
Remember me
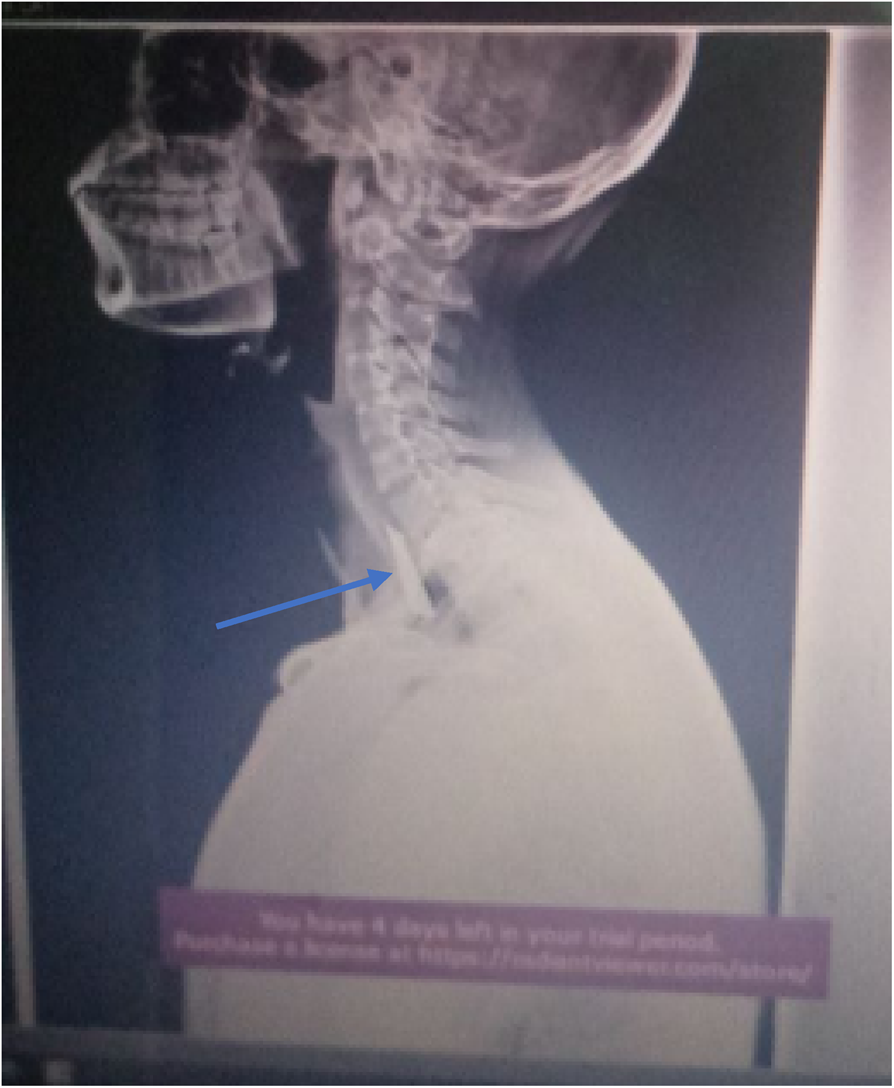





A 63-year-old patient, without any pre-existing condition, suffered from OHCA during daytime in an urban environment. His wife alerted the emergency medical services and performed bystander cardiopulmonary resuscitation (CPR). Six minutes after the initial call, the ambulance team consisting of one paramedic, one paramedic in training, and one emergency medical technician arrived on the scene. The first rhythm assessed was VF and the first shock was delivered by the ambulance crew (Fig. 1A). Approximately 15 min after the emergency call, the physician response unit, staffed with an anesthesiologist and two paramedics, arrived on the scene. Advanced life support (ALS) was continued with epinephrine and amiodaron applications according to current ALS guidelines [4]. After the sixth shock, the patient achieved a return of spontaneous circulation (ROSC) for the first time, approximately 29 min after the collapse. Due to ongoing hemodynamic and arrhythmogenic instability, the Medical Intervention Car (MIC), a specialized response vehicle, was alerted 45 min after the initial call, and 2 g magnesium was applied. The MIC is staffed with two anesthesia consultants and one anesthesia resident with special training in prehospital emergency medicine and equipped with a primed ECMO machine (Cardiohelp, Getinge Germany, Rastatt, Germany), portable transesophageal echocardiography (TEE), and near-infrared spectroscopy (NIRS).
