
Remember me


Multiple sclerosis (MS) is a chronic autoimmune-based degenerative disorder of the central nervous system with a variable clinical course characterized by progressive disability.1 Early treatment initiation decreases inflammatory activity and the risk of disease progression.2 Several disease-modifying treatments are available for relapsing-remitting MS (RRMS) at different doses and with varying features.3 Therefore, patients with RRMS may experience decisional conflict at the time of treatment choice.4
Shared decision making (SDM), a decision-making process shared by patients and their healthcare providers, aims to help patients and clinicians reach a treatment decision considering patients' values.3,5 Nurse professionals lead the SDM process by providing patients with support and information during face-to-face clinical encounters. In the Spanish setting, neurologists are legally responsible for prescriptions and therefore participate in the SDM process, making the final treatment decision and prescription.5 Furthermore, nurses are essential within MS multidisciplinary teams and play a fundamental role in facilitating the SDM process.6
Implementation of SDM models requires understanding large amounts of information and may be complex, especially when decisions have implications for patients' autonomy and quality and prolongation of life.7,8 For this reason, SDM uses patient decision aids (PtDAs) to facilitate informed, value-based decisions regarding health.9–11Decision aids have proven knowledge improvement, consistency between treatment choice and patient values, and decisional conflict reduction. Furthermore, PtDAs have improved patients' access to health information and their ability to use it effectively by providing a friendly language with simple numbers, clear visualization of data, and narrative examples.12,13
A nurse-led educational program has been developed in Catalonia to empower patients with MS in disease self-management.14 However, a PtDA facilitating SDM between RRMS patients and nurses was still missing. The Catalan Regional Government proposed the development of a PtDA using the international methodology for PtDAs to serve this unmet need, but information regarding the needs and demands of RRMS patients in the Spanish setting was missing.15 This qualitative study aimed to identify key elements in treatment choice from the perspective of patients with RRMS in the Spanish sociocultural context to create a PtDA to support patients with RRMS and nurses during SDM.
MethodsThis was a qualitative study16 with a constructivist naturalistic approach, which was conducted through focus group interviews to identify the needs and demands of patients with RRMS. Specifically, they were asked about their healthcare needs and demands, the SDM process, and general characteristics of a peer support program. Results were subdivided by themes.14 The study was approved by the hospital Clinical Research Ethics Committee. Participants were informed that they could withdraw from the study without giving any reasons, and anonymity and confidentiality were ensured. All participants provided informed consents for participation in the study.
Purposive sampling was used to recruit patients with RRMS receiving treatment in the Neuroimmunology and MS Unit.17 We conducted an informative session and requested voluntary participation from assistants. Study participants were selected among those who expressed their willingness to attend a focus group, considering the representation of participants with different characteristics, of both sexes, and different ages. Potential participants with severe cognitive impairment or alterations in communication that hindered their participation were excluded.
We planned 4 focus groups of 5 to 8 participants, as recommended.17 However, the final number of groups (ie, sample size) was determined by information power18 (ie, accrual of enough repetitive and substantial information to obtain conclusions). Sessions were conducted from January to February 2016 by an MS clinical nurse specialist as the principal investigator, following a semistructured script (Supplemental Digital Content 1, https://links.lww.com/JNN/A476) to answer the exploratory points obtained from a literature review.19 Another MS clinical nurse specialist was present as an observer and collected the complementary information.
Focus group sessions were held in a reserved room, ensuring an interruption-free space. At the beginning of the session, the moderator thanked participants for attending, informed them of the session's purpose, and reminded them that the analysis and dissemination of research results would remain confidential. Focus groups lasted 1.5 to 2 hours, during which the moderator intentionally sought participants' points of view and experiences regarding research concepts. The recordings of the informants' contributions were transcribed verbatim for analysis.
