
Remember me






Initially, 127 primary studies were identified through various databases and registry searches. After excluding 79 studies due to duplication, 23 studies were further eliminated based on titles and abstracts that were unrelated to the research topic. The remaining 25 full-text articles underwent a rigorous screening process to assess their eligibility for inclusion in the meta-analysis. Of the 25 full-text articles, 13 studies were excluded because they did not meet the eligibility criteria. The criteria for exclusion included studies that did not focus on household or individual client satisfaction, methodological problems, inaccessible or undefined results, letters, reviews, commentary, and studies conducted outside of Ethiopia. Finally, 12 primary studies [24, 34,35,36,37,38,39,40,41,42,43,44] that scored six or higher out of eight on the JBI quality score were considered suitable for systematic review and meta-analysis. These studies focused on household or individual client satisfaction in Ethiopia and had high-quality research methodologies. Therefore, the selection process was extensive and rigorous to ensure that the studies included in the meta-analysis were of high quality and provided relevant information on the topic of interest (Fig. 1).
Fig. 1
A flow diagram depicting studies included in a systematic review and a meta-analysis to estimate the pooled household satisfaction with community-based health insurance in Ethiopia
Study characteristicsA meta-analysis was conducted to examine 12 primary studies that were carried out in Ethiopia. These studies were conducted in the three largest regions of the country and the Addis Ababa city administration. The studies included six from Amhara [34, 35, 39, 40, 43, 45], three from SNNPs [24, 35, 38], two from Addis Ababa [36, 37], and one from Oromia [42]. The sample sizes of the studies varied from 314 to 627, and the total study size was 5311 (as shown in Table 1). All the studies were cross-sectional observational epidemiological studies published between 2016 and 2023. Two of the 12 studies [42, 44] employed mixed methods using both qualitative and quantitative data collection techniques. These studies were conducted among households that purposely selected CBHI enrollees.
Results of study bias assessmentEach paper underwent a thorough assessment, classifying studies as either low risk or good quality if they scored 8 out of 8, while studies scoring 6 or 7 were deemed medium risk. No study was excluded from the reviews using the above appraisal tools. The following criteria were utilized to evaluate cross-sectional studies: (1) adherence to inclusion criteria, (2) clear description of study subjects and settings, (3) utilization of valid and reliable exposure measurements, (4) utilization of objective and standardized criteria, (5) identification of confounding factors, (6) implementation of strategies to address confounding, (7) appropriate outcome measurement, and (8) utilization of suitable statistical analysis (Table 2).
