Axillary management of initially node-positive patients who become node-negative after NAST remains controversial. However, with increasing evidence, the trend toward less invasive surgical procedures continues [11, 12]. Over the years, the number of breast cancer patients receiving NAST has increased at our institution. In cN + patients converting to ycN0 after NAST, we have adopted SLNB with double tracer technique and at least 3 SLNs removed. The proportion of upfront ALNDs at our institution has decreased accordingly (85% upfront ALNDs in 2012–2013, 61% in 2015–2016, and 50% in 2020–2021).
The main concern with SLNB in patients with cN + disease in the neoadjuvant setting remains the high FNR [13]. Although the purpose of axillary surgery is to both stage the axilla and remove any residual disease, it is unclear whether a higher FNR is actually associated with a higher regional recurrence rate and a worse prognosis. Detection of post-treatment changes in SLNs has been proposed as one of the principles for evaluating false negatives [6]. Brown et al. have shown that the absence of post-treatment changes in SLNs has a sensitivity of 82% and a specificity of 65% for detecting a false-negative SLN [14]. Post-treatment changes were present in 50% of SLNs, and the median number of SLNs removed was 2. In the study by Barrio et al., post-treatment changes were present in 88% of SLNs, and the median number of SLNs removed was 4 [15]. An alternative approach to assessing false negativity is clip placement at the time of initial nodal diagnostic biopsy. In the subgroup analysis of the Z1071 trial where a clip was used, it was identified in 75% of cases at SLNB only [16].
In our single-center retrospective study, post-treatment changes were identified in 70% of ypN0 patients (57/82) with a median of 3 SLNs removed. To our knowledge, we are the first to report the prognostic significance of absent post-treatment changes in SLNs in patients with biopsy-proven cN + disease undergoing NAST.
The probability of identifiyng post-treatment changes in our cohort of patients undergoing SLNB only was higher when more SLNs were removed, which supports the need for consistent sampling of at least 3 SLNs in cN + patients after NAST. However, the absence of post-treatment changes in SLNs did not translate into worse regional control in our cohort.
According to the literature, post-treatment changes were detected in more than 90% of ALND specimens [15]. This is comparable to our results; the patients that underwent ALND during our study period had post-treatment changes detected in 89%. In addition to false negativity, the absence of post-treatment changes in SLNs may also be explained by failure to identify the changes by the pathologist and to nodal sampling. In the present study, the first problem was partially adressed by reevaluation of the original H&E and IHC slides.
