
Remember me
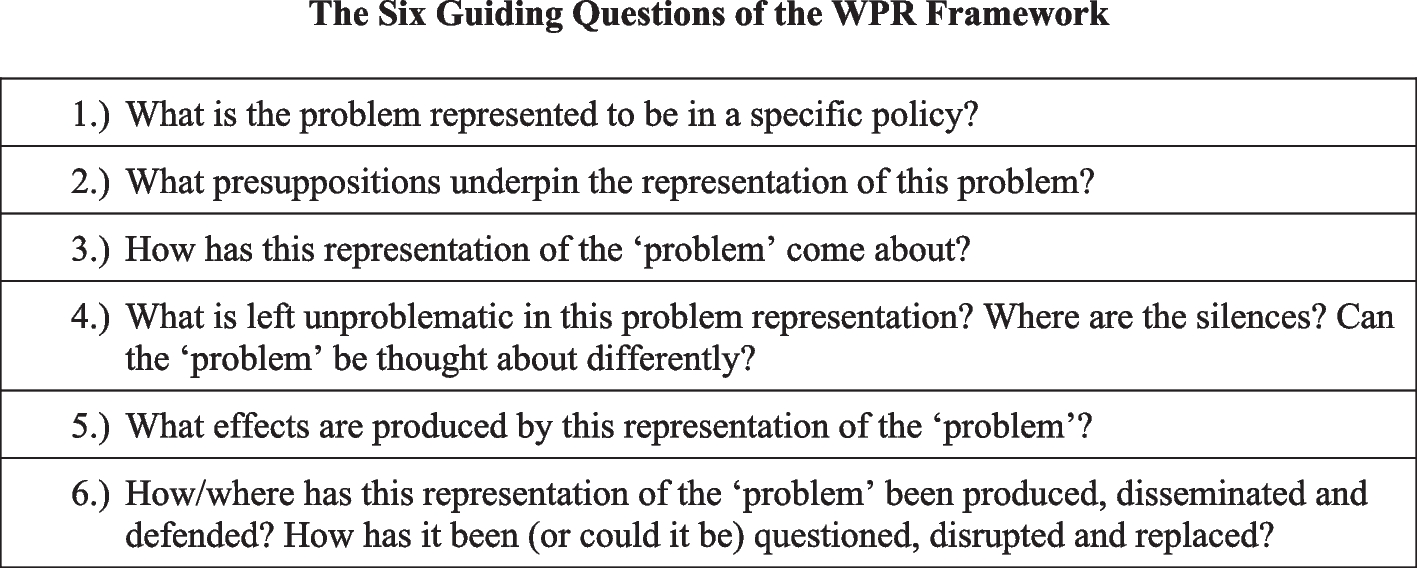


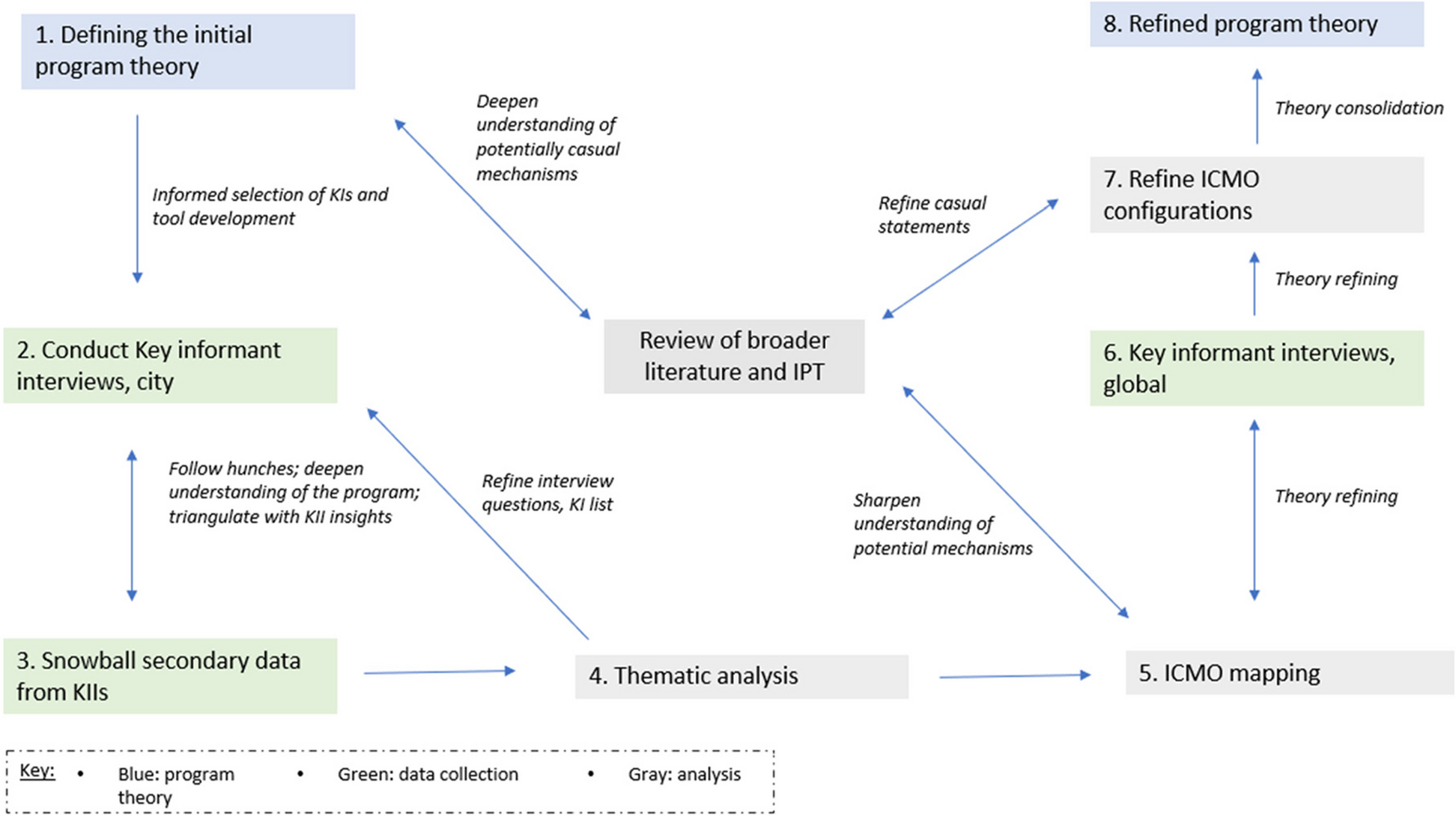

We sought to identify the key factors shaping global priority for children’s care, especially those internal to the community of children’s care proponents. Problem definition disagreements surrounding DI among children’s care proponents is a central challenge to advancing global priority for children’s care. We first discuss this challenge, identifying—through analysis of the data—three distinct perspectives: pro-DI, progressive realization DI, and DI-critical. These distinct perspectives differed in their definition of an institution, what DI encompasses, and the strategy’s legitimacy. We then identify the factors that have shaped children’s care proponent disagreements. We end by identifying two consequences of problem definition disagreement: ineffective governance and unconvincing framing of the problem, both of which have further hampered global advancement of addressing children’s care. Figure 1 summarizes the core beliefs held by three groups of children’s care proponents, the factors shaping perspective differences, and the impact of these divisions on proponent efforts to advance global attention.
