
記住我

The study protocol was approved by the Research Ethics Committee of Southwest University (No. H21034). The study was carried out in compliance with the most recent iteration of the Helsinki Declaration and adhered to all other stipulations outlined by the local legislation of China. The participants were recruited from local hospitals, the university campus, and communities in Chongqing, China. Based on the results of a recently published pilot RCT examining MBSR effects on migraine [29], a minimal sample size of 60 participants was determined for a pilot RCT study. Written informed consent was obtained from all participants.
Eligibility for the study was assessed using an online screening questionnaire. Inclusion criteria were as follows: (1) willing and able to provide informed consent, (2) aged 18 to 65 years, (3) reported pain duration of at least for 3 months and painful days for at least 60 days within the past 3 months, (4) able to read and write in Chinese, (5) agreeing to complete homework if assigned to the treatment group, (6) meet the criteria for fMRI scanning. Meanwhile, exclusion criteria were: (1) no Internet access, (2) prior participation in any structured mindfulness training, (3) regular meditation practice (more than once per month), (4) unable or unwilling to commit to the prescribed amount of sessions and home practice, (5) concurrent enrollment in another study assessing a pharmacological or psychological treatment for chronic pain, (6) diagnosis of psychiatric disorder, (7) participants with pacemaker, metal implants, dentures, severe claustrophobia.
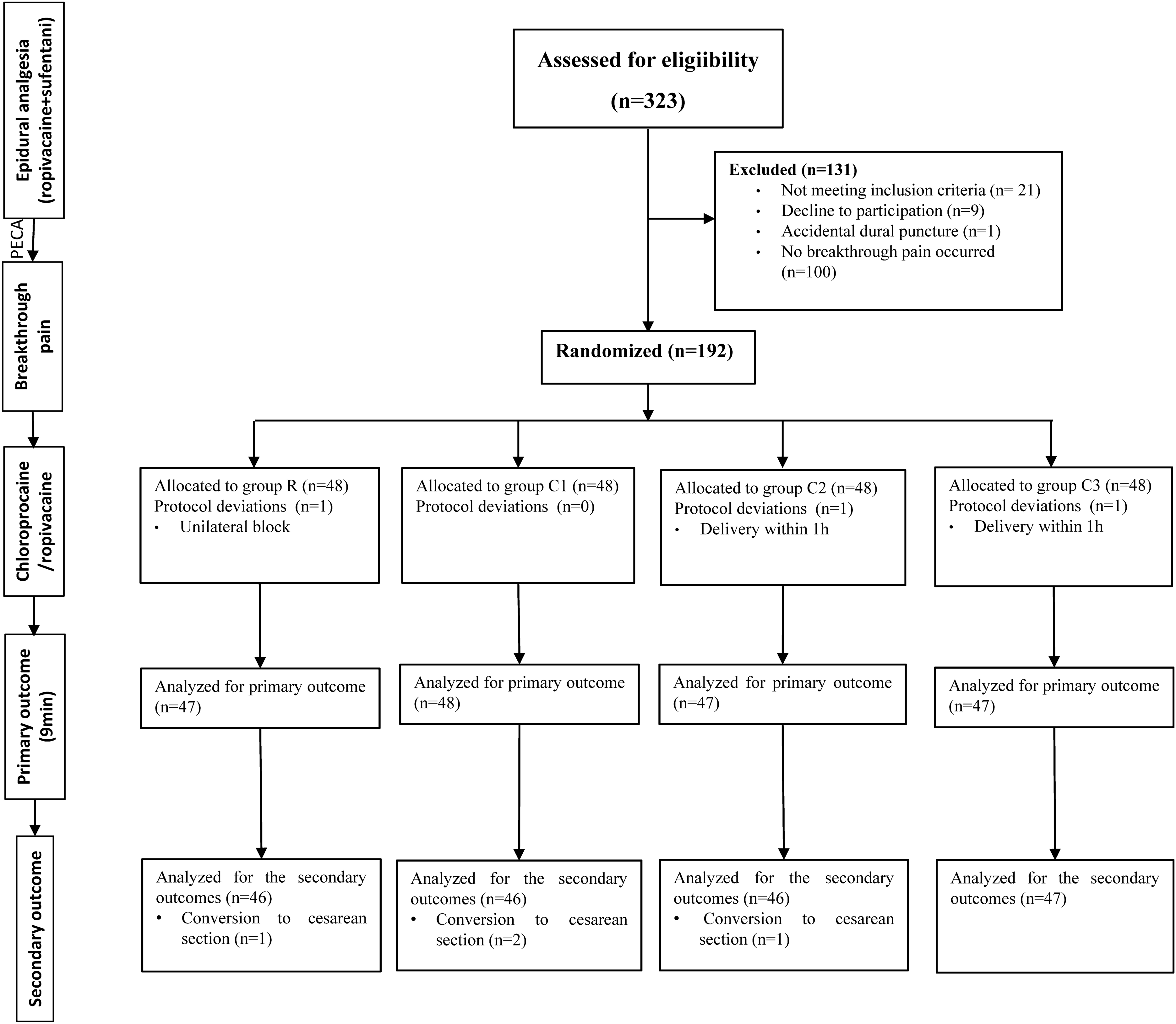
ProcedureRandomizationA CONSORT flow diagram is depicted in Fig. 1. Among the 139 patients assessed for eligibility, 89 were eligible and invited for the first assessment visit. Among the eligible participants, 22 declined to participate, leaving 67 eligible participants to be randomized in the study. The participants provided written consent, which outlined the vague purpose of the present study and assessment schedules. Of these, 40 were randomized to the mindfulness group (MBSR) and 27 were assigned to the treatment-as-usual group (TAU), according to a ratio of 1.5:1 between MBSR and TAU. This ratio was employed because the participants in the treatment group were more likely to drop out [30, 31]. Excel software was used to generate the random number, with a range of 0–1. Twenty-seven participants with the lowest sequence scores were assigned to the TAU and the remaining 40 participants were allocated to the MBSR group. Participants were given the chance to one of the three MBSR classes to attend, based on their schedule. Once they decided to attend the class at a particular time, they were not allowed to change the class throughout the treatment period. Finally, a total of three MBSR classes, with 9 to 16 participants per course, were conducted in the laboratory (Class 1, n = 15; Class 2, n = 9; Class 3, n = 16). It should be noted that five participants in the MBSR group did not attend any mindfulness courses but they participated in the online group discussion after classes, were available for mindfulness practice recordings, and completed self-report questionnaires at all three assessments (Fig. 1).
