
記住我


Nonconvulsive seizures (NCSs) are prevalent among critically ill patients and patients with recent convulsive seizures, with a reported incidence of 8% to 20% in the intensive care unit (ICU) population.1 Frequently, NCSs can go undetected at the bedside because of subtle clinical symptoms, but most can be diagnosed with electroencephalography (EEG) monitoring.2,3 Current guidelines from multiple professional societies support prompt evaluation of patients using EEG after convulsive status epilepticus, cardiopulmonary resuscitation, and acute brain injuries (eg, traumatic brain injury, stroke) that lead to altered mental status and/or seizures.4–6 Delays in obtaining EEGs are associated with decreased diagnostic yield and latency in administering antiseizure medications, which may lead to increased seizure burden and decreased efficacy of antiseizure medications.7–9 Conversely, prompt diagnosis and treatment may be neuroprotective, improve patient prognosis, and reduce hospital or ICU length of stay (LOS).10 Several factors contribute to delayed seizure recognition and hinder timely diagnosis and treatment. Although other training initiatives have shown that nursing staff can effectively recognize and monitor EEG patterns in continuous and long-term monitoring settings, this is still dependent on readily available EEG equipment.11–14 A major contributor at many hospitals is limited access to rapid conventional EEGs. This is often due to cumbersome and expensive conventional EEG equipment that requires highly trained technicians.15 In addition, fellowship-trained neurologists are needed to interpret conventional EEG tracings and guide diagnostic and therapeutic decisions.15,16
Recently, a point-of-care, rapid-response EEG (POC-EEG) platform (Ceribell Inc) received 510(k) clearance from the United States Food and Drug Administration. The POC-EEG systems record electrographic data comparable with conventional EEG.17 The system's straightforward montage and setup enables ancillary staff to acquire a rapid-response EEG in a fraction of the time needed for a technician to set up a conventional EEG.18 A prospective multicenter study demonstrated that POC-EEG increases diagnostic confidence and accuracy in managing suspected NCS patients, where seizure diagnosis sensitivity and specificity increased from 77.8% to 100% and 63.9% to 89%, respectively.19 It has been estimated that this may result in cost-savings from decreased hospital LOS, rates of intubation, and duration of mechanical ventilation.20 Finally, POC-EEG has previously been successfully deployed at community hospitals with limited conventional EEG infrastructure.21 The purpose of this quality improvement (QI) project was to expand EEG availability and facilitate 24/7 access to stat EEGs for the emergency department (ED) and inpatient units. Our primary goals were to reduce time to EEG, enhance seizure detection, and reduce patients' LOS.
Problem IdentificationOur hospital is a 208-bed, not-for-profit, suburban community hospital in Northern California. The hospital has a 5-star rating from Centers for Medicare & Medicaid Services and is a leader in cardiac, orthopedic, and vascular services. Before 2018, access to EEG was limited. The hospital had only 1 part-time EEG technician and 1 conventional EEG machine. These scarce resources were divided between inpatient and outpatient services and restricted to typical business hours. Limited staffing and equipment resulted in significant wait times for EEG studies. Fewer than 100 conventional EEGs were conducted annually, with most being completed in the ICU. Monitoring of long-term EEG was challenging, because there were only 2 fellowship-trained neurologists on staff. As a result, real-time patient care decisions could not always be made using conventional EEGs. Treating physicians, often the ED and ICU attending physicians, relied on clinical judgment alone for managing patients with antiseizure medications or critical care interventions. Between 2017 and 2018, EEG services were further impacted by high staff turnover and limited availability of trained EEG technicians. This led to the evaluation of whether a POC-EEG protocol could be implemented at our institution to expand EEG coverage.
MethodsStakeholders for the QI project included nurse managers of the ED, ICU, cardiac surveillance, and medical-surgical orthopedics units, as well as the chiefs of medicine for the hospitalist, intensivist, emergency, and neurology departments, as well as the respiratory therapists (RTs). These stakeholders collaborated to identify barriers in assessing and treating suspected seizure patients and to review the rapid-response EEG technology. The hospital subsequently purchased 2 rapid-response EEG devices for the QI project.
