
Remember me





A 61-year-old South-East Asian male presented to the Uveitis Service complaining of a decrease in vision in both eyes for a few weeks. His general health was unremarkable, and he denied any other symptoms/signs. The patient was high myopic with pseudophakia in both eyes and a past ocular history of diplopia related to decompensating left 4th nerve palsy, corrected with a Fresnel prism prescription. He underwent cataract surgery on the right eye in July and the left eye in September. One month after left eye surgery he reported that the vision in the right eye was not clear. On clinical examination, the best corrected visual acuity (BCVA) was 6/15 in both eyes. Intraocular pressure was 24 mmHg in the right eye and 23 mmHg in the left eye. Bilateral anterior segment examination revealed inferior keratic precipitates (KPs) and 0.5 + anterior chamber cells. On dilated fundoscopy, both eyes showed resolving cotton wool spots (CWS), located along the temporal arcades in the right eye and along the avascular arcade surrounding the optic disc in the left eye, in the absence of chorioretinal lesions (Fig. 1A). Vascular involvement was not clinically detectable. However, Optos ultra-widefield (UWF) fundus fluorescein angiography (FFA) showed bilateral vascular leakage and the absence of areas of capillary non-perfusion (Fig. 1B). The absence of choroidal involvement was confirmed by indocyanine green angiography (ICGA). Optical coherence tomography (OCT) showed a bilateral dry macula. The patient was diagnosed with bilateral anterior and intermediate uveitis. Full blood count, kidney and liver function, serum angiotensin-converting enzyme, C-reactive protein, erythrocyte sedimentation rate, antineutrophil cytoplasmic antibodies, antinuclear antibodies, anti-double stranded DNA antibodies, treponemal serology and Quantiferon TB Gold were all normal/negative. The patient was started on a tapering course of Prednisolone 0.8 mg/kg/day together with topical dexamethasone.
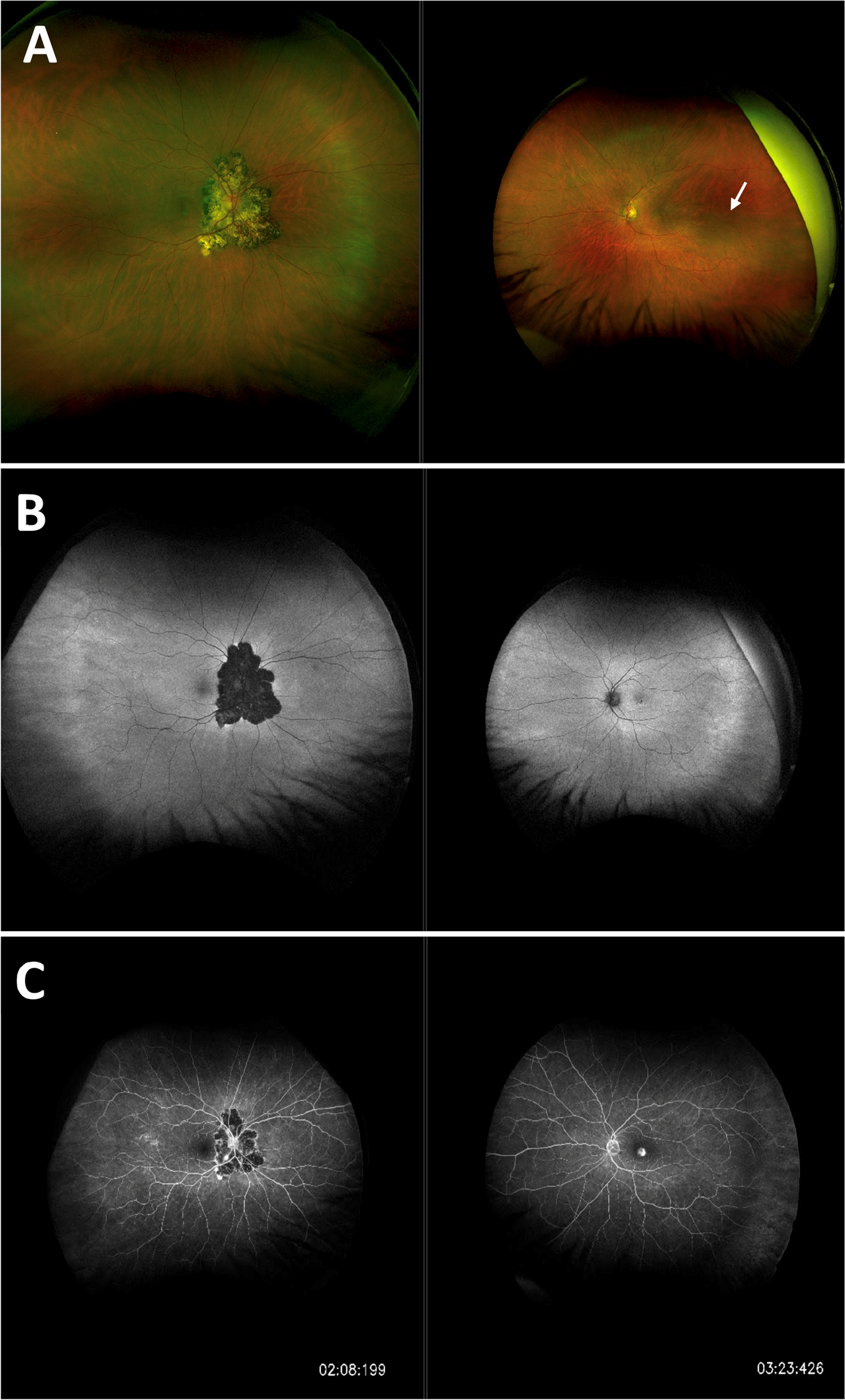
Fig. 1