Fig. 1
Problem definition disagreements, factors shaping perspective differences & their impact on proponent efforts to advance children’s care
Problem definition disagreementFindings reveal divisive disagreements among children’s care proponents surrounding deinstitutionalization (hereafter referred to as DI) as a strategy, which are underpinned by disagreements on what DI encompasses, the appropriateness of various forms of non-family-based care, and which forms ought to be labeled ‘institutional’ in nature—a term with negative connotations. Children’s care proponents fall into three groups on the issue of DI, which we term pro-DI, progressive realization DI, and DI-critical. Pro-DI proponents view nearly all non-family-based forms of care to be unacceptable, consider most of these forms to be institutional in nature, and call for the closure of even small-scale facilities and orphanages. Respondents identify Disability Rights International as the organization most aligned with this perspective (I1, I10, I13, I14, I24, I25, I29, I30). Others supporting DI call for a progressive realization approach—with children in families and family-based care as the end goal, but recognizing the need for some forms of residential care in the interim and/or at the margins of the continuum of care. Some view quality, small group congregate care as part of the long-term solution (I1, I10, I14, I29, I30). Those supporting progressive realization include Better Care Network, Lumos Foundation, Hope and Homes, USAID, and the Lancet Institutional Care Reform Commission Group. DI critics (themselves holding varying views concerning what ‘DI’ refers to) view the strategy as lacking nuance and therefore inappropriate, and perceive the need for continuing care arrangements of multiple forms. They see the need for ongoing non-family-based care arrangements when other alternatives are not available, and do not designate all these arrangements as institutional in nature. Respondents identify SOS Children’s Villages International, Whole Child International, Family for Every Child and a small group of academics as embracing this perspective (I1, I7, I8, I10, I14, I18, I20, I25, I27). The organizational histories and locales of key informants informed their adoption of these positions. For instance those working in organizations focused on former Soviet Union states were more likely to have embraced DI, as well as disability organizations given neglect of that group of children and their placement into facilities. In contrast, individuals working in organizations more focused on other parts of the world are less wedded to DI, as they are likely to have observed a diversity of circumstances of children.
Despite differences, nearly all care proponents agree that family-based care is ideal and that very large residential facilities are poor options and should be closed. Momentum to address these differences has accelerated, in part due to children’s care problems exacerbated by the COVID-19 pandemic (I31). A Lancet Commission on Children’s Care helped bridge disagreements, [26] as did a 2019 United Nations General Assembly Resolution on the Rights of the Child, which contained provisions on children without parental care (I3, I14, I29, I30) [58]. In the latter, a coalition of 256 organizations working on children’s care agreed on the need to strengthen children’s care in families, prevent unnecessary separation by addressing its root causes, tackle orphanage volunteering, and put an end to institutionalization by progressively replacing it with family and community-based care. Yet proponents note this agreement did not bridge all differences. One commented:
Many of us in the middle were very frustrated…There is a coming together of minds, but you are not hearing it in these debates (I30).
Another respondent points to the effects of ongoing divisions:
We are bogged down on these technical issues and as a result we’re unable to actually think strategically about…the fundamental issue of how we ensure care for children (I29).
Differences on the definition of ‘institution’Differences concerning what constitutes institutional care shape childcare reform debates. The UN Guidelines for the Alternative Care of Children [6] distinguish between ‘institutions’—a term that appears only once in the document—and residential facilities. Residential facilities encompass all alternative care settings that are not family-based (including those that are categorized as ‘family-like’— another term that provokes disagreement) from emergency shelters and small group homes to the biggest residential facilities. The term ‘institutions’ is often reserved only for large residential facilities. However, there is no universally agreed understanding—in the Guidelines or among care proponents—of what constitutes an ‘institution’ as opposed to other kinds of residential care settings, and the terms are used inconsistently among care sector proponents (I3, I9, I25, I27).
These definitional differences have shaped proponent disagreements surrounding which residential care arrangements are institutional in nature and therefore an unacceptable option for children’s care (I2, I5, I7, I8-I10). These include emergency shelters, children’s homes, small group homes, and children’s villages. Those holding pro-DI perspectives find any care arrangements that are not family-based to be institutional in nature (I1, I12, I23, I24):
They are just mini-institutions and no child should be in a small group home. Every child should be in a family (I1).
In contrast, those critical of DI generally consider some arrangements that are not family-based care to constitute residential or family-like care approaches [17, 59]. One respondent noted:
Residential care does not by definition have to be institutional…Most people when they think of residential care they think of the Romanian orphanages. That of course is terrible…and there is no reason for that. The same structure can be restructured to feel like a home (I15).
Differences on the definition and legitimacy of the DI approachThese disagreements about what constitutes an institution underpin the most divisive debate: whether DI is an appropriate entry point for care reforms, and what DI actually encompasses.