Fig. 1
Study flow diagram of participant randomization. MBSR mindfulness-based stress reduction, TAU treatment-as-usual, T1 baseline, T2 post-treatment, T3 3-month follow-up, ITT intention-to-treat, VBM voxel-based morphometry, fMRI functional magnetic resonance imaging
Modified Mindfulness-Based Stress Reduction ProgramThe modified MBSR training was conducted on the campus of Southwest University. Participants were instructed to continue their stable use of prescribed preventative treatments and continue taking acute abortives as needed. Considering the health conditions of the sample, we reduced the regular class duration from 2.5–3 h to 2–2.5 h. The separate groups for each intervention met for about 2.5 h for weeks 1 and 8 and 2 h weekly for weeks 2–7. One-day retreat practice was not conducted. Therefore, the total MBSR course duration was 17 h. Two instructors, certified as the MBSR teacher or under supervision, guided the MBSR courses in Chinese. In line with a manualized protocol that included participant handouts and materials for home use [8, 32], we also made several modifications based on characteristics of the current sample. For example, the people of Chongqing enjoy spicy foods, an almost painful sensation on the tongue. Savoring spicy foods in daily life could challenge the mindset that painful sensation is terrible and hateful. The outline of the modified MBSR course for Chinese adults with chronic pain is listed in the Electronic Supplementary Material (Table S1). Specifically, we focused on trauma-informed methods, disassociation among painful sensations, ruminative thoughts and sufferings, and emphasized loving kindness to distress and self-compassion.
Mindfulness practice sections in Class 1 were audio-recorded and transferred to written scripts, which were used by the junior instructor to guide Class 2 and Class 3 to increase the treatment fidelity. Of note, the mindfulness expert provided real-time online courses for weeks 5–7 because of health conditions that made it difficult to visit the laboratory during that period. A master-level student majoring in applied psychology assisted with the course and managed the online group community. Missed sessions were made up by sending the mindfulness practice audio that was recorded in class. Research staff conducting the assessments were blind to the study allocation.
Assessment ScheduleBaseline (Time [T]1), post-treatment (T2), and 3-month follow-up (T3) consisted of a battery of self-report questionnaires, which will be described in detail in the following section. The questionnaire took approximately 20–40 min to complete. All participants completed the written questionnaires at the T1 assessment during their visit to our laboratory. Those participants who were unavailable for the T2 and/or T3 visits completed the questionnaires online. In addition, participants attended the fMRI scanning at the T1 and T3 assessments, with 8 min allocated for acquiring resting-state brain activity and 6 min for collecting brain structure imaging. The imaging-acquisition procedure is described in detail in the Electronic Supplementary Material. Participants received minor compensation at each assessment.
Outcome MeasuresSelf-Report MeasuresThe Chronic Pain Grade (CPG) evaluates pain severity and pain interference across three items each [33]. Items measuring current pain, average pain, and most severe pain over the previous 3 months rated from 0 (no pain at all) to 10 (most severe pain). The pain interference tests how much the pain has interfered with daily activities, social activities, and work abilities rated from 0 (no interference) to 10 (unable to carry out activities/extreme change over the past 3 months). The subscale average scores were used. Previous investigations have validated CPG in Chinese chronic pain samples [15].
The 20-item Center for Epidemiologic Studies Depression (CES-D) scale was used for measuring depressive symptomatology [34]. Participants rated the frequency of each symptom throughout the previous week from 0 (rarely or never [less than 1 day]) to 3 (most or always [5–7 days]). The CES-D has been shown to be reliable and valid in Chinese adults with chronic pain [23].