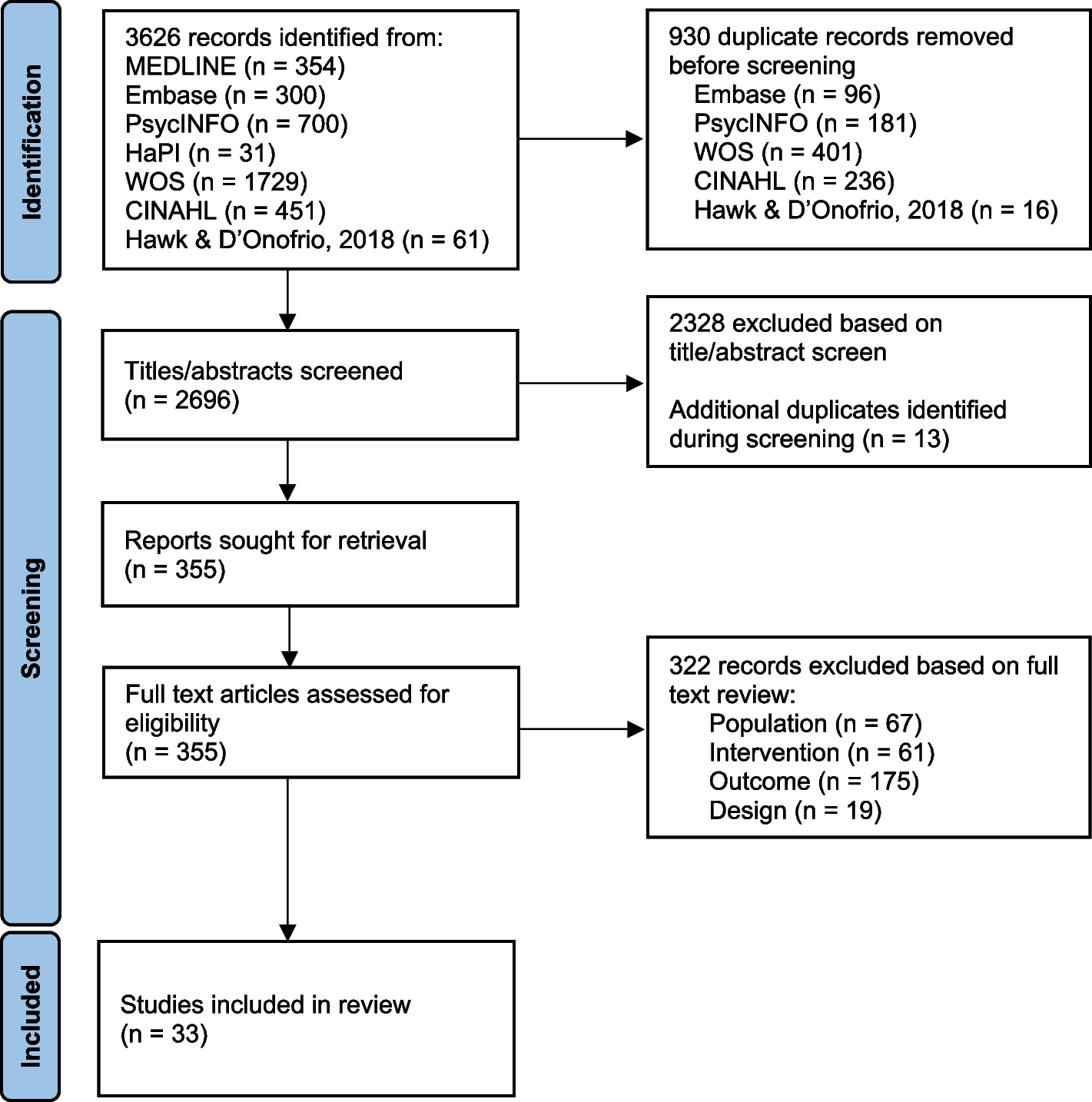
Fig. 1
Defibrillations throughout the course of the resuscitation. Defibrillator pads of shocks A–K were placed in the standard position, while L was placed in the anterior–posterior position. Shocks K and L were delivered with two devices at the same time. Times are stated as minutes after collapse
At the time the MIC arrived, the endotracheally intubated patient had ROSC with continuous non-invasive blood pressure (cNIBP) of 83/66 mmHg, end-tidal CO2 (etCO2) of 40 mmHg, arterial oxygen saturation (SpO2) of 92%, and left and right forehead NIRS baseline values of 51% and 32%, respectively (Fig. 2).
Fig. 2
Near-infrared spectroscopy cerebral oximetry values from the MIC arrival until the handover at the cath lab with minutes after collapse at the respective timepoints. Abbreviations: MIC, Medical Intervention Car; eCPR, extracorporeal cardiopulmonary resuscitation; DSED, double sequential external defibrillation
As a routine intervention for unstable patients, the placement of two 4-French introducer sheaths in the femoral artery and vein was performed. During this intervention, the patient deteriorated again into recurrent VF, ALS was resumed, and a third dose of 150 mg amiodaron was given, which accounted for a total of 600 mg amiodaron. A team-based decision was made to initiate eCPR by exchanging the two introducer sheaths for ECMO cannulas and connect them to the primed Cardiohelp ECMO. Manual chest compressions were resumed, as no mechanical CPR device was at the patient’s bedside. Confirmation of correct guidewire and cannula position was performed using TEE. During eCPR cannulation, a seventh shock was delivered with the patient remaining in VF.
Return of circulation (ROC) with ECMO flow of 4 l/min was achieved 76 min after the initial collapse, with 47 min of total low flow time. Initial sweep gas flow was 1 l/min with FiO2 at 50%, as per institutional guidelines. Due to logistic reasons, prehospital blood gas analysis was not available for this case.
When the patient did not spontaneously convert into a perfusing rhythm on eCPR, 100 mg lidocaine and a bolus of 50 µg norepinephrine were applied. Three shocks were delivered 2, 3, and 10 min after ROC (Fig. 1H–J), respectively. TEE showed increased spontaneous contrast with incipient stasis in the left atrium and ventricle. The decision was made to perform DSED as a measure of last resort. Both shocks were delivered simultaneously by the same person using two identical devices (Corpuls3T, GS Elektromedizinische Geräte G. Stemple, Kaufering, Germany) with ± 200 Joules each. The patient immediately converted into a perfusing rhythm (Fig. 1K, L), with a raise in etCO2 from 8 to 39 mmHg and a further increase of NIRS values (Fig. 2). Despite the help of the local fire brigade, extrication from the first floor took 25 min. The patient was transported directly to the catheterization laboratory of the nearest cardiac arrest center where the team arrived 52 min after ECMO flow had been established. The occluded coronary artery (left anterior descending) was successfully stented approximately 200 min after the initial collapse. Unfortunately, the patient died due to a traumatic subarachnoid hemorrhage suffered from the initial collapse and probable aggravation by heparin and antiplatelet therapy.
Comments (0)