Arguments by those who identify as pro or progressive realization ‘DI’Pro-DI proponents believe that facilities that institutionalize children are unable to guarantee the well-being of children and deprive children of their right to a family. In advancing their perspective, proponents make several arguments.
Pro-DI proponents argue that facilities that institutionalize children have long-term harmful effects on child well-being, and often apply the findings to all forms of care that are not family-based (I1, I3, I4, I12, I21,I23). The literature that supports this claim is sizeable and dates back to the mid-20th century. Studies have found that institutionalized children, in comparison to their peers, are atypically short, low IQ, and low self-esteem [60,61,62]. Many DI proponents point to the Bucharest Early Intervention Project (BEIP), [63] a randomized-controlled trial comparing longitudinal outcomes among young institutionalized children, which offered strong evidence that institutional care has a causal effect on developmental deficits and delays. This finding has since been substantiated by other works [64]. Furthermore, there is evidence that the harmful effects of institutionalization are not limited to large institutions. Children in small-group care—such as SOS Children’s Villages—have substantial development delays as compared with their peers in family care [65, 66]. One respondent pointed to the strength of the scientific evidence:
The science is…pretty clear that you know, a child needs a family (I1).
Others expressed concerns about the lack of scientific rigor in research supporting claims that residential care is comparable to the care received in family-based arrangements (I23, I29):
[There is] dangerous research [conducted by a] minority that is academically questionable saying that the clean institutions and residential care and group homes are just as good as foster care…. There is a very serious misunderstanding of science out there…They are not paying attention to the greater amount of science that shows that residential care and group homes are dangerous, and the children need to be with families (I23).
Another DI argument is that institutionalization is not cost-effective and diverts resources from preventing family separation and strengthening families (I1, I12, I14). Research from the United States, for instance, indicates that group placements cost seven to ten times the cost of placing a child with a family [67]. One DI proponent made the additional point that:
The more we continue to pour resources into improving institutions, the less resources [there are] for helping families take care of their children (I7).
DI proponents also point to evidence on the heightened risk to institutionalized children of neglect and abuse from caregivers and peers [68,69,70,71,72]. For example, a Romanian study found that 38% of 7 to 18-year-olds in residential care reported severe punishments or beatings [73]. In addition, DI proponents point to the social and psychological harm, especially in terms of attachment, that institutionalized children experience given the constant overturn of volunteers in such facilities, and the involvement of untrained and non-certified caregivers [74].
In addition, DI proponents note that approximately 80–90% of the millions of children living in orphanages have at least one living parent [74, 75]. Accordingly, proponents argue that DI is critical to reintegrating these children back into their biological families, with support services to strengthen a family’s capacity to care [76].
Arguments by those who identify as DI-criticalThose who identity as DI-critical question the quality of the evidence that purports to show that all forms of care that are not family-based have more pronounced adverse effects on children than those that are family-based (I11, I14, I16, I19, I21, I25) [77]. They express concern (I10, I16, I18) [78] that analyses examining the effects of care arrangements that are not family-based on child well-being have focused largely on large hospital-style facilities caring for infants with shift workers, and that studies providing evidence on the harmful consequences of care arrangements that are not family-based are based predominantly on the experiences of states in the former Soviet bloc [79, 80]. Critics also express concern about design and methodological problems in studies of care arrangements that are not family-based [81]. One respondent noted his frustration with the body of literature that claims any care arrangement that is not family-based is universally detrimental:
Nobody seems ever to take account of the trauma [children have] been through before placement in care…The very fact they’re in care indicates that some degree of pre-care trauma has taken place (I27).
Critics also note evidence that family-based care can have adverse effects. A number of studies highlight that vulnerable and orphaned children are often exposed to significant levels of violence and abuse within extended-family care settings [82]. Critics note also that in some instances outcomes for children in care arrangements that are not family-based may be equal or better than those for their counterparts living in kinship care arrangements on outcomes pertaining to child rights, [83] nutritional status, [84] and mental health [85].