POC-EEG ProtocolSpearheaded by nursing leadership, the team created a standardized protocol to obtain POC-EEGs for all suspected seizure patients (Supplemental Digital Content 1, Fig 1, https://links.lww.com/JNN/A465). Indications for activating the protocol were as follows: recent seizure or status epilepticus without return to baseline; cardiac arrest, in parallel with targeted temperature management; unexplained or persistent altered mental status in the setting of traumatic brain injury, infection, or stroke; episodic repetitive movements that concerned the clinical team; and suspected seizure-like nonepileptic events. RTs and nurses underwent training with the protocol, devices, connectivity monitoring, and troubleshooting. A new stat rapid-response EEG order was created in our electronic health record (EHR).
The POC-EEG protocol could be initiated by a nurse, advanced practice provider, or physician from anywhere in the hospital. When a stat EEG order was received by the RTs, they would bring a device from their workroom, apply it to the patient, and begin the EEG recording. Nursing monitored the connection of the device, especially during and after patient movement or transport. Any connectivity issues were resolved by RTs. Using the devices' previously validated brain stethoscope function,19,21–23 staff would perform an initial assessment for any suspicious rhythmic activity. If such activity was present, the on-call neurologist would be consulted and then review the EEG tracings remotely through an Internet portal. Treatment decisions could now be made by the care team, in real time, based on the POC-EEG diagnostics.
Data Collection and AnalysisThe data collection was performed retrospectively. The QI project was presented to the institutional review board and determined to be exempt from their oversight. We subsequently conducted a review of EHR data to measure the following key performance indicators determined by the stakeholders for both point-of-care and conventional EEGs: the time-to-EEG (ie, latency between EEG order and recording start time), the number of seizures or seizure-like activity (eg, highly epileptiform activity, defined elsewhere19) determined by patients' EEG report, and the LOS (in days) for any patient who received an EEG in the ED or inpatient units.
Patients who underwent conventional or POC-EEG monitoring during 2018 were identified through orders placed in the EHR. We defined the pre-QI period as the first 6 months of the year the protocol was introduced (January 1 to June 30, 2018), when only conventional EEGs were available. The post-QI period was defined as the last 6 months of the same year (July 1 to December 31, 2018), when all stat EEGs used the new protocol. We excluded EEGs obtained during the 2-week period spanning the final week pre-QI and the first week post-QI, when POC-EEG training and implementation were concurrent, from the analysis (Supplemental Digital Content 2, Fig 2, https://links.lww.com/JNN/A466).
The time-to-EEG was determined as the difference (in minutes) from when an EEG was ordered to when the EEG recording started, based on time-stamped information in the EHR (Supplemental Digital Content 3, Fig 3, https://links.lww.com/JNN/A467). Individual patients' LOS was determined based on when they were registered in the ED and when their discharge order was placed using the EHR. Data were binned into 24-hour periods representing hospital days. Quantitative data were described by counts and percentages or medians and interquartile ranges. Statistical significance was established by Mann-Whitney U tests for comparing nonparametric distributions using a threshold of 0.05. Microsoft Excel (version 16.54) and GraphPad Prism (version 9.3.1) were used for data management and statistical analysis.
We estimated how the rapid-response protocol may have impacted hospital finances through financial modeling, assuming annual patient EEG volume twice the amount measured during the 6-month post-QI period. Cost-savings were estimated by multiplying the difference in median LOS between conventional and rapid-response EEG patients by the cost per night. An assumption of a 10% ICU case mix was used based on American Hospital Association data regarding community hospital beds in the United States.24 Additional revenue was estimated by multiplying the difference in number of seizures detected in the pre-QI and post-QI periods by the reimbursement dollar amount for an EEG-confirmed seizure diagnosis based on Medicare Severity Diagnosis-Related Group (MS-DRG) complication or comorbidity, or major complication or comorbidity coding. We included equipment costs but did not incorporate personnel costs in the model (Supplemental Digital Content 5, Fig 5, https://links.lww.com/JNN/A469).