Perceived positive and negative stress reactions were measured by the ten-item Perceived Stress Scale (PSS-10) [35] based on the original 14-item PSS [36]. In a sample of Chinese patients, a hierarchical two-factor PSS-10 structure outperformed the 14-item PSS and the four-item PSS in terms of overall psychometric qualities [35].
The 12-item Mindfulness Questionnaire (MQ-12) [37] was adopted from the 39-item FFMQ, which measures five aspects of mindfulness in its original form [38]. The MQ-12 evaluated three aspects of mindfulness: describing one’s experience, acting with awareness, and non-judgment of inner experience. Items are rated from 1 (very seldom true) to 5 (always true). A more proficient level was indicated by higher overall scores for each facet of mindfulness. The MQ-12 was validated in Chinese university students [37] and Chinese chronic pain individuals [23].
The 13-item Pain Catastrophizing Scale (PCS) measures a person’s propensity for pain catastrophizing, which includes feelings of helplessness, magnifying pain, and ruminating about it [39]. Scores for each PCS item range from 0 (not at all) to 4 (always). Previous studies showed that PCS has acceptable psychometrics among Chinese individuals with chronic pain [40].
The original 14-item Pain Resilience Scale (PRS) was used to assess a person’s capacity to successfully manage or adapt to pain [41]. Items are rated between 0 (never) and 4 (all the time), with higher total scores indicating more pain resilience. The 12-item PRS was optimal for Chinese adults with chronic musculoskeletal pain [16].
The six-item Brief Resilience Scale (BRS) was employed to assess one’s general capacity to bounce back from adversities [42]. In an initial validation study with four independent samples, the BRS was shown to have a unitary factor structure and strong convergent and discriminant validity [42]. Moreover, the BRS had good reliability in Chinese young adults [43].
Brain StructureGray matter volume (GMV) is an index of gray matter density defined as the product of cortical thickness and cortical surface area [44]. GMV changes could be as a function of genetics, aging, and pathology as well as in response to particular training [45]. The voxel-based morphometry (VBM) was employed to investigate focal differences in GMV [46].
Resting-State Brain ActivityThe amplitude of low-frequency fluctuation (ALFF), the fractional amplitude of low-frequency fluctuation (fALFF), and regional homogeneity (ReHo) were used to assess resting-state brain activity measured by functional magnetic resonance imaging (fMRI). ALFF refers to the averaged square root of power spectra within a low-frequency oscillation range (e.g., 0.01–0.1 Hz) from fast Fourier transformations [47]. The fALFF measures the ratio of fluctuations within the low-frequency band to the entire frequency range, providing information on relative amplitudes in low frequencies [48].
Demographic InformationWe collected information on participants’ age, gender, body mass index (BMI), the highest education level (1 [primary school or lower], 2 [middle school completion or partial completion], 3 [high school completion or partial completion], 4 [post-secondary education]), ethnicity, pain duration (months), primary pain site, prescribed analgesic usage, and presence or absence of pain every day in the past week.
Data AnalysesSelf-Report MeasuresAll statistical analyses were conducted in RStudio (version 1.2.5033; RStudio Team, 2019) based on the R programming environment (Version 3.6.3; R Core Team, 2019). Initially, independent samples t tests and chi-square tests were conducted to analyze baseline differences in patient characteristics between intervention groups. Mean scores at baseline (T1), post-treatment (T2), and 3-month follow-up (T3) were derived from linear mixed-effects models, which account for the within-subject correlation of responses over time and enable the use of all available data across all time points to increase statistical efficiency [49]. The intervention group and time point were treated as fixed effects. Group × Time interaction was assessed to determine whether participants randomized to MBSR differ from those randomized to TAU for change from T1 to T2, and from T1 to T3 on outcomes; the significance level is reported for the Group × Time interaction. Moreover, we reported the between-group effect sizes of change from T1 to T2, and from T1 to T3, as Cohen’s d (0.20 small; 0.50 medium; 0.80 large). We conducted intent-to-treat (ITT) analyses involving the entire randomized participants and “completer” analyses limiting the MBSR group who attended at least four sessions [50].
Imaging OutcomesImaging preprocessing is described in the Supplementary Materials. We included the sample of individuals who completed both T1 and T3 fMRI scanning with adequate data quality and participants in the MBSR group attended at least four treatment sessions. Initially, full factorial analysis was conducted on GMV via SPM. Then, the paired t test was performed on each group if the Group × Time interaction was significant. Age, gender, and total intracranial volume (TIV) were included as covariates for all GMV analyses per conventions of VBM [51]. Voxels with GMV values under 0.2 were excluded using absolute threshold masking. A threshold of p < 0.05 with a false discovery rate (FDR) correction at the voxel level and a cluster size over 40 voxels were used to identify peak clusters on which subgroups differed [52].
As for resting-state brain activity, mixed-effects models of Group × Time with covariates (age, gender, head motion) were conducted using the Data Processing & Analysis for Brain Imaging toolbox (DPABI 4.0, http:/rfmri.org/dpabi). Again, the paired t test with head motion as the covariate was applied for each group if the Group × Time interaction was significant. Gaussian random field (GRF) correction (voxel level p < 0.05, cluster level, p < 0.05, two-tailed) was conducted for each analysis.
留言 (0)