DI critics argue that more nuanced approaches tailored to context are needed (I10, I11, I14, I19, I25). They object to DI’s universal approach, concerned that it is too narrow a goal:
I really don’t think we can do black and white, especially when it comes to children. And if we do black and white that all children have to be in a family…then we’re not doing what the [UN Guidelines] say and the guidelines really ask us for an individualized approach for every child (I19).
Critics worry also about consequences for children in various care facilities when these are shut down (I9, I10, I11, I14, I15, I18, I25). There is concern that donor-led strategies have imposed unrealistic goals for DI implementation:
[There] has been a pressure on the countries to close institutions without having a clear roadmap for what should be there instead, and sometimes it’s done too hastily and without good, proper assessment for each individual child (I25).
Those concerned with the current DI approach also point to the fact that not all biological parents or extended families are capable of or have a desire to care for their children:
So you get other bold statements like: ‘A large majority of children living in institutions have one living parent or existing family.’ So what? That says nothing about the willingness, ability or capability of those people to be the caregiver. If they’re not willing, it doesn’t matter if they’re alive (I27).
Critics contend that more attention should be given to the “quality of care provided within a setting, whether that setting be family-based or institution-based,” rather than eliminating all forms of care that is not family-based [78].
Factors shaping disagreements on deinstitutionalization as a strategyAside from differences on what DI actually entails, several additional factors have shaped care proponent disagreements on the legitimacy of DI as a strategy, and global priority for the issue of children’s care.
Data inadequaciesInsufficient data on the scope and nature of the problem have intensified proponent differences (I2-I4, I6, I8, I12-I14, I21, I26, I27):
How many [orphanages] are unlicensed? We don’t know. Number in children care? We don’t know. Number of economic orphans versus orphans? We don’t know (I11).
While efforts exist to improve data collection, [62, 64] difficulties persist in detecting the number of vulnerable and orphaned children. Divergent perspectives on the definition of ‘orphan’ and its usefulness as a designation shape these difficulties, [86] as does the dearth of accessible data from household surveys on children living outside of family care. With the exception of a few scattered estimates from a handful of countries and emergent efforts to better use household survey data, [87,88,89] vulnerable children are “largely falling off the statistical map” [90].
Contradictory evidence on solutionsA sometimes conflicting evidence base on solutions also leads to proponent differences. This is underpinned by the fact that robust impact measures for a number of areas of child well-being are not available, and ‘quality of care’ is a difficult concept to measure. Few longitudinal studies follow cohorts of children, especially in LMICs [59]. Those studies that do exist present contradictory results on the effects on children of small group homes versus other care arrangements [65, 66, 91, 92]. Yet another problem is that many of the studies examining care arrangements and interventions are based on experiences of former Soviet bloc countries [79, 80, 93]. One respondent noted:
You can’t prove the points to policymakers without the data (I27).
Divergent experiences between former Soviet bloc and other countriesDivergent experiences between former Soviet bloc and other countries have also fueled DI disagreements. Many with experience in the former tend to favor a strong DI approach given the history of child maltreatment in large-scale institutions in these countries. Many of those who support DI were moved by the horrifying images that surfaced in the 1990s of thousands of neglected children housed in overcrowded, state-run orphanages in Romania and other Eastern European countries (I9, I11, I18). One respondent notes that Lumos and Hope and Homes, for instance, both arose out of the Romanian experience (I18).
DI critics, in contrast, argue for a more nuanced approach given experiences with different child demographics and care arrangements that are more typical in the rest of the world. In low-income countries, children on average are considerably older than those of former Soviet bloc countries, as access to basic services and education drives children home placement. The majority of children living in alternative care across Sub-Saharan Africa are in family-based arrangements—living with a surviving parent, grandparent, or other family member [17, 94, 95].
Furthermore, there are differences in the way that existing care systems are organized. Highly centralized and government-regulated systems—which is more amenable to a DI approach—are common among post-Soviet countries. In contrast, decentralized and poorly regulated systems often characterize low-income countries, where private and often faith-based organizations dominate the landscape (I29, I30). One DI-critical respondent expressed frustration about the lack of recognition of the different realities:
The evidence that isn’t being absorbed by the DI community is that this whole DI movement started out as the former Soviet Union with large state-run institutions… But the profile of the child in care worldwide is very different than that reality (I18).