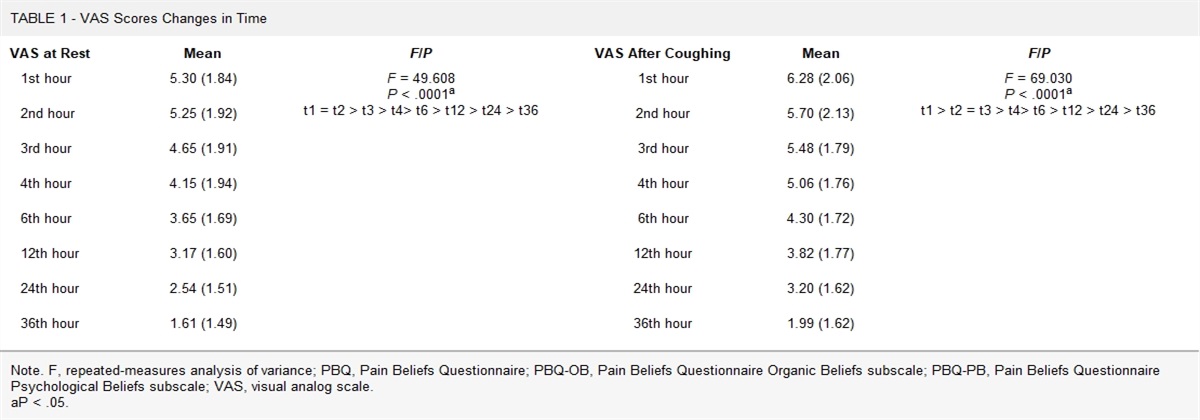
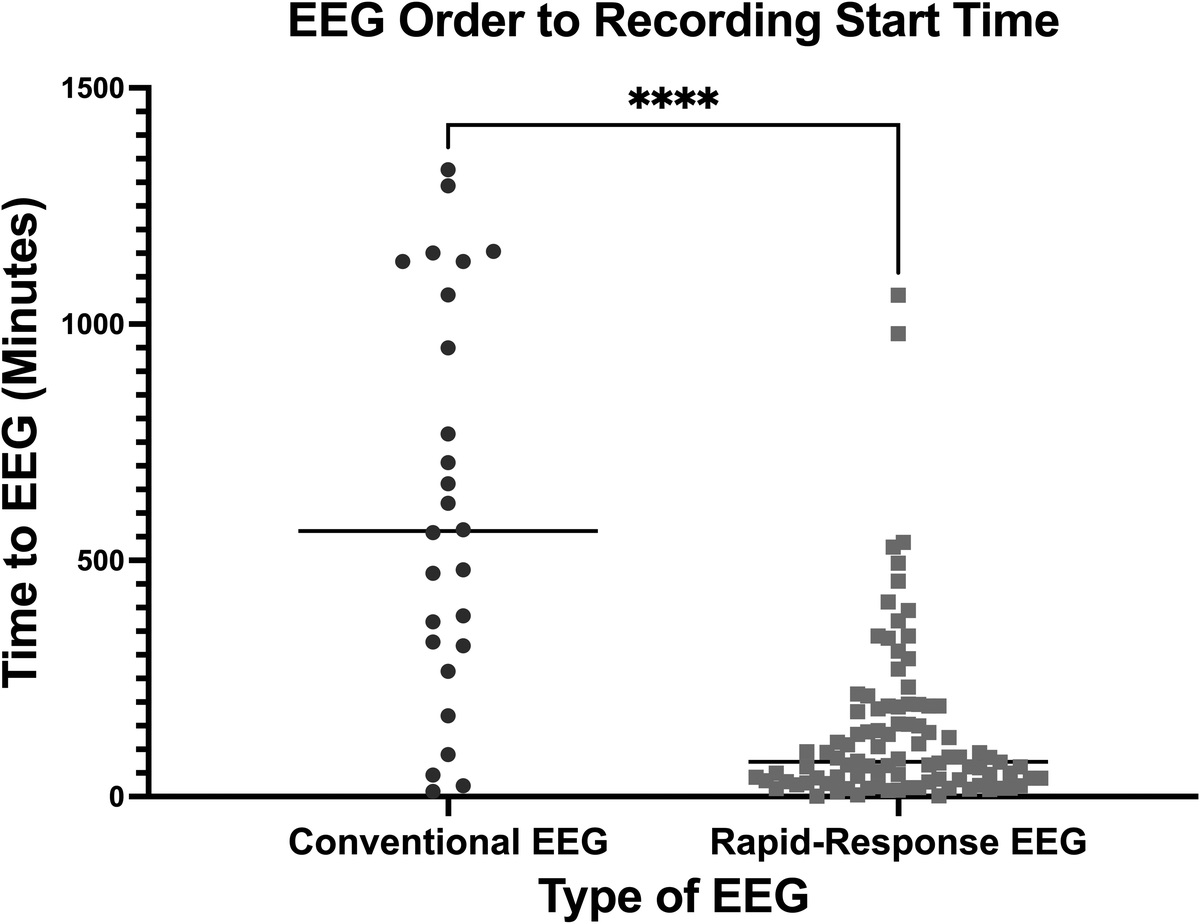
ResultsDuring the QI project, 164 EEGs were performed for suspected seizures per hospital standard of care. Complete data were available for 35 conventional EEGs obtained on 26 individual patients (pre-QI) and 115 POC-EEGs obtained on 76 individual patients (post-QI). Hospital location where EEG studies were performed were identified using our EHR (eg, ICU, ED, cardiac surveillance). The median time-to-EEG was computed for 26 studies conducted during the pre-QI period with conventional EEG and 96 studies during the post-QI period with POC-EEG. The median time-to-EEG for pre-QI conventional studies of 562 (321-103) minutes was significantly longer than the median time-to-EEG post-QI of 74 (34-187) minutes (P < .0001; Fig 1).
 FIGURE 1:
FIGURE 1: Rapid-response electroencephalography (EEG) was associated with a significant reduction in median time-to-EEG. Median ordering to recording time for conventional EEGs (circles, n = 26) was 562 (321-1034) minutes in the pre–quality-improvement period. Median ordering to recording time for rapid-response EEGs (squares, n = 96) was 74 (33.5-187) minutes in the post–quality-improvement period. “****” denotes statistically significant difference (P < .0001) between the 2 groups based on a 2-tailed Mann-Whitney U test.
Eight POC-EEG patients had an LOS < 1 day and were excluded because they were discharged from the ED (n = 6), transferred to an outside hospital (n = 1), or died within 24 hours of admission (n = 1). No conventional EEG patients had an LOS ≤ 1. Accordingly, we analyzed the median