
記住我

Cerebral palsy (CP) is a lifelong disability causing disruption to movement, posture, and balance, and variable delay in the development of gross motor skills and functional mobility.1 It is characterized by a permanent injury to the developing brain during infancy, but its effects are ever changing throughout growth and development.1 Cerebral palsy movement patterns are influenced by the area of the brain affected, which can be described as spastic (stiffness), dyskinetic (uncontrollable movements), ataxic (poor coordination and balance), or a mixed presentation.2 The motor disability in CP can be accompanied by impairments in cognition, social skills, and sensory systems.1 Cerebral palsy is the most common physical disability in childhood, with an overall prevalence of 2.11 per 1000 live births worldwide.3 Bilateral CP, with both sides of the body affected, comprises approximately 60% of the CP population.2 The predominant motor type for children with bilateral CP is spasticity. This review includes young children with CP with any of the motor types.
Longitudinal studies of children with CP support that gross motor development and mobility skills are rapidly developing during the first 5 years of life.4 This makes early childhood an important period to maximize gross motor development and functional mobility while capitalizing on the potential that exists during the early years of life.5
Traditional therapeutic interventions aimed at improving gross motor function and mobility have used a facilitated approach dominated by passive handling and positioning6; however, there is limited evidence that these approaches are effective at improving gross motor development and mobility.6 Instead, there is emerging evidence to support active motor learning interventions to promote motor development in children with CP.6 Active motor learning principles allow the child to explore the environment with minimal handling or facilitation.7 Self-generated movement and muscle activation is encouraged through play and equipment/toy placement to encourage successful attempts at new movements and positions.8,9 Active motor learning interventions aiming to improve gross motor function include approaches such as goal-directed training, task-based training, context-focused therapy, action observation training, functional therapy, and bimanual training.6
PURPOSEChildren with bilateral CP represent more than half of all childhood CP diagnoses, making this cohort an important target group for understanding how therapeutic intervention can help to improve gross motor function and functional mobility.1 A number of studies looking predominately at children with unilateral CP have demonstrated efficacy for active motor learning interventions to improve gross motor function in older children (>6 years) and infants (<2 years) with CP.6,8 To date, the efficacy of motor learning-based interventions to improve gross motor development and functional mobility for younger children (2-6 years) with bilateral CP has not been systematically reviewed.
This study aimed to systematically review the efficacy of active motor learning interventions to improve gross motor development and functional mobility for children with bilateral CP between the ages of 2 and 6 years.
METHODSPreferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed in performing this review.10 The protocol for this systematic review was registered with PROSPERO (CRD42020195981). Deviations from the protocol include not restricting the search to English language articles and including a search on gray literature. Ethical approval was not required.
PICOThe Population, Intervention, Comparison, Outcome (PICO) question was as follows: for children aged between 2 and 6 years with bilateral CP (P), which active motor learning interventions (I), compared with usual care or other movement-based interventions (C), improve gross motor development and/or functional mobility (O)?
SEARCH STRATEGYAn initial search of the following databases—PubMed, Cochrane, MEDLINE, CINAHL, and EMBASE—was completed on January 27, 2020, by the first author (K.M.). Articles were included from database inception to the search date. The search was supplemented by manually searching reference lists and bibliographies of the included studies. Consultation with experts in the field of pediatric motor learning for CP was explored at the time of the initial search and revealed 1 additional study, which met the inclusion criteria. The search was updated using identical terms with the same databases on October 20, 2021 (from the initial search date). An additional search of gray literature was completed on May 3, 2022, which included the following databases: Scopus, Web of Science, Proquest, Clinicaltrials.gov, and World Health Organization International Clinical Trials Registry Platform (WHO ICTRP). This search yielded 1 study, which met the inclusion criteria. No language restrictions were applied to the search terms. A comprehensive search of all databases was rerun on January 4, 2023, using the same search strategy. The full search strategy can be found in Supplemental Digital Content 1 (available at: https://links.lww.com/PPT/A480). Medical Subject Headings (MeSH) terms and key words relevant to cerebral palsy, bilateral, children, active motor learning, and movement-based interventions were used to search each database. The study flow diagram (see Supplemental Digital Content 2, available at: https://links.lww.com/PPT/A481) includes pooled results obtained from all search dates. The search strategy was restricted to randomized controlled trials (RCTs) only. RCTs are considered the highest level of evidence in research.11 This decision was made to increase the quality of the evidence as well as improve the certainty of recommendations for the included articles. A list of potentially relevant studies with the reason for their exclusion can be found in Supplemental Digital Content 3 (available at: https://links.lww.com/PPT/A482).