Challenges in introducing formal alternative care arrangementsThe lack of social protection and legal systems and capacity to implement formal alternative care arrangements in many low-income settings lead some proponents to question the feasibility of DI as a strategy. While many countries have made efforts to establish legal and statutory frameworks for childcare reforms, the implementation of these laws has been challenging, given the lack of financial resources, inadequately qualified staff, and poor service provision. In Uruguay and Guatemala, police, rather than social workers, assess protection risks and make most referrals. Cultural, religious, and social resistance to certain alternative care arrangements also exist. In a number of countries alternatives such as domestic foster care or adoption are resisted because of unease with the idea of families raising another person’s child [23]. In most African countries, formal adoption is rare. One respondent describes the problem this way:
Foster care, development of small group homes, development of domestic adoption have all been proposed…we’re asking other countries to develop a whole type of profession …not necessarily something that naturally comes out of their own country environment. So, it can feel like an imposed solution (I8).
Commercial interestsThe fact that individuals and organizations profit from institutional care and therefore have an interest in sustaining their existence also fuels disagreements on DI as a strategy. DI proponents argue that this phenomenon heightens the need for their closure:
If you don’t close the institutions, the places will be filled with new children. Without strong gatekeeping and actually closing them, you will have new children coming in (I25).
Others, while acknowledging these interests, believe that DI proponents use these as an excuse to promote an uncompromising position.
Few in the children’s care community deny that commercial interests shape the persistence of residential care (I4, I8, I25). Employees of residential facilities fear losing their jobs. Poor families, often seeking better education or health for their children, are sometimes pushed by orphanages engaged in intercountry adoption or residential facility managers driven by profit into giving up their children. Some parents do not understand the legal implications of adoption, signing papers without understanding that the provision is permanent [96]. Orphanage tourism—fueled by foreigner desires during their travels to help local children—motivates operators to set up new residential facilities and to use illicit practices to recruit clients [97,98,99,100]. Strong business interests make residential care facilities hard to close. Furthermore, government officials often support these facilities:
Government officials often have significant investments in orphanage care because it’s a lucrative business model for them (I18).
While acknowledging this reality, one respondent expressed frustration about how some DI proponents exaggerate the pernicious nature of profit-making in these facilities:
I’m not saying that never happens, but you cannot generalize globally that …the only reason why children are in child protection systems is because evil people who run orphanages want to make money (I15).
Perspectives of children, families and the disability communityTensions about the acceptability of residential care have also been shaped by the perspectives of two historically under-represented groups in childcare reform debates: the children and families directly affected by care reform, and the disability community.
Children and young people themselves sometimes express a preference for residential over family-based care alternatives (I2, I11, I14, I19, I21, I28). This was found to be particularly true for teenagers who are at the stage where “the idea of having a family is not the most important thing” or for children who have already been through multiple foster placements that have failed (I2, I21). HIV positive children have also reported benefiting from important protective factors. These include a sense of belonging and appreciation for community, and gaining the resilience for coping with challenges such as stigma [101]. Practitioners working with young, unaccompanied migrants stress that:
It is really important to keep that menu of [care] options really open, be really conscious about what profiles may be more appropriate for certain types of care, really listening to the children themselves (I28).
On the other hand, most disability rights groups strongly support the DI agenda. They point to numerous declarations that advance the right of children with disabilities to live with their families, including the Convention on the Rights of Persons with Disabilities [102]. In 2017, the Committee on the Rights of Persons with Disabilities advanced the right of a child to grow up in a family, finding institutions—regardless of quality or size—to be unacceptable alternatives.
Disability Rights International (DRI) and partner organizations subsequently called for the UN General Assembly to include in its Resolution on the Rights of Children a recognition that there are “no exceptions to the right to grow up in a family for any child, and the provision of care never justifies the denial of this right”. While some care reform proponents sympathize with the concerns expressed by disability rights advocates, others express frustration with claims that residential care is akin to encroaching on a child’s human rights:
The problem is that they are mixing up dogmatic rights and justified claims…They’re saying basically that putting a child in a residential care home is tantamount to violating that child’s rights. And it’s not (I13).