number of hospital days for 23 patients who underwent conventional EEG and for 62 patients who received POC-EEGs. The median LOS for pre-QI and post-QI patients of 7 (3.5-12.5) and 4 (2-10) days, respectively, were not significantly different (P = .058). However, we found that post-QI patients tended to have a shorter LOS (Supplemental Digital Content 4, Fig 4, https://links.lww.com/JNN/A468).
Diagnostic yield for seizures and seizure-like activity also improved with POC-EEG (Fig 2). Pre-QI, no seizures and only 1 instance of seizure-like activity was diagnosed with conventional EEG. In comparison, 43% of POC-EEGs captured seizures (22/115) or seizure-like activity (27/115). Implementation of the rapid-response protocol resulted in a 3.29-fold increase in EEG volume at the hospital (Supplemental Digital 3, Fig 3, https://links.lww.com/JNN/A467). During the project period, 28 POC-EEGs were performed in the ED (post-QI) compared with only 1 conventional EEG (pre-QI). Six patients received a POC-EEG before being safely discharged from the ED. Seven POC-EEG patients were discharged from the hospital within 24 hours. Every conventional EEG patient identified had an LOS of at least 2 days.
 FIGURE 2:
FIGURE 2: The rapid-response electroencephalography (EEG) protocol (gray bars, post–quality improvement) was associated with more seizures and seizure-like activity being captured compared with conventional EEG (black bars, pre–quality improvement). Zero seizures and 1 instance of seizure-like activity were diagnosed with conventional EEG. Forty-nine seizures or seizure-like activity were diagnosed by rapid-response EEG.