Qualitative data were analyzed by thematic analysis and a constructivist naturalistic approach20 using NVivo 11 software. The analysis included familiarization with data, generation of initial codes, theme searching, revision, definition, naming, and report writing.20 Independent peer analysis was conducted by the principal investigator and the study coordinator. This study was reported in accordance with the guidelines provided by the Standards for Reporting Qualitative Research.21
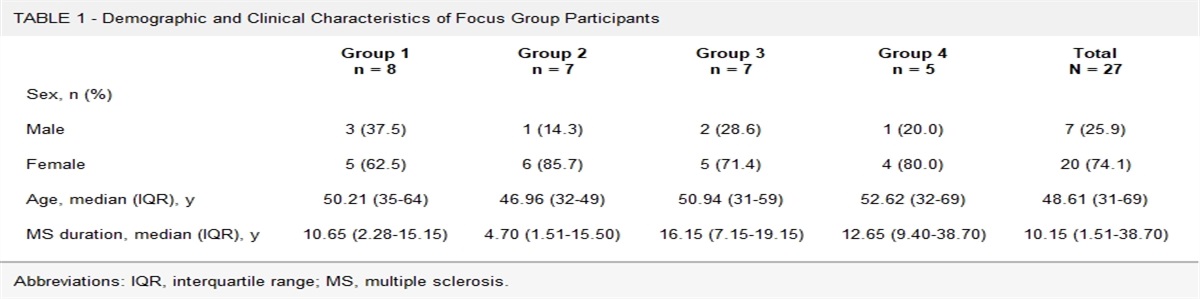
ResultsOf 37 patients with MS approached for consent, 27 agreed to participate. Four focus group interviews were performed. Participants were mostly female (74.1%), middle-aged (48.6 years), and with a long MS evolution (10.2 years). Table 1 summarizes the characteristics of study participants in each focus group. Three overarching themes were identified: “information access,” “knowledge of treatment options,” and “decision-making role.” Table 2 shows a comprehensive list of categories and codes that emerged from participants' narratives after analyzing all open-ended questions.
TABLE 1 - Demographic and Clinical Characteristics of Focus Group Participants Group 1Abbreviations: IQR, interquartile range; MS, multiple sclerosis.
Abbreviation: SDM, shared decision making.
Participants identified access to sufficient and high-quality information as a key element in the SDM process. Participants searched for information online, and despite the abundancy of data available on the Internet, they experienced difficulties in finding appropriate, understandable information for nonprofessional readers because most sources used technical terms. We identified the need for reliable, accessible, updated, sufficient, and proportionate information adapted to the lay audience.
“I did a search online and clearly found loads of information. Honestly, at that moment, I couldn't decide which content was true and matched my illness and my situation. Back then, if I had known where to look for these data, I wouldn't have searched everywhere; instead, I would have narrowed my search and made it more accurate for me” (P25.FG4_woman_32y).
Regarding disease and treatment, information was essential to personal autonomy and should be accessible outside the clinical setting: “We're always being sent lots of leaflets, and we sit down...” (P2.FG1_woman_39y).
Participants appreciated information being available to share outside the clinical setting in a relaxed environment, without time restrictions. Collaboration with family reduced anxiety: “It's great that we can all sit around the table at home and have a look at them. We all look through them together and discuss them…. This one does this and that; I don't know what to do. Another says: We can rule this one out” (P2.FG1_woman_39y).
Treatment OptionsParticipants considered it essential to have treatment options for optimal treatment choice awareness regarding efficacy, adverse effects, administration frequency and route, and impact on daily life. Information about treatments according to their type of MS and clinical situation was also appreciated:
“We aren't doctors, and we aren't allowed to understand which treatment is the best for us considering our number of lesions and our situation. We are not equipped with all the essential information to make such important decisions” (P14.FG2_woman_49y).
All focus groups linked the concept of efficacy to treatment success in decreasing disease impact. They believed the main treatment goal should be to reduce relapses and control MS evolution: “They give you a certain percentage of protection against relapses; this [medication] one gives you 35% protection against potential relapses, and of course, there is less evolution” (P14.FG2_woman_49y).
Participants found it essential to be aware of treatment adverse effects to make an informed treatment selection and to enable their identification when they occurred. Participants were worried about treatment adverse effects, even those sufficiently informed, and these feelings persisted until treatment initiation: “What worries me are the side-effects.... As long as it [the medication] works, I don't care if I must inject myself ten times a day or more. However, side effects do worry me” (P21.FG3_woman_59y).
Participants accepted monitoring and follow-up controls as necessary for detecting adverse effects and potential drug-associated complications. Their early detection helped decrease participant vulnerability, increasing their sense of control. Likewise, in most cases, follow-ups improved participants' sense of security: “You must maintain a strict follow-up, which means undergoing blood tests periodically. So, it's possible to assess the state of different organs involved in the treatment, which may affect, for instance, the liver” (P13.FG2_woman_49y).
Administration frequency was an important criterion associated with potential adverse effects. Participants shared their experiences with previous treatments and correlated adherence with associated adverse effects. Treatments administered with a higher frequency and significant adverse effects increased their feelings of being ill. Consequently, participants prioritized drugs with a lower administration frequency: “Just thinking I've got to take a pill every day is knowing I've got sclerosis every day. If I don't [intravenous therapy], I don't remember for 28 days” (P3.FG1_woman_53y).