SELECTION CRITERIATo be eligible for inclusion, the study (a) was an RCT; (b) included a population of children with bilateral CP, with a mean age between 2 and 6 years; (c) evaluated the effects of active motor learning-based intervention (with a primary aim for the child to develop their gross motor skills and coordination to perform everyday movement and tasks). Active motor learning was defined as the child actively performing/participating in the therapeutic activities with minimal physical assistance or facilitation by either parent/therapist or device/garment/equipment (equipments such as a walker or bicycle were allowed if they were required to perform the goal); however, supportive equipments such as devices or garments that were the focus of the study intervention were excluded (ie, compression garments to improve sitting ability); (d) intervention was compared to a control group or other active movement-based intervention; and (e) outcomes measured gross motor capacity and functional mobility. Studies were excluded if the experimental intervention used adjunct therapies, passive facilitation, passive participation, supportive equipment or garments or devices, pharmacological adjuncts, and/or neuromuscular stimulation.
Selection of Studies and Data ExtractionEach step of the study selection process was completed using Covidence (Veritas Health Innovation, Melbourne, Australia, www.covidence.org) by 2 independent reviewers, with a third reviewer introduced to resolve conflicts as required. Studies were screened initially by title and abstract. Abstracts meeting inclusion criteria or requiring the full text to determine inclusion were retained. Full-text articles were included when reviewers achieved 100% agreement after consensus discussion to resolve conflicts. Structured data extraction tables were developed including demographics (Gross Motor Function Classification Scale [GMFCS], age, number of participants, and percentage of participants with bilateral CP), intervention details (style, provider, setting, session duration, and number of sessions), and funding source.
Where not explicitly stated, percentage of bilateral CP was calculated based on the assumption that children classified in GMFCS levels III, IV, and V have bilateral involvement.12
Data extraction was completed by one author and cross checked by a second author and are in Supplemental Digital Content 4 (available at: https://links.lww.com/PPT/A483).
Quality of Studies and Risk of BiasThe Cochrane Risk of Bias 2.0 (RoB 2.0)13 tool was used to assess the quality of articles at the study level and the GRADE (Grading of Recommendations Assessment, Development and Evaluation)14 tool to rate the certainty of evidence at the outcome level. Two independent reviewers completed the ratings with a third reviewer introduced to resolve conflicts as required. The RoB 2.0 includes 5 domains: (1) randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported results and rating of studies as “low risk,” “some concern,” or “high risk.” A final score of overall bias is produced based on the 5 domain ratings. The GRADE approach was used to assess and rate the certainty of the body of evidence using factors that may increase or decrease the confidence in the synthesized findings including: number of studies, study design, risk of bias, the precision of the effect estimates, the consistency of the individual study results, how directly the evidence answers the questions of interest and the risk of publication, or reporting biases.14 The GRADE approach includes 5 domains to determine the quality of the evidence: risk of bias, imprecision, inconsistency, indirectness, and publication bias. Two independent reviewers considered the evidence with a third reviewer introduced to resolve conflicts. Reviewers rated the overall certainty of the quality of the evidence as very low, low, moderate, or high.
DATA ANALYSISQuantitative analyses were conducted using Review Manager 5.4.1.15 Meta-analyses were completed on intervention outcomes measuring gross motor capacity and mobility performance such as the Gross Motor Function Measure (GMFM) and the PEDI-FSS, mobility domain. Where possible, studies were pooled for random-effects meta-analyses immediately post-intervention and at longer term follow-up where available. Authors were contacted to obtain within-group change scores for bilateral CP participants only, and these were used in preference to end point data where possible. Two authors supplied additional data.16,17 One author included change score data in their results.18 Mean differences (MDs) or standardized mean differences (SMDs) and 95% confidence intervals (CIs) were calculated for continuous outcomes across trials. The P value threshold was set as P = .05. Differences of 0.2, 0.5, and 0.8 standard deviations are considered “small,” “medium,” and “large” effect sizes, respectively.19
Combining data for analysis was considered by selecting the key features of each study and grouping similar participant characteristics, intervention features, and outcome measures together for meta-analysis. For example, 2 studies comparing context-focused and child-focused interventions were grouped together for meta-analysis, as they are similar intervention and comparator groups with alike outcome measures. All other meta-analysis included an active motor therapy group compared with a usual therapy group with similar outcome measures.