In the post-QI period, 15 patients were admitted at our institution and then had a seizure diagnosed by POC-EEG. Ten patients were admitted for nonseizure primary diagnoses and thus eligible for additional MS-DRG reimbursements. Nine patients qualified for complication or comorbidity DRG reimbursement and 1 for major complication or comorbidity DRG reimbursement because seizures were captured by POC-EEG (Supplemental Digital Content 5, Fig 5, https://links.lww.com/JNN/A469). In comparison, zero conventional EEG patients qualified for additional MS-DRG reimbursements. Accordingly, utilization of POC-EEG enabled the hospital to appropriately generate more revenue. Assuming that 230 POC-EEGs could be performed annually (twice the number of EEGs conducted post-QI), over the course of a year, the rapid-response protocol would be associated with $737 818 cost-savings because of reduced LOS and ED discharges, and an additional revenue of $145 580 from MS-DRG coding (Supplemental Digital Content 4, Fig 4, https://links.lww.com/JNN/A468). Since completing this QI project, the hospital has exclusively used the rapid-response protocol for all stat EEGs.
DiscussionStakeholders at our community hospital identified barriers to obtaining stat conventional EEGs. They included conventional EEG technician staffing, prohibitive costs for providing 24/7 conventional EEG coverage, and provider hesitation to order conventional EEGs for patients who posed a low-to-moderate suspicion of seizure due to actual or perceived lack of conventional EEG availability. Different interventions to streamline management of NCS and status epilepticus have been described in other QI publications and demonstrate improvements in time to treatments and increased diagnostic yield.25,26 However, these interventions do not address the staffing shortages and reduced after-hours coverage identified by the stakeholders here. The nursing and physician leadership hypothesized that adopting a point-of-care rapid-response EEG protocol could address all the identified barriers.
The introduction of POC-EEG at the hospital was associated with more efficient staffing, improved patient care, and hospital finances. After a 1-hour training session, ancillary staff could perform POC-EEGs. Having multiple, easily accessible, small devices meant multiple EEGs could be performed at any given time. This led to increased utilization of EEG such that POC-EEGs could be obtained at any hour, regardless of patient location or availability of conventional EEG technicians and equipment. From a nursing perspective, the POC-EEG technology liberated clinical resources for other patients by virtue of remote, real-time monitoring.
For the first time at the hospital, clinicians and nursing staff were able to reliably access EEGs for patients in the ED. The increased number of EEGs performed, decreased time-to-EEG, and better diagnostic yield provided evidence that critical care patients may have been underserved. This suggests that there are clear advantages for critical care nurses and bedside staff to incorporate emerging technologies that allow them to play more active roles in the management of NCS and nonconvulsive status epilepticus.27
From a financial perspective, the rapid-response EEG protocol may also be associated with a shorter LOS for hospitalized patients who require EEG monitoring. Although the LOS analysis did not yield a statistically significant difference, it was clinically significant because it enabled certain patients to be discharged sooner or avoid admission altogether. Furthermore, the data are consistent with a previous multicenter trial demonstrating that rapid-response EEG utilization was associated with per-patient cost-savings between $3971 and $17 290 driven by reduced LOS.20 Finally, additional seizures diagnosed by POC-EEG led to an increase in reimbursement from insurance providers. Taking estimated cost-savings, additional reimbursement, and equipment costs into account, our financial model projected that the rapid-response protocol resulted in a net profit for the hospital (Supplemental Digital Content 5, Fig 5, https://links.lww.com/JNN/A469).
This QI project has significant limitations. Statistical analyses were hindered by the relatively small sample sizes. An analysis comparing clinical variables such as demographics, medical history, indication for EEG order, and severity of illness for the pre-QI and post-QI subgroups was outside the scope of this project. The study's retrospective nature also complicates determinations of causality between POC-EEG utilization and LOS or other outcome metrics. The increased EEG utilization observed during the project period may have been affected by perceived availability of diagnostics. Thus, provider ordering behavior may have changed. Potential differences in pre-QI and post-QI patients' LOS may not be due to availability of EEG or improved treatment facilitated by the rapid-response protocol. However, we are not aware of any other hospital-wide initiatives that coincided with this project and could have confounded the results. Furthermore, this retrospective QI project could not analyze whether transitions of care (ie, expedited downgrades from the ICU, admissions from the ED) or changes in management (ie, intubations or administration of antiepileptic medications) occurred because of patients' POC-EEG.
Since the intervention was performed, staffing and infection control issues have only been exacerbated (eg, COVID-19 pandemic). Identifying sustainable alternatives to obtaining stat EEGs is highly desirable, and some case series have already documented the usefulness of POC-EEG systems during such scenarios.28,29 Future studies should prospectively look at the impact of rapid-response EEG monitoring with respect to treatment decisions, patient outcomes, and hospital finances over longer periods and across different departments.