Moreover, information regarding administration route and frequency was identified as critical for treatment selection. This information included treatments requiring self-administered injections that may cause pain or rapid-onset local adverse effects, injection frequency, and new treatment options not requiring injections: “In any case, self-injecting is a nuisance; the more often you must do it, the greater discomfort, isn't it? When you do it, that's when you remember you're ill” (P2.FG1_woman_39y).
Finally, participants identified the knowledge of treatment impact on daily life and activities as essential for a successful choice. Participants prioritized treatments that were less likely to impact their lives because they considered that these should help minimize the inconveniences caused by their disease: “Easy to manage. Ultimately, we look for a treatment with the expectation that it won't affect our daily and ordinary lives” (P5.FG1_man_64y).
During the focus group sessions, we observed 2 attitudes among participants: 1 group preferred an engaged decision-making role and considered that health professionals' support was necessary for doubt resolution throughout the process: “If you have a wide range of options, you have to be able to decide which treatment you want and which one adapts better to your lifestyle—having the right to choose what's best for you and following your own criteria. That's all” (P1.FG1_woman_41y).
On the other hand, nonengaged participants preferred to delegate the responsibility to the healthcare team. This opinion was less common and was related with their trust in the clinician. Nevertheless, these participants were also aware of the importance of improving their knowledge to understand their situations and empower themselves: “In the end, I trusted the doctor's opinion and chose the treatment that he told me to be the best one” (P10.FG2_woman_49y).
DiscussionWe found that patients with RRMS have difficulty finding sufficient, up-to-date, good-quality, reliable information regarding the MS treatments available. Patients with RRMS are mainly interested in obtaining knowledge about the efficacy, adverse effects, administration route and frequency, and impact on daily life of treatment options. Despite the 2 identified approaches regarding decision-making roles (engaged vs nonengaged), there is consensus among participants that they should be more active in treatment decisions.
Access to Sufficient and High-Quality InformationGiven the complexity of MS and the variety of treatments, providing reliable and accurate sources of information is essential for patient involvement in decision making.22 Patients with MS generally search for treatment information online and exchange information using electronic health technologies.23 Moreover, as shown in this study, it is essential for patients with RRMS to have access to reliable, accessible, updated, comprehensible, and sufficient information.24
Some web-based applications have been developed to help MS patients choose their treatment.25 These aids provide information, help patients decide their preference, and improve knowledge, expectations, and participation. Moreover, they reduce decisional conflict, inequalities in patient access, and delayed decisions, and they encourage adherence.13,26 However, aids' design, led by nurses, should consider patients with RRMS and healthcare professionals and include the relevant contents identified during the nurse-led focus groups. Moreover, by using a virtual environment with patient-friendly language, they may facilitate communication between nurses and patients during clinical encounters, improving comprehension and satisfaction with the SDM process.22
Treatment OptionsProviding evidence-based, balanced information on treatment benefits and adverse effects helps increase disease-related knowledge.27 Most patient education interventions include drug therapy, relapse management, health promotion, and MS impact on a person's life.24 In line with the literature, participants in this study identified these aspects as key elements in MS treatment, highlighting the need for disease information,28 including the benefits and risks associated with first-line treatments.29 In addition, new treatment options for MS are associated with greater complications and adverse effects. In this regard, the SDM process in MS is strongly influenced by patients' risk perception.30 The aspects identified in this study are consistent with the contents of the main web-based aids available for MS treatment understanding. Most of these aids explain why SDM is necessary, provide general information about the disease, and explain the usefulness of treatments for RRMS.25
Decision-Making RoleDespite studies showing that most patients with MS prefer SDM,31 some would still rather have their physician decide for them.32 In this regard, previous studies have also identified these 2 attitudes regarding decisions: engaged patients have the knowledge, motivation, skills, and confidence to make an effective, shared decision, whereas nonengaged patients delegate the decision making entirely to health professionals with no participation.33Shared decision making can be developed and strengthened, even among those who initially are less confident and motivated or have low levels of health literacy.34 All these elements are consistent with the results from the focus groups.
Nurse-led SDM and PtDAs aim to help patients make a treatment choice by encouraging their participation.35 However, most websites and PtDAs are developed by the pharmaceutical industry focusing on patient treatment adherence and have not been specifically designed to address the needs and demands of patients with MS.35 Identifying key elements in SDM from the perspective of RRMS patients to integrate them in PtDAs may help solve these issues and strengthen the role and participation in their treatment selection process. Furthermore, they may facilitate the nurses' essential role in supporting treatment decisions.
