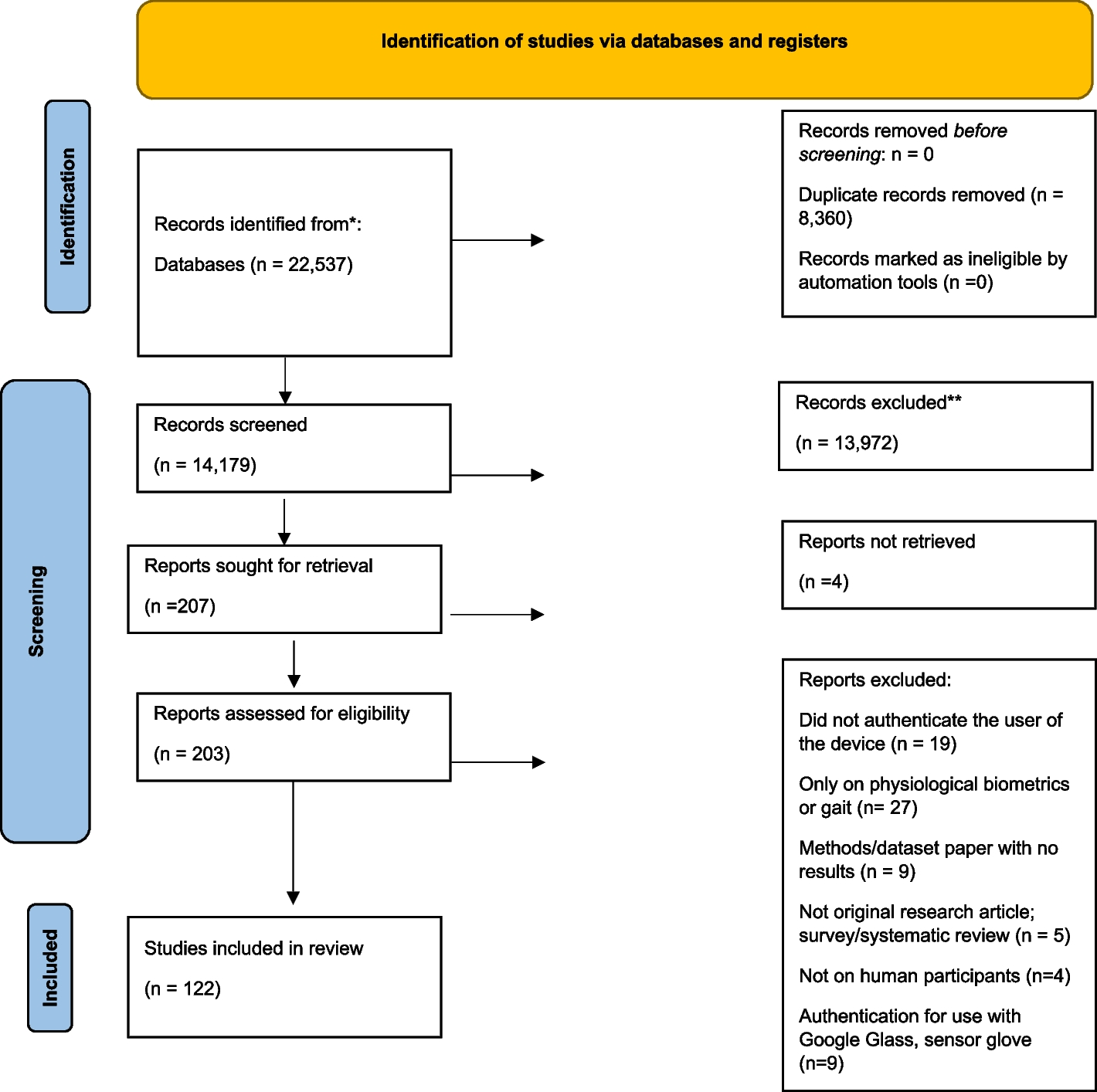
Patients on preoperative DAPT and undergoing CABGBlood lossEleven observational CABG studies contained sufficient data on postoperative blood loss to be presented collectively in Fig. 2. Of these, 8 compared suspending DAPT (defined as holding P2Y12 inhibition with continuation of acetylsalicylic acid [ASA]) at various preoperative timepoints, which we dichotomized as ≤ 2 days withdrawal or > 2 days withdrawal. Of note, 1 study that grouped 48–72 h was placed in the > 2 days withdrawal group [23]. A second study had comparison groups of 0–3 days and > 4 days, which were reassigned to ≤ 2 and > 2 withdrawal days, respectively [24]. The remaining 3 studies compared discontinuation DAPT, defined as stopping one or both ASA and a P2Y12 inhibitor, to continuing DAPT until surgery. In 6 of the 11 studies shown in Fig. 2, mean blood loss was statistically lower in patients that either experienced withdrawal of DAPT > 2 days preop or discontinuation of DAPT. The other 5 studies showed no significant differences in mean blood loss between DAPT management groups. Only 2 studies [25, 