Sensitivity analyses will be performed where possible to determine whether there is any difference in the effect size estimates with the removal of studies with high risk of bias.
Elements of InterventionThe international clinical practice guidelines for interventions to improve physical function for children and young people with CP provide 9 good practice recommendations and 4 evidence-based recommendations to guide therapists, families, and children with CP.20 To provide further insight into the results of the included studies, we evaluated elements of the research and control group interventions against these clinical good practice recommendations to illustrate how closely interventions aligned with the guidelines.
The clinical good practice recommendation items 1, 2, 3, 4, 5, 6, and 8 were relevant to research settings and were included in the analysis (see Supplemental Digital Content 5, available at: https://links.lww.com/PPT/A484. Items 7 and 9 were not included as they were not relevant to a defined, short-term research intervention, but rather were more suited to long-term therapy team relationships. The 4 evidence-based recommendations have not been included in this review.
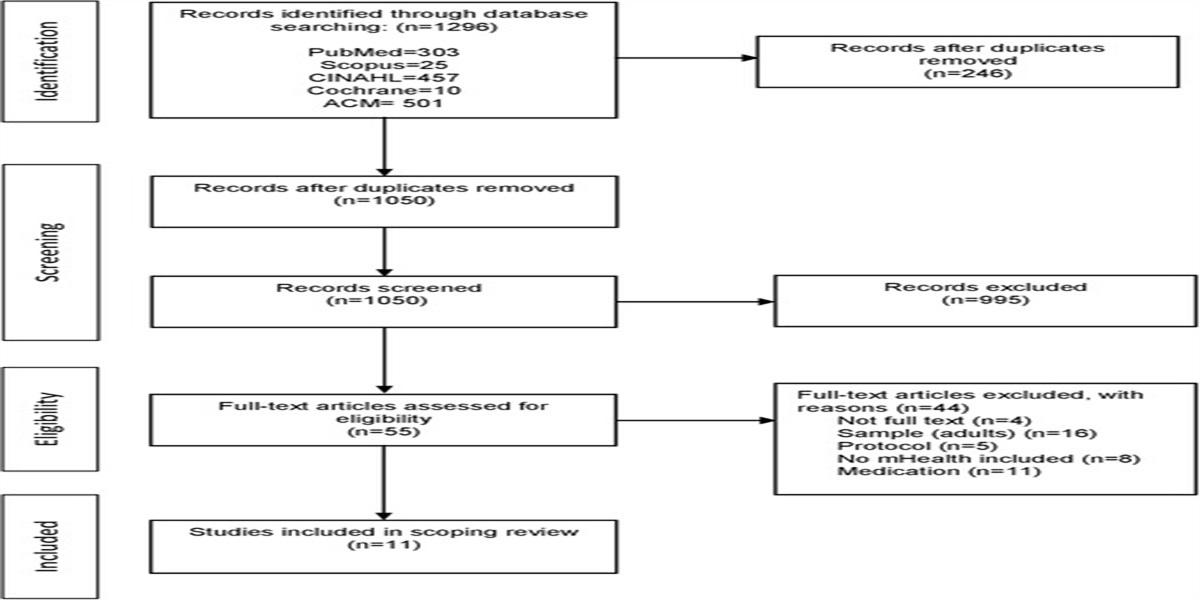
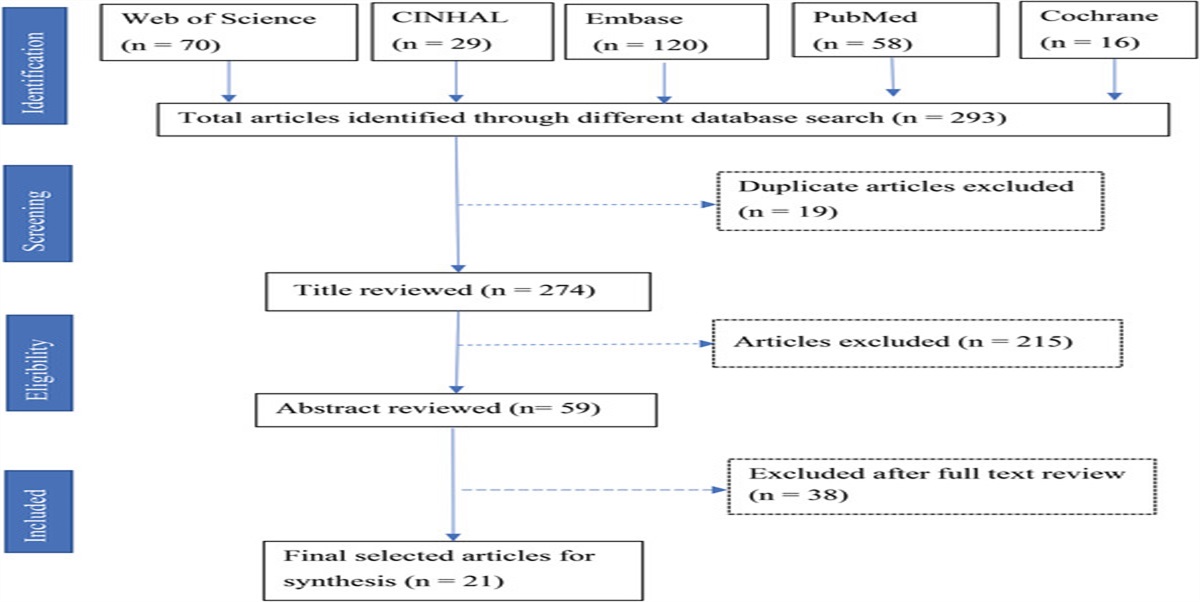
RESULTSThe results of the search and inclusion of studies are graphed in Supplemental Digital Content 2 (available at: https://links.lww.com/PPT/A481), the PRISMA flow diagram. A total of 5802 articles were identified with 3480 remaining after duplicates were removed. Following review of titles and abstracts, 89 articles remained for full-text review and a total of 7 articles met the inclusion criteria.