LimitationsThis study's population might not be representative outside this sociocultural environment, because participants' needs and demands are closely linked to services, resources, and healthcare models implemented in their region. Further studies are necessary to assess the effectiveness of the virtual environment on treatment selection and its impact on health literacy and patient-reported outcomes and experience of potential users.
ConclusionsKey self-perceived elements in SDM in patients with MS include access to sufficient high-quality data, knowledge on treatment options with available information on relevant features of each treatment, impact on daily life, and the patients' role in treatment decision. Integrating these elements in SDM should facilitate promoting the nurse-led SDM process, reduce the lack of understanding during encounters between nurses and RRMS patients, and provide a comprehensive approach to meet the needs and demands of patients with MS. The findings from this study provided valuable information to develop virtual environment contents to facilitate the nurses' role of conveying information to patients and enhancing communication.
AcknowledgmentsThe authors would like to thank Sara Cervantes, PhD, for providing medical writing assistance during the preparation of the final manuscript draft.
References 1. Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. Lancet. 2018;391(10130):1622–1636. doi:10.1016/S0140-6736(18)30481-1 2. Tintore M, Rovira À, Río J, et al. Defining high, medium and low impact prognostic factors for developing multiple sclerosis. Brain. 2015;138(pt 7):1863–1874. doi:10.1093/brain/awv105 3. Wilkie DD, Solari A, Nicholas RSJ. The impact of the face-to-face consultation on decisional conflict in complex decision-making in multiple sclerosis: a pilot study. Mult Scler J Exp Transl Clin. 2020;6(4):2055217320959802. doi:10.1177/2055217320959802 4. Lowden D, Lee V, Ritchie JA. Redefining self: patients' decision making about treatment for multiple sclerosis. J Neurosci Nurs. 2014;46(4):E14–E24. doi:10.1097/JNN.0000000000000064 5. Keij SM, van Duijn-Bakker N, Stiggelbout AM, Pieterse AH. What makes a patient ready for shared decision making? A qualitative study. Patient Educ Couns. 2021;104(3):571–577. doi:10.1016/j.pec.2020.08.031 6. Friesen-Storms JHHM, Bours GJJW, van der Weijden T, Beurskens AJHM. Shared decision making in chronic care in the context of evidence based practice in nursing. Int J Nurs Stud. 2015;52(1):393–402. doi:10.1016/J.IJNURSTU.2014.06.012 7. Légaré F, Ratté S, Gravel K, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: update of a systematic review of health professionals' perceptions. Patient Educ Couns. 2008;73(3):526–535. doi:10.1016/j.pec.2008.07.018 8. Ubbink DT, Damman OC, de Jong BA. Shared decision-making in patients with multiple sclerosis. Front Neurol. 2022;13:2574. doi:10.3389/FNEUR.2022.1063904/BIBTEX 9. Stacey D, Légaré F, Lewis KB. Patient decision aids to engage adults in treatment or screening decisions. JAMA. 2017;318(7):657–658. doi:10.1001/jama.2017.10289 10. O'Connor A, Llewellyn-Thomas H, Stacey D. International Patient Decision Aid Standards (IPDAS) collaboration. IPDAS collaboration background document. 2005. Available at http://ipdas.ohri.ca/ipdas_background.pdf. 11. Hakim H, Newland P, Oliver BJ. Initial user testing of decision aids for multiple sclerosis disease-modifying therapies. J Neurosci Nurs. 2020;52(4):160–165. doi:10.1097/JNN.0000000000000521 12. Garcia-Retamero R, Cokely ET. Designing visual aids that promote risk literacy: a systematic review of health research and evidence-based design heuristics. Hum Factors. 2017;59(4):582–627. doi:10.1177/0018720817690634 13. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4):CD001431. doi:10.1002/14651858.CD001431.pub5 14. Robles-Sanchez MA, Cruz-Díaz V, Amil-Bujan P, Sastre-Garriga J, Ramió-Torrentà L, Bertran-Noguer C. An expert patient program as a tool to empower people with multiple sclerosis. J Neurosci Nurs. 2020;52(4):166–171. doi:10.1097/JNN.0000000000000514 15. Elwyn G, O'Connor A, Stacey D, et al. Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. BMJ. 2006;333(7565):417–410. doi:10.1136/bmj.38926.629329.AE 16. Caelli K, Ray L, Mill J. ‘Clear as mud’: toward greater clarity in generic qualitative research. Int J Qual Methods. 2003;2(2):1–13. doi:10.1177/160940690300200201 17. Doody O, Slevin E, Taggart L. Focus group interviews in nursing research: part 1. Br J Nurs. 2013;22(1):16–19. doi:10.12968/BJON.2013.22.1.16 18. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444 19. Kiesler DJ, Auerbach SM. Optimal matches of patient preferences for information, decision-making and interpersonal behavior: evidence, models and interventions. Patient Educ Couns. 2006;61(3):319–341. doi:10.1016/J.PEC.2005.08.002 20. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa 21. O'Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388 22. Rieckmann P, Boyko A, Centonze D, et al. Achieving patient engagement in multiple sclerosis: a perspective from the multiple sclerosis in the 21st century steering group. Mult Scler Relat Disord. 2015;4(3):202–218. doi:10.1016/j.msard.2015.02.005 23. Dennison L, McCloy Smith E, Bradbury K, Galea I. How do people with multiple sclerosis experience prognostic uncertainty and prognosis communication? A qualitative study. PLoS One. 2016;11(7):e0158982. doi:10.1371/journal.pone.0158982 24. Köpke S, Solari A, Rahn A, Khan F, Heesen C, Giordano A. Information provision for people with multiple sclerosis. Cochrane Database Syst Rev. 2018;10:CD008757. doi:10.1002/14651858.CD008757.pub3 25. Colligan E, Metzler A, Tiryaki E. Shared decision-making in multiple sclerosis: a review. Mult Scler J. 2017;23(2):185–190. doi:10.1177/1352458516671204 26. Marziniak M, Brichetto G, Feys P, Meyding-Lamadé U, Vernon K, Meuth SG. The use of digital and remote communication technologies as a tool for multiple sclerosis management: narrative review. JMIR Rehabil Assist Technol. 2018;5(1):e5. doi:10.2196/rehab.7805 27. Heesen C, Kasper J, Köpke S, Richter T, Segal J, Mühlhauser I. Informed shared decision making in multiple sclerosis—inevitable or impossible? J Neurol Sci 2007;259(1–2):109–117. doi:10.1016/J.JNS.2006.05.074 28. de Ceuninck van Capelle A, van der Meide H, FJH Vosman, Visser LH. A qualitative study assessing patient perspectives in the process of decision-making on disease modifying therapies (DMT's) in multiple sclerosis (MS). PLoS One. 2017;12(8):e0182806. doi:10.1371/journal.pone.0182806 29. Kremer IEH, Evers SMAA, Jongen PJ, van der Weijden T, van de Kolk I, Hiligsmann M. Identification and prioritization of important attributes of disease-modifying drugs in decision making among patients with multiple sclerosis: a nominal group technique and best-worst scaling. PloS One. 2016;11(11):e0164862. doi:10.1371/journal.pone.0164862 30. Cocco E, Caoci A, Lorefice L, Marrosu MG. Perception of risk and shared decision making process in multiple sclerosis. Expert Rev Neurother. 2017;17(2):173–180. doi:10.1080/14737175.2016.1217155 31. Cofield SS, Thomas N, Tyry T, Fox RJ, Salter A. Shared decision making and autonomy among US participants with multiple sclerosis in the NARCOMS registry. Int J MS Care. 2017;19(6):303–312. doi:10.7224/1537-2073.2016-091 32. Rahn AC, Solari A, Beckerman H, et al. “I will respect the autonomy of my patient”: a scoping review of shared decision making in multiple sclerosis. Int J MS Care. 2020;22(6):285–293. doi:10.7224/1537-2073.2020-027 33. Smith SG, Pandit A, Rush SR, Wolf MS, Simon CJ. The role of patient activation in preferences for shared decision making: results from a national survey of U.S. adults. J Health Commun. 2016;21(1):67–75. doi:10.1080/10810730.2015.1033115 34. Kasper J, Köpke S, Mühlhauser I, Nübling M, Heesen C. Informed shared decision making about immunotherapy for patients with multiple sclerosis (ISDIMS): a randomized controlled trial. Eur J Neurol. 2008;15(12):1345–1352. doi:10.1111/j.1468-1331.2008.02313.x 35. Stiggelbout AM, Pieterse AH, de Haes JCJM. Shared decision making: concepts, evidence, and practice. Patient Educ Couns. 2015;98(10):1172–1179. doi:10.1016/j.pec.2015.06.022
Comments (0)