Table 2 Quality appraisal results of included cross-sectional studies in Ethiopia, Using Joanna Briggs Institute (JBI) quality appraisal checklist for systematic review and meta-analysisHousehold satisfaction with community-based health insurance in EthiopiaThis study conducted a meta-analysis and systematic review to evaluate household satisfaction with community-based health insurance (CBHI) in Ethiopia. The research gathered data from various sources and calculated household satisfaction by dividing the number of satisfied household heads by the total study size and then multiplying the results by 100.
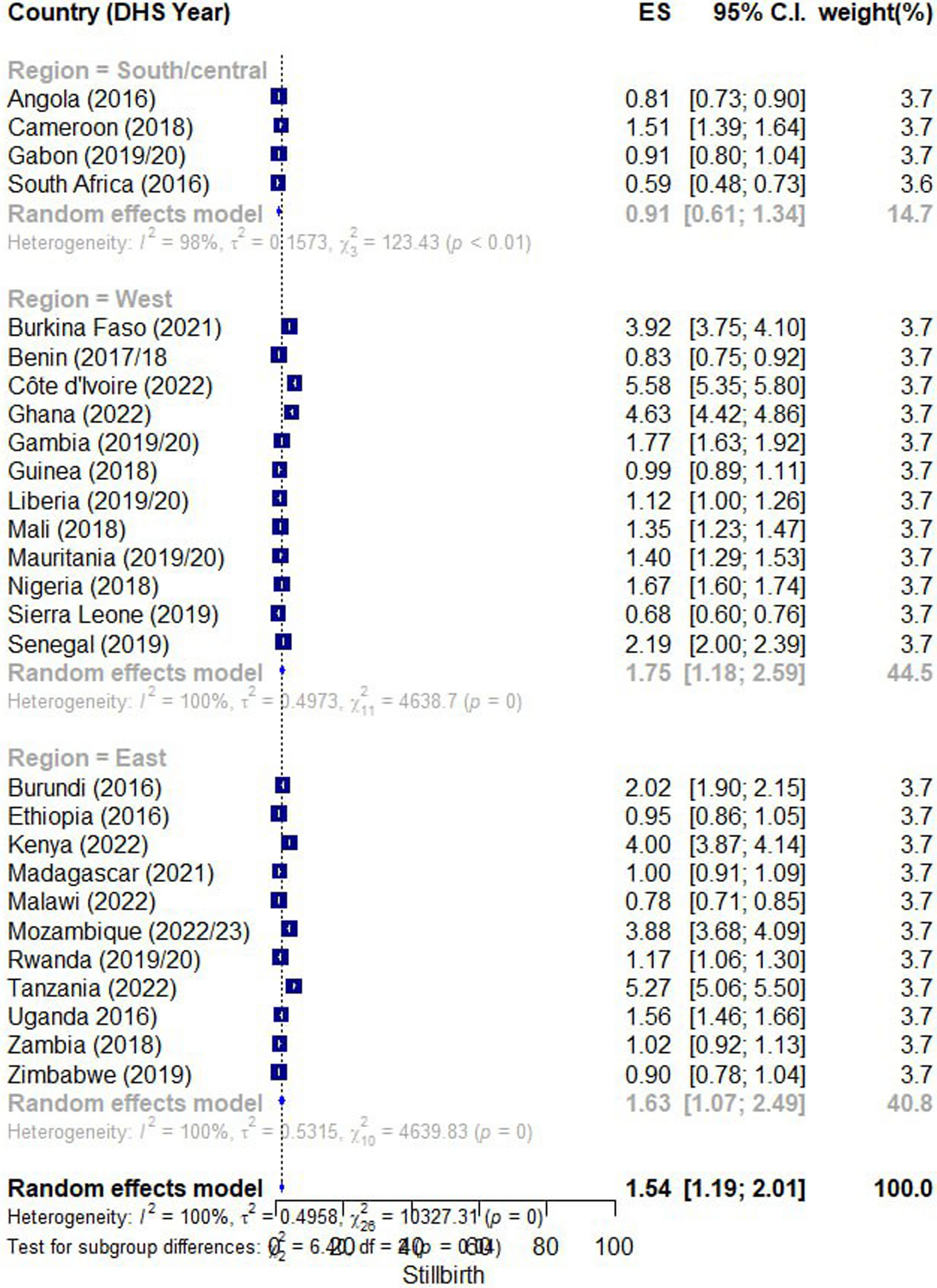
The meta-analysis findings showed that the overall household satisfaction with CBHI in Ethiopia was 62.26%, with a 95% confidence interval ranging from 53.25 to 71.21%. These results suggest that many households in Ethiopia are satisfied with CBHI. The study also used a forest plot to visualize the meta-analysis results.
A visualized forest plot revealed that the SNNP region had the highest household satisfaction reported by Badacho et al. [24]. The second-highest level of satisfaction was reported in the Amhara region by Abera Af et al. [34]. These results indicate that there are regional variations in the level of household satisfaction with CBHI in Ethiopia.
The findings of this study are essential for policymakers and healthcare providers in Ethiopia as they provide insight into the success and limitations of CBHI programs. The results suggest that there is a need for targeted interventions to increase the level of household satisfaction with CBHI in regions where satisfaction is lower. Additionally, the study highlights the importance of continued monitoring and evaluation of CBHI programs to ensure their sustainability and effectiveness (Fig. 2).
Fig. 2
A forest plot illustrating the pooled level of household satisfaction with CBHI in Ethiopia
Results of sensitivity analysisThe study conducted an inverse variance test (I2 test) among primary studies and found that there was a high degree of heterogeneity between studies (I2 = 98.19, p value < 0.00). To check the stability of the estimated effect sizes and the source of heterogeneity, the researchers used a "leave-one-out" evaluation approach as a sensitivity analysis. In this approach, they removed one study at a time and estimated the surrogacy measures using the remaining studies. This iterative procedure was used to investigate potential outlier studies on the overall effect size and identify them.