Consequences of problem definition disagreementDifficulties with problem definition have hindered the ability of the children’s care community to address strategic challenges concerning governance and positioning.
Weak governanceProponents identify numerous fault lines that hamper the establishment of effective governance arrangements for the children’s care community, ones that could enable actors in the sector to more effectively work together. The primary fault line is grounded in the problem definition difficulties pertaining to DI strategy. As one respondent puts it:
There [are] differences of opinion about what it is we’re arguing for and what the solutions are that we’re putting forward, which preoccupy us as a community…[and] stops us from being very cohesive (I8).
Proponents identify additional fault lines based on organizational focus and type; for example, between organizations largely active in and drawing on experiences in Eastern Europe and those focused on care reform in Sub-Saharan Africa and Asia (I9).
Proponents note that fragmentation is driven not just by differences over ideas, but also by turf. Respondents identify power struggles, with contention over control of the childcare reform agenda and desires to gain credit for contributions (I4, I5, I6, I7, I9, I11, I18, I21, I27). Respondents express concern over the uncomfortable environment in the children’s care sector that has emerged (I2, I5, I10, I11, I15, I25):
Organizations are trying to shut each other up rather than having a proper conversation (I2).
The ideology becomes a battering ram…If you’re not on board, you are an outcast. If you’re not singing from the hymnal, you’re excommunicated from the community (I20).
Proponents perceive the sector’s lack of resources to have contributed to competition (I2, I3, I5, I7, I12, I13, I27), resulting in organizations becoming “connected with their model” and unable to “step back and look at these issues free of their organizational needs” (I3). Effective leaders—individual and institutional—might help in transcending these challenges, but respondents note a dearth of unifying champions for childcare reform (I3, I6, I9, I13, I18).
Governance challenges include difficulties with coalition-building with the variety of sectors shaping children’s care, including education, child protection, health and justice (I2, I5, I8, 19, I14, I19, I24, I26, I28). One proponent expressed frustration that:
The very sectors and actors that need to be at the table to actually create the reforms we need aren’t there… And so it’s like we’ve got our eyes on the symptoms, not on the root causes (I5).
Some note disinterest or active resistance by these sectors in connecting their issues to children’s care because of resource constraints, bureaucratic red tape, or lack of awareness of how their issue relates.
The greatest lost opportunity proponents note has been the inability to capitalize on the recent surge in attention for addressing violence against children (VAC) (I2, I3, I5, I8, I9, I12, I14, I21, I25). Despite some efforts to advance linkages with the VAC sector, [103, 104] some children’s care proponents believed that they themselves were in part to blame for not collecting evidence to foster collaboration (I9). Others blame VAC sector actors for this disconnect, perceiving them to have “elbowed care issues out of the way” in their attempts to bring their issue prominence in the SDG discussions (I2).
Unconvincing positioningDifferences surrounding problem definition have made it difficult for care proponents to address the challenge of positioning: advancing a clear case that motivates policy-makers and civil society groups to act. Divergent approaches to childcare reform lead to policy-maker confusion concerning what they are being asked to do (I9, I18, I21, I29). Respondents note that care reform proponents lack a “collective elevator speech” (I18). Respondents express concern that the terminology actors in the sector use —such as institution and alternative care—is ambiguous and complex (I3, I9, I25).
As long as we can’t define what an institution is and what it looks like, it makes it hard to then advocate for governments not to support it (I9).
One of the difficulties with making the case for children’s care are misperceptions individuals have about orphanhood being the problem (I29) and the best way to support orphans. These misperceptions encourage the institutionalization of children and orphanage volunteerism. It is difficult to redirect an individual’s well-meaning support of orphanages via volunteering, donations, and faith-based mission work to support efforts to help strengthen and unify families. One respondent noted the difficulties in striking a balance in messaging that combats these public misperceptions, but that also does not deter the public from supporting children’s care all together:
How do we nuance the message so that you can say: ‘Yes eager person wanting
Comments (0)