ConclusionElectroencephalography-based management is multifactorial and influenced by the clinical heterogeneity of patients requiring EEGs, interprovider variability, and triage of clinical resources. Point-of-care rapid-response EEG may improve care for patients by making EEG services more efficient. At our community hospital, the introduction of a nursing-led rapid-response EEG protocol expanded access to EEGs. The availability of this technology resulted in decreased time from EEG order to the start of EEG monitoring. This may have improved patient flow through the ED and inpatient units. Our rapid-response EEG protocol was also associated with more EEG-confirmed seizures and additional DRG reimbursements. Although this retrospective QI project has limitations, based on its findings, we continued to use rapid-response EEGs at our hospital. Future studies are aimed at investigating how improved access to point-of-care diagnostic technologies impacts patient outcomes and hospital finances.
AcknowledgmentsThe authors would like to acknowledge Michelle Armenta Salas, PhD, as well as Drs Daniel Beckerman, Kapil Gururangan, and Josef Parvizi for critical feedback on the manuscript and statistical analysis.
References 1. Laccheo I, Sonmezturk H, Bhatt AB, et al. Non-convulsive status epilepticus and non-convulsive seizures in neurological ICU patients. Neurocrit Care. 2015;22(2):202–211. doi:10.1007/s12028-014-0070-0 2. Claassen J, Mayer SA, Kowalski RG, Emerson RG, Hirsch LJ. Detection of electrographic seizures with continuous EEG monitoring in critically ill patients. Neurology. 2004;62(10):1743–1748. doi:10.1212/01.wnl.0000125184.88797.62 3. Jirsch J, Hirsch LJ. Nonconvulsive seizures: developing a rational approach to the diagnosis and management in the critically ill population. Clin Neurophysiol. 2007;118(8):1660–1670. doi:10.1016/j.clinph.2006.11.312 4. Brophy GM, Bell R, Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17(1):3–23. doi:10.1007/s12028-012-9695-z 5. Panchal AR, Bartos JA, Cabañas JG, et al. Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(16_suppl_2):S366–S468. doi:10.1161/CIR.0000000000000916 6. Herman ST, Abend NS, Bleck TP, et al. Consensus statement on continuous EEG in critically ill adults and children, part I: indications. J Clin Neurophysiol. 2015;32(2):87–95. doi:10.1097/WNP.0000000000000166 7. King MA, Newton MR, Jackson GD, et al. Epileptology of the first-seizure presentation: a clinical, electroencephalographic, and magnetic resonance imaging study of 300 consecutive patients. Lancet. 1998;352(9133):1007–1011. doi:10.1016/S0140-6736(98)03543-0 8. Debicki DB. Electroencephalography after a single unprovoked seizure. Seizure. 2017;49:69–73. doi:10.1016/j.seizure.2017.03.001 9. Sánchez Fernández I, Goodkin HP, Scott RC. Pathophysiology of convulsive status epilepticus. Seizure. 2019;68:16–21. doi:10.1016/j.seizure.2018.08.002 10. VanHaerents S, Gerard EE. Epilepsy emergencies: status epilepticus, acute repetitive seizures, and autoimmune encephalitis. Continuum (Minneap Minn). 2019;25(2):454–476. doi:10.1212/CON.0000000000000716 11. Amorim E, Williamson CA, Moura LMVR, et al. Performance of spectrogram-based seizure identification of adult EEGs by critical care nurses and neurophysiologists. J Clin Neurophysiol. 