The sensitivity analysis showed that the meta-analysis finding was not dependent on a single study, and the estimated overall effect size was relatively stable. The presented effect size for each study corresponded to an overall effect size calculated from a meta-analysis excluding that study. The leave-one-out forest plot was also used to help detect outlier studies. This plot showed a vertical line at the overall effect size based on the complete set of studies (with no omission). After deleting a single study at each iteration step, the researchers found that the pooled estimate of household satisfaction varied from 59.60 (95% CL 53.03–66.17) to 63.71 (54.55–72.86) (Fig. 3). Overall, the sensitivity analysis showed that the findings of the meta-analysis were robust and not influenced by any single study.
Fig. 3
A forest plot depicting leave-one-out sensitivity analysis to estimate pooled household satisfaction with CBHI in Ethiopia
Subgroup analysis by region of primary study for household satisfaction with community-based health insurance in EthiopiaWe conducted a subgroup meta-analysis stratified by the primary studies' location to explore household satisfaction with CBHI. When analyzing the results based on the different regions in Ethiopia, the study found that the level of household satisfaction with CBHI was 63.40% (95% CI 58.67–68.13, I2 = 0.00, p = 0.00) in Oromia, which was the nearest to the national overall household satisfaction level. Similarly, the study found that the level of household satisfaction with CBHI was 64.01% in Amhara, which was relatively higher than in Addis Ababa city and the Oromia region.
In contrast, the study found that the level of household satisfaction with CBHI was the lowest in Addis Ababa, with a satisfaction rate of 49.68%. This is a significant finding, as Addis Ababa is the capital city of Ethiopia and has a relatively higher level of socioeconomic development compared to other regions.
Finally, the study found that the level of household satisfaction with CBHI was 66.76% (95% CI 40.12–93.40, I2 = 99.39, p = 0.06) in the South Nation Nationality and Peoples (SNNPs) region, which was the highest satisfaction rate observed in any of the regions. The high level of household satisfaction in SNNPs suggests that CBHI is a feasible and effective health financing mechanism for rural communities in Ethiopia.
Overall, the subgroup analysis results suggest that household satisfaction with CBHI varies across different regions in Ethiopia, with the highest satisfaction rates observed in rural regions such as SNNPs. These findings have important implications for policymakers and program implementers, as they highlight the need to tailor health financing mechanisms to the specific needs and contexts of different regions in Ethiopia (Fig. 4).
Fig. 4
Forest plot depicting subgroup analysis by region of household satisfaction with CBHI in Ethiopia
Factors associated with household satisfaction with CBHI in EthiopiaThis systematic review and meta-analysis included 12 primary studies to investigate the association between household satisfaction and community-based health insurance (CBHI). Three out of eight studies indicated a significant association between household satisfaction and the availability of drugs within the healthcare facility providing the CBHI scheme, with a pooled odds ratio of 2.13 (95% CI 1.47–2.78). This means that households whose prescribed drugs were available in the healthcare provider were 2.13 times more likely to be satisfied than those whose prescribed medications were unavailable. Two out of three studies included to assess whether friendly services are a predictor variable showed a significant association with household satisfaction, with a pooled odds ratio of 3.85 (95% CI 1.60–6.10). The result indicated that households who got friendly services in the healthcare facility under the CBHI scheme were more likely satisfied than those who did not receive friendly services.
Two primary studies were included in a meta-analysis to assess the association between premiums and household satisfaction, and both reported that premiums were a factor associated with household satisfaction. The findings showed that households with no extra expense during healthcare visits were 2.8 times more likely to be satisfied than those who paid an additional cost from the annual premium. However, none of the three primary studies included to assess the effect of the availability of diagnostic services on household satisfaction under the CBHI scheme reported a significant association, and the pooled odds ratio from the random effect model showed an insignificant association with the outcome variable (OR 1.99; 95% CI 0.27–3.70). Furthermore, two studies analyzed qualitative data to identify factors associated with household satisfaction and CBHI. The finding supported that the availability of drugs in the healthcare facilities under the CBHI scheme and friendly services are positively associated factors with household satisfaction and community-based health insurance in Ethiopia.
Lastly, the knowledge and awareness of household heads about the CBHI scheme were associated with household satisfaction. The finding indicated that households with knowledge and awareness about CBHI were 2.52 times more likely to be satisfied than those without knowledge/awareness. These results are summarized in table (Table 3).
Table 3 A table depicting factors associated with household satisfaction and community-based health insurance in Ethiopia
Comments (0)