The 7 studies included a total of 332 children classified in all Gross Motor Functional Classification System (GMFCS) levels. Two studies comprised an entire sample of children with bilateral CP.21,22 Upon request 1 study18 provided end point and change score data and 2 studies16,17 provided change score data for bilateral CP participants only. These data have been used in place of the combined unilateral/bilateral participant data where possible. The variation of proportion of bilateral CP ranges from 51% to 89% for the 2 studies where only bilateral CP data were not obtainable.23,24 Two studies compared context-focused intervention with child-focused intervention.16,24 The context-focused intervention addressed functional task achievement via environmental modification and was considered the active motor learning group for the purposes of this study. The child-focused group addressed functional task achievement by identifying impairments and underlying functional limitations and providing therapy using physical handling as well as practice of functional activities and was considered the usual care group. Three studies described using a task-oriented approach to improve sitting posture and sit-to-stand transitions21,22,23 and 1 study looked at functional activities with a parent-led model.17 One study used goal-directed therapy to improve gross motor function including a home program.18 One study used action observation training to stimulate functional tasks and mobility.22 Four studies provided individual therapy in the home17,22 or clinic setting18,23 and 1 delivered the intervention in a small group in the clinic setting.21
The content for comparison groups was poorly described but typically focused on balance and mobility training, stretching and strengthening exercises, normalization of movement, neurodevelopmental therapy (NDT), Bobath, or Vojta methods.25,26
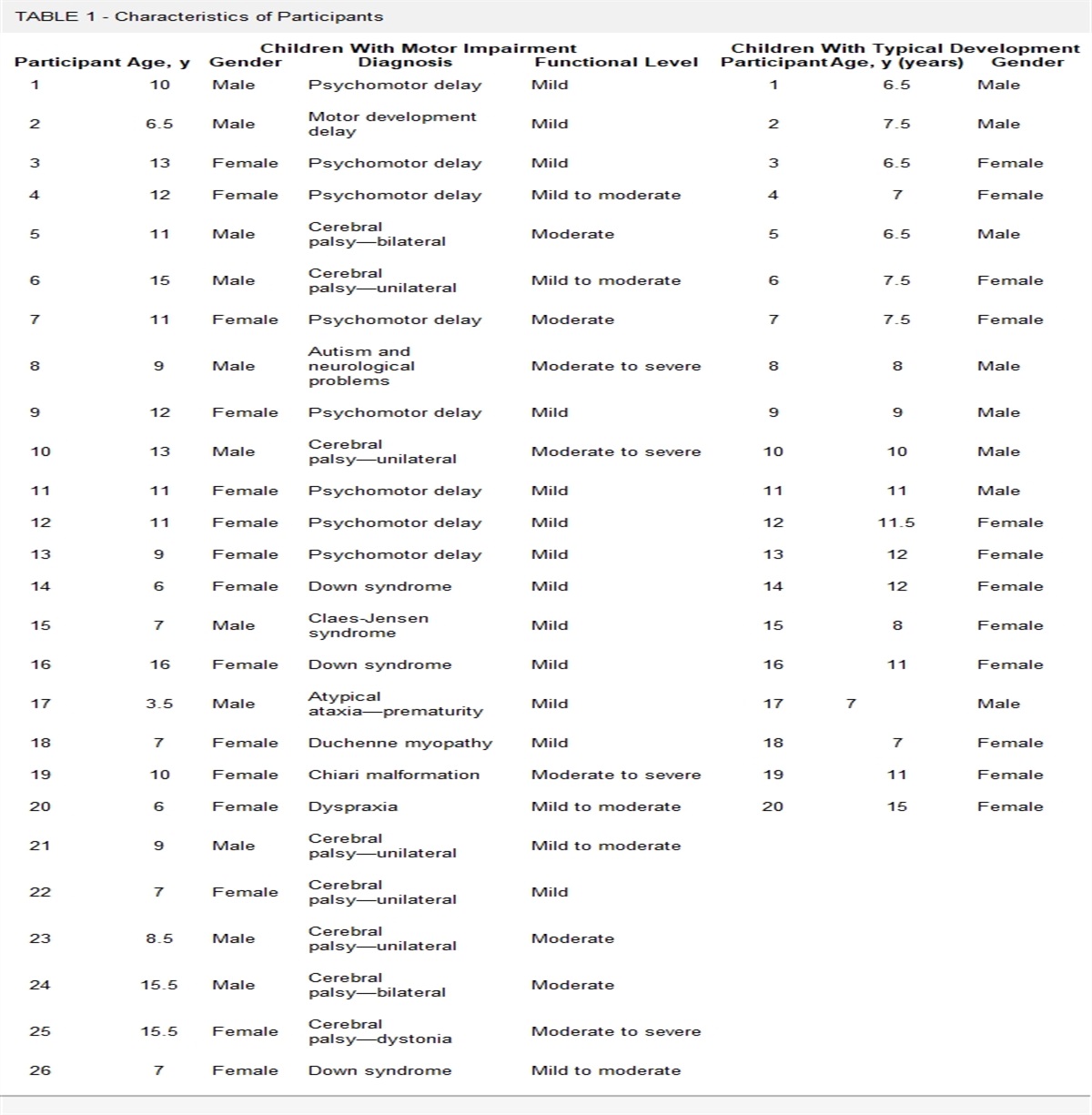
Table 1 provides study description and details of active therapy and usual care group content. Table 2 includes details of study design and demographics including sources of funding reported by authors.