2017;34(4):359–364. doi:10.1097/WNP.0000000000000368 12. Seiler L, Fields J, Peach E, Zwerin S, Savage C. The effectiveness of a staff education program on the use of continuous EEG with patients in neuroscience intensive care units. J Neurosci Nurs. 2012;44(2). Available at: https://journals.lww.com/jnnonline/Fulltext/2012/04000/The_Effectiveness_of_a_Staff_Education_Program_on.10.aspx 13. Picinich C, Kennedy J, Thind H, Foreman C, Martin RM, Zimmermann LL. Continuous electroencephalographic training for neuroscience intensive care unit nurses: a feasibility study. J Neurosci Nurs. 2020;52(5). Available at: https://journals.lww.com/jnnonline/Fulltext/2020/10000/Continuous_Electroencephalographic_Training_for.10.aspx 14. Kang JH, Sherill GC, Sinha SR, Swisher CB. A trial of real-time electrographic seizure detection by neuro-ICU nurses using a panel of quantitative EEG trends. Neurocrit Care. 2019;31(2):312–320. doi:10.1007/s12028-019-00673-z 15. Hilkman DMW, van Mook WNKA, van Kranen-Mastenbroek VHJM. Continuous electroencephalographic-monitoring in the ICU: an overview of current strengths and future challenges. Curr Opin Anesthesiol. 2017;30(2):192–199. Available at: https://journals.lww.com/co-anesthesiology/Fulltext/2017/04000/Continuous_electroencephalographic_monitoring_in.6.aspx 16. Benbadis SR. Use and abuse of stat EEG. Expert Rev Neurother. 2008;8(6):865–868. doi:10.1586/14737175.8.6.865 17. Kamousi B, Grant AM, Bachelder B, Yi J, Hajinoroozi M, Woo R. Comparing the quality of signals recorded with a rapid response EEG and conventional clinical EEG systems. Clin Neurophysiol Pract. 2019;4:69–75. doi:10.1016/j.cnp.2019.02.002 18. Kurup D, Gururangan K, Desai MJ, et al. Comparing seizures captured by rapid response EEG and conventional EEG recordings in a multicenter clinical study. Front Neurol. 2022;13:915385. doi:10.3389/fneur.2022.915385 19. Vespa PM, Olson DM, John S, et al. Evaluating the clinical impact of rapid response electroencephalography: the DECIDE multicenter prospective observational clinical study. Crit Care Med. 2020;48(9):1249–1257. https://doi.org/10.1097/CCM.0000000000004428 20. Ney JP, Gururangan K, Parvizi J. Modeling the economic value of Ceribell rapid response EEG in the inpatient hospital setting. J Med Econ. 2021;24(1):318–327. https://www.doi.org/10.1080/13696998.2021.1887877 21. Yazbeck M, Sra P, Parvizi J. Rapid response electroencephalography for urgent evaluation of patients in community hospital intensive care practice. J Neurosci Nurs. 2019;51(6):308–312. doi:10.1097/JNN.0000000000000476 22. Hobbs K, Krishnamohan P, Legault C, et al. Rapid bedside evaluation of seizures in the ICU by listening to the sound of brainwaves: a prospective observational clinical trial of Ceribell's brain stethoscope function. Neurocrit Care. 2018;29(2):302–312. doi:10.1007/s12028-018-0543-7 23. Parvizi J, Gururangan K, Razavi B, Chafe C. Detecting silent seizures by their sound. Epilepsia. 2018;59(4):877–884. doi:10.1111/epi.14043 24. American Hospital Association. AHA Hospital Statistics. 2022nd ed. Chicago, IL: Health Forum; 2022. 25. Pranboon S, Tiamkao S, Chainirun N, Sawanyawisuth K; Integrated Epilepsy Research Group. A fast-track care by a nursing case management concept improved status epilepticus outcomes. J Neurosci Nurs. 2020;52(4):200–204. doi:10.1097/JNN.0000000000000522 26. Gupta N, Baang HY, Barrett W, et al. Reducing seizure to needle times in nonconvulsive status epilepticus with multifaceted quality improvement initiatives. Epilepsy Res. 2023;190:107085. doi:10.1016/j.eplepsyres.2023.107085 27. Alexandrov A. Where early suspicion, detection, and treatment advocacy in nonconvulsive status epilepticus: a role for the critical care nurse. Int J Crit Care. 2022;16(3):1–3. 28. LaMonte MP. Ceribell EEG shortens seizure diagnosis and workforce time and is useful for COVID isolation. Epilepsia Open. 2021;6(2):331–338. doi:10.1002/epi4.12474 29. Agarwal S, Sabadia S, Abou-Fayssal N, Kurzweil A, Balcer LJ, Galetta SL. Training in neurology: flexibility and adaptability of a neurology training program at the epicenter of COVID-19. Neurology. 2020;94(24):e2608–e2614. https://doi.org/10.1212/WNL.0000000000009675
留言 (0)