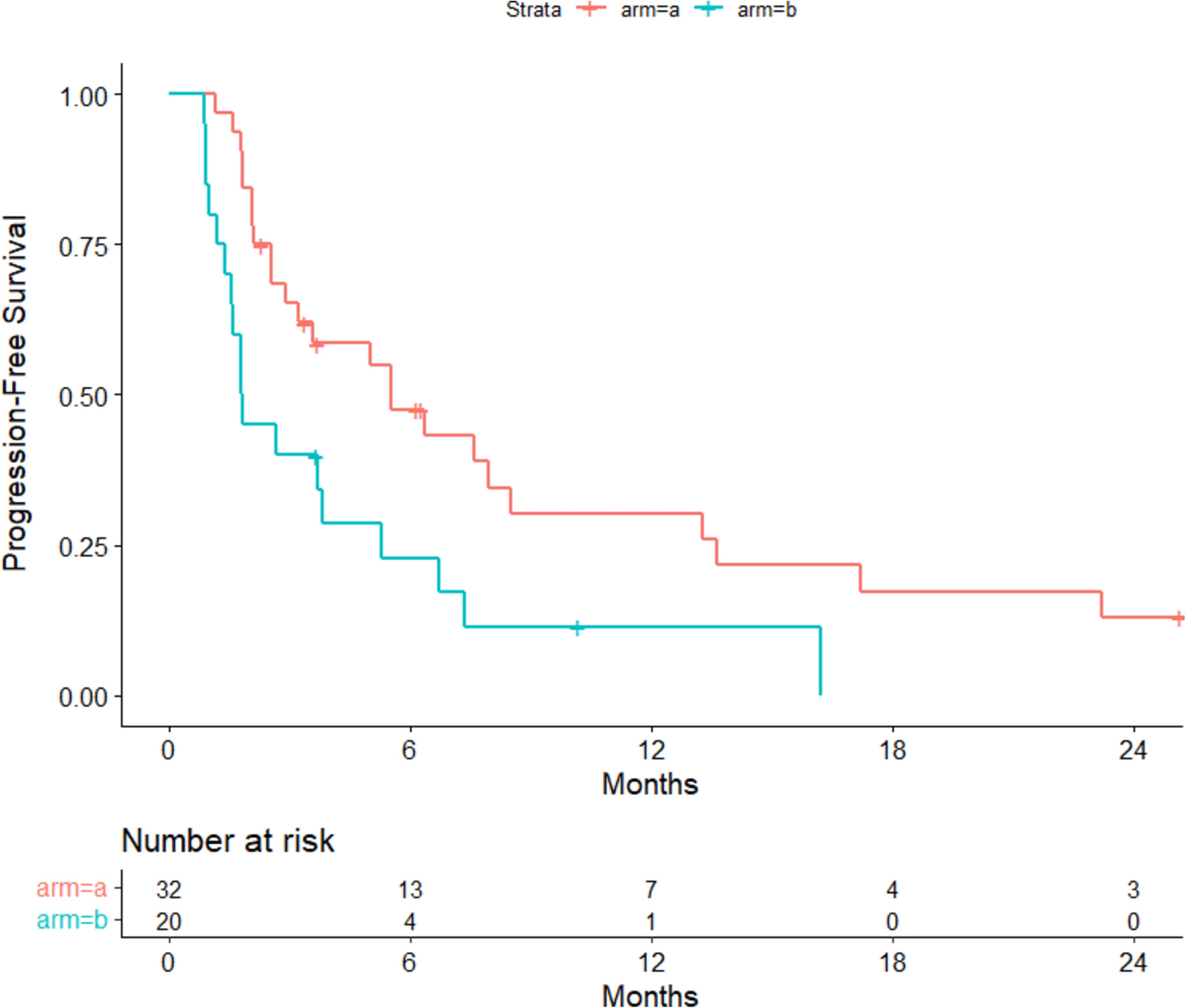
In our cohort of 82 patients with cN + disease who were ypN0 after SLNB only, there was only one (1.2%) isolated axillary recurrence during a median follow-up of 41 months. The regional recurrence rate in our cohort is within the range of previously published studies (0–1.6%) [11, 17,18,19,20]. The patient with regional recurrence underwent salvage ALND and is disease free 28 months after ALND.
Consistent with the study by Piltin et al., patients with ITC were classified as ypN0 in our study, although this is still controversial in the neoadjuvant setting [11]. Patients with ITC seem to carry a better prognosis than patients with macrometastases, but it is not entirely clear whether they can be classified as pCR/ypN0 [20,21,22]. The ongoing ICARO study may provide additional clarity on the oncologic outcomes for patients with ITC who undergo ALND, nodal RT or observation only after SLNB.
In women with cN + disease who respond well to NAST and are downstaged to ypN0, the role of RT in preventing locoregional recurrence is not entirely clear. The NSABP B-51 trial will shed light on the role of adjuvant RT in reducing recurrence rates in these patients. In our clinical practice, the need for regional nodal RT has been determined primarily by the status of the axillary nodes prior to NAST, regardless of response to treatment (ypN0 or ypN1). In our study, the vast majority of patients received adjuvant RT (93% of patients with post-treatment changes and 96% of patients whithout post-treatment changes received adjuvant RT).
Limitations of the current study include its retrospective nature and a median follow-up time of only 41 months. However, it has been shown that the majority of nodal recurrences occur in a follow-up period of up to 5 years, so a longer follow-up period would not likely change the results significantly [18, 23, 24]. Although we follow the national guidelines for performing SLNB after NAST in patients with cN + disease, which include the use of dual tracers and removal of at least 3 SLNs, we do not follow a very strict protocol but decide on a case-to-case basis whether to omit or complete ALND in patients with less than 3 SLNs removed or absent post-treatment changes. Multidisciplinary input is essential to decide whether additional treatment is needed in these patients.
The study allowed analysis of a single-center practice with many years of experience in the SLNB technique. Despite the relatively small number of patients included, this study adds to the short list of available studies on prognostic information for SLNB only after NAST in patients with cN + disease. To our knowledge, this is the first study to compare the oncologic outcomes of patients with cN + disease who convert to ycN0 and undergo SLNB only between patients with absent and present post-treatment changes in SLNs.

留言 (0)