TABLE 1 - Study Description Treatment Control Study Details of Therapy Provider/Setting Goals Determined Session Duration, min, Sessions/wk n, wk Home Program Details of Therapy Provider/Setting Goals Determined Session Duration, min, Sessions/wk n, wk Home Program Law et al24 Context-focused therapyChild-focused = body structure and function focus
Rehabilitation centerRehabilitation center
TherapistTherapist
Duration and frequency not known26
NRNR
Regular care = involves once or twice weekly physical and/or occupational therapy—30 min/session Rehabilitation center NR OT and/or PT 30 min 1-2 × weekAbbreviations: ADL, activities of daily living; NDT, neurodevelopmental therapy; NR, not recorded; OT, occupational therapist; PT, physical therapist; VCD, video compact disc.
Abbreviations: CP, cerebral palsy; GMFCS, Gross Motor Function Classification Scale; NDT, neurodevelopmental therapy; NR, not recorded; RCT, randomized controlled trial; VCD, video compact disc.
aWhere not explicitly stated, percentage of bilateral CP has been calculated based on the acceptance that GMFCS level III, IV and V as well as diplegia, quadriplegia and triplegia have bilateral involvement.12A summary of study results and calculated effect sizes is provided in Table 3. Effect sizes were calculated for each outcome in each study and found that out of 7 studies, 5 showed no significant difference for any of the outcomes. One study17 comparing active motor therapy to usual care showed a significant difference for the PEDI-FSS mobility outcome (combined end point data subgroup) and another study18 comparing active motor therapy to usual care showed a significant difference for the following outcomes across specific participant subgroups: GMFM-66 lying and rolling, GMFM-66 sitting domain, GMFM-66 crawling/kneeling, GMFM-66 standing domain, GMFM-66 walking/running/jumping, and GMFM-66 total score.
TABLE 3 - Data Extractiona Study Outcome Measure Timing, mo Intervention
留言 (0)