26] reported higher blood loss in the DAPT-withheld or discontinued groups; however, these differences were minimal (≤ 30 mL) and nonsignificant. Longer duration of suspension of DAPT therapy (i.e., for more than 2 days) favored less blood loss; however, the differences amounted to < 300 mL on average.
Fig. 2 Transfusions
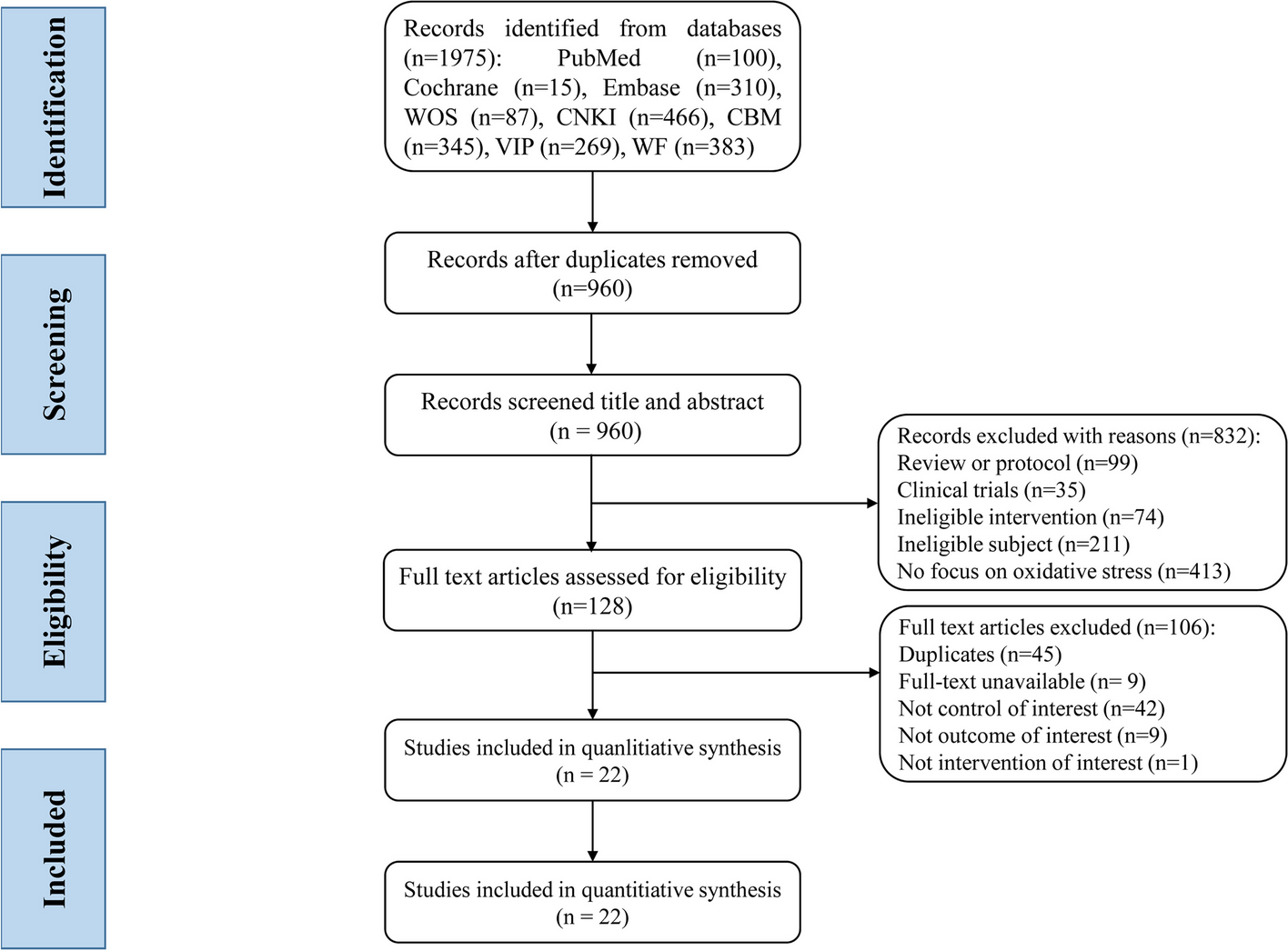
TransfusionsDifferences in red blood cell transfusion requirements across DAPT strategies from the 9 observational CABG articles that reported transfusion outcomes are shown in Fig. 3. Of the 9 available studies, 4 showed less transfusion requirements for > 2 days DAPT withdrawal or discontinuing DAPT, 4 reported nonsignificant results (3 of which favored > 2 days DAPT withdrawal or discontinuation), and only 1 study [27] reported statistically more transfusions in the DAPT discontinuation group.
Fig. 3 Re-explorations
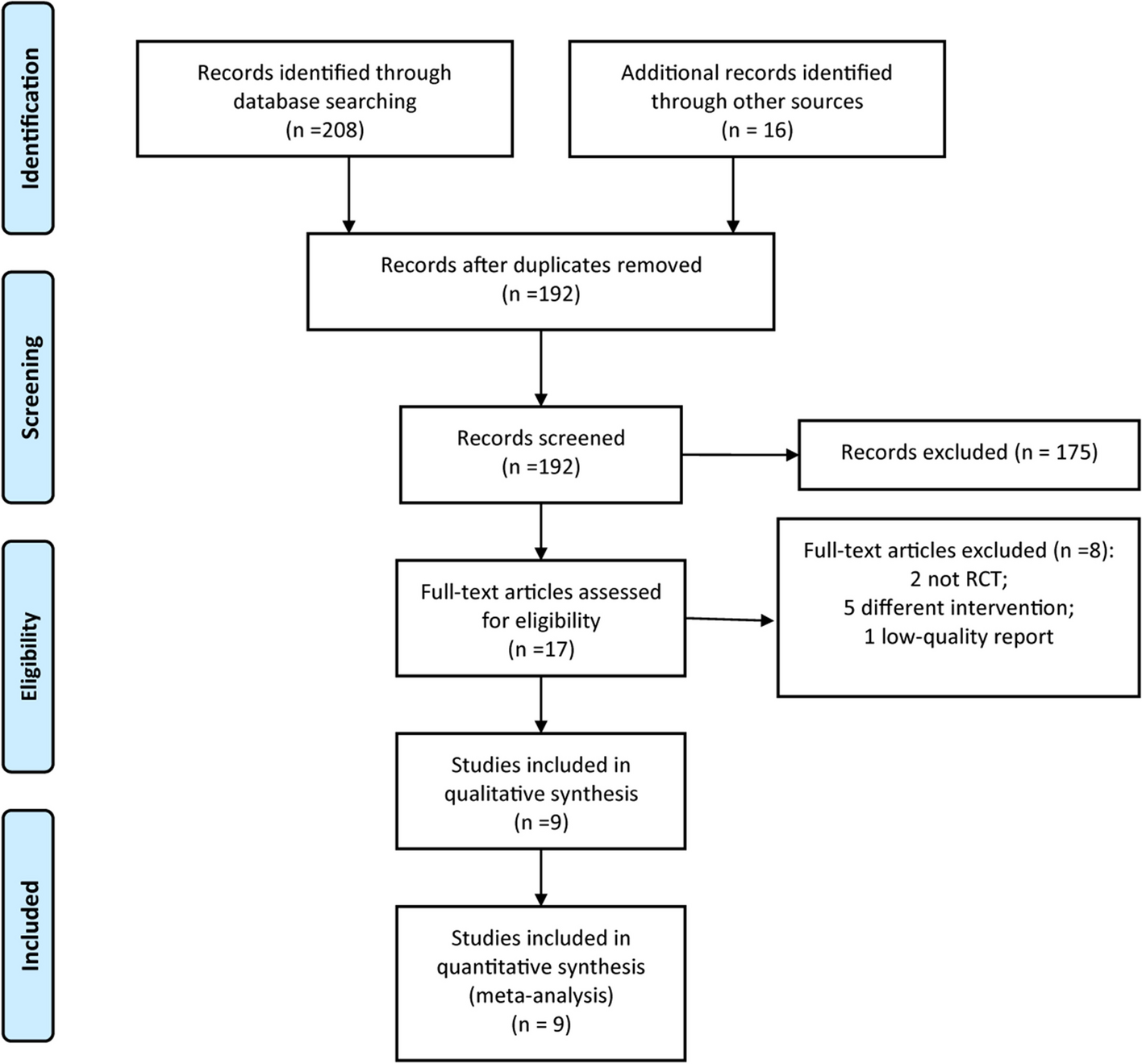
Re-explorationsSurgical re-exploration data showed a similar pattern, with all the point estimates favoring less re-exploration in patients with > 2 days DAPT withdrawal (in 2 of 5 studies this difference was not statistically significant). In contrast, the 2 studies comparing DAPT discontinuation to continuation found no difference in re-exploration (Fig. 4).
Fig. 4 Perioperative death
Perioperative deathThere were 4 observational CABG studies that reported mortality risk differences across comparison arms (shown in Fig. 5) and 1 additional study [23] that reported mortality as odds ratios. None of these reported significant differences in patient death across DAPT management strategies.
Fig. 5
Perioperative death outcomes
Cardiac outcomesThere were too few CABG studies that reported similar cardiac outcomes to the graph. Nardi and colleagues [23] observed no incidences of myocardial infarction for all DAPT management strategies, which included holding P2Y12 inhibition for 0 to 4 days prior to CABG. In a multicenter observational study of patients undergoing isolated CABG, Gielen et al. found no significant association between the last use of DAPT and MACE (odds ratio [OR] = 0.85, 95% CI [0.64, 1.14], P = 0.27).
Patients on preoperative DAPT and undergoing non-cardiac surgeryThree studies reported outcomes after non-cardiac surgery [28,29,30]. Due to the variance in reported outcomes, it was not possible to create graphs as was done for the CABG studies, and we discuss each study narratively below.
Irie and colleagues identified 133 patients on DAPT post-cardiac stenting who underwent emergency non-cardiac surgery (57.9% abdominal, 9% vascular) and determined predictors of life-threatening and major bleeding within 180 days of surgery (N = 18 patients who experienced a major bleeding event) [28]. There was no significant association between the type of P2Y12 inhibitor and the risk of bleeding (unadjusted). In addition, of those who had major or life-threatening bleeding, 61% had restarted antiplatelet therapy less than 2 days after surgery compared to patients who did not develop these bleeding complications (61.1% vs 26.1%; unadjusted P = 0.005). After adjusting for potential confounders, overall mortality was higher in the bleeding group compared to patients without bleeding; however, the difference did not reach statistical significance (180-day mortality: 4 (22.2%) in the bleeding group vs 9 (7.8%) in no bleeding group; P = 0.06).
Cao and colleagues evaluated 747 patients who underwent non-cardiac surgery (33% vascular, 23% gastrointestinal surgery) within 1 year of cardiac stenting and compared outcomes among those who interrupted antiplatelet therapy and those who did not [29]. There was no association between antiplatelet therapy management and MACE after adjusting for patient factors and procedure urgency (adjusted odds ratio [aOR] = 1.23, 95% CI [0.55, 2.74], P = 0.62) or death within 30 days (aOR = 1.21, 95% CI [0.49, 2.98]). However, there were 83% increased odds of bleeding (defined as > 2 units transfused) among patients with no interruption of antiplatelet agent (aOR = 1.83, 95% CI [1.11, 3.01], P = 0.018), which the authors note tended to occur sooner after cardiac stenting.
The third study of antiplatelet management after cardiac stenting by Kim and colleagues compared discontinuing (N = 1750) versus continuing 1 or both antiplatelet agents (N = 1832) for at least 1 day prior to non-cardiac surgery across 9 institutions [30]. Here, the most common types of surgeries that antiplatelet therapy was discontinued included gynecologic, breast, head and neck, and intraabdominal surgeries, while other types such as vascular and ophthalmologic surgeries more often continued antiplatelet therapy. When comparing continuation versus discontinuation of antiplatelet therapy across all surgeries, the authors found no effect of antiplatelet discontinuation on MACE in a risk-adjusted Cox proportional hazards model (adjusted hazard ratio [HR] = 1.13, 95% CI [0.57, 2.24], P = 0.721) or in major bleeding when antiplatelet agents were discontinued (adjusted HR = 1.22, 95% CI [0.80, 1.87], P = 0.349). The authors also conclude that an optimal duration for discontinuing antiplatelet therapy is 4–8 days, as this was associated with the lowest risk of MACE (unadjusted HR = 0.12; 95% CI [0.03, 0.52], P = 0.019).
Patients on preoperative DAPT and undergoing surgery for hip fractureWe identified 1 retrospective study of 122 patients taking DAPT who required fixation or hip arthroplasty for hip fracture that assessed whether the duration of DAPT discontinuation was associated with relevant clinical outcomes [21]. This study design could not isolate the effects of DAPT washout periods from confounding due to other reasons for medical delay of surgery. They found a small increased adjusted odds of 30-day mortality for each day of operative delay (OR = 1.32, 95% CI [1.03, 1.68], P = 0.030) but no association with units transfused among 11 patients requiring transfusion (incidence rate ratio = 1.00, 95% CI [0.87, 1.15], P = 0.968). The authors concluded that there was no benefit to surgical delay after hip fracture for older adults on DAPT.
Patients on preoperative DAPT and undergoing renal transplant surgeryOur search identified 1 study that compared antiplatelet interruption before renal transplantation in 106 patients with prior coronary stent placement [31]. There were no significant differences in cardiovascular clinical outcomes, including stent thrombosis (P = 0.465), myocardial infarction (P = 0.840), MACE (P = 0.840), and death (P = 0.411), for early versus late DAPT interruption after second-generation DES or BMS placement. The authors conclude that early interruption of DAPT after stent placement in preparation for renal transplant surgery was a safe strategy and did not lead to increased ischemic complications.
Certainty of evidenceThe certainty of evidence for each of the outcomes and DAPT management strategies is shown in Table 1 below. In general, all outcomes were judged to have serious limitations due to study design and execution issues, and there were no RCTs available. All outcomes were judged to have no limitations due to directness, as the outcomes measured were judged to be both sufficiently accurately assessed and the outcomes that matter to patients. All outcomes were judged to have limitations due to imprecision, even if the directionality of results was consistent. Some outcomes were judged to have inconsistent results across studies (bleeding, transfusions, re-explorations, etc.), while some other outcomes were judged to be consistent, in part because there were so few studies (re-explorations, MACE outcomes), these latter all being judged as very low certainty evidence. In sum, there were no outcomes/DAPT strategy choices that were judged to be high or even moderate certainty of evidence. A few outcomes associated with bleeding (i.e., blood loss, transfusions) were judged to be low certainty evidence, and all other outcomes, including other possible interventions (bridging, other potential antiplatelet therapy [APT] variations) and all other outcomes (including limb outcomes), were judged to be very low certainty evidence since there was either a single observational study or no studies informing the decision.
Table 1 GRADE for the certainty of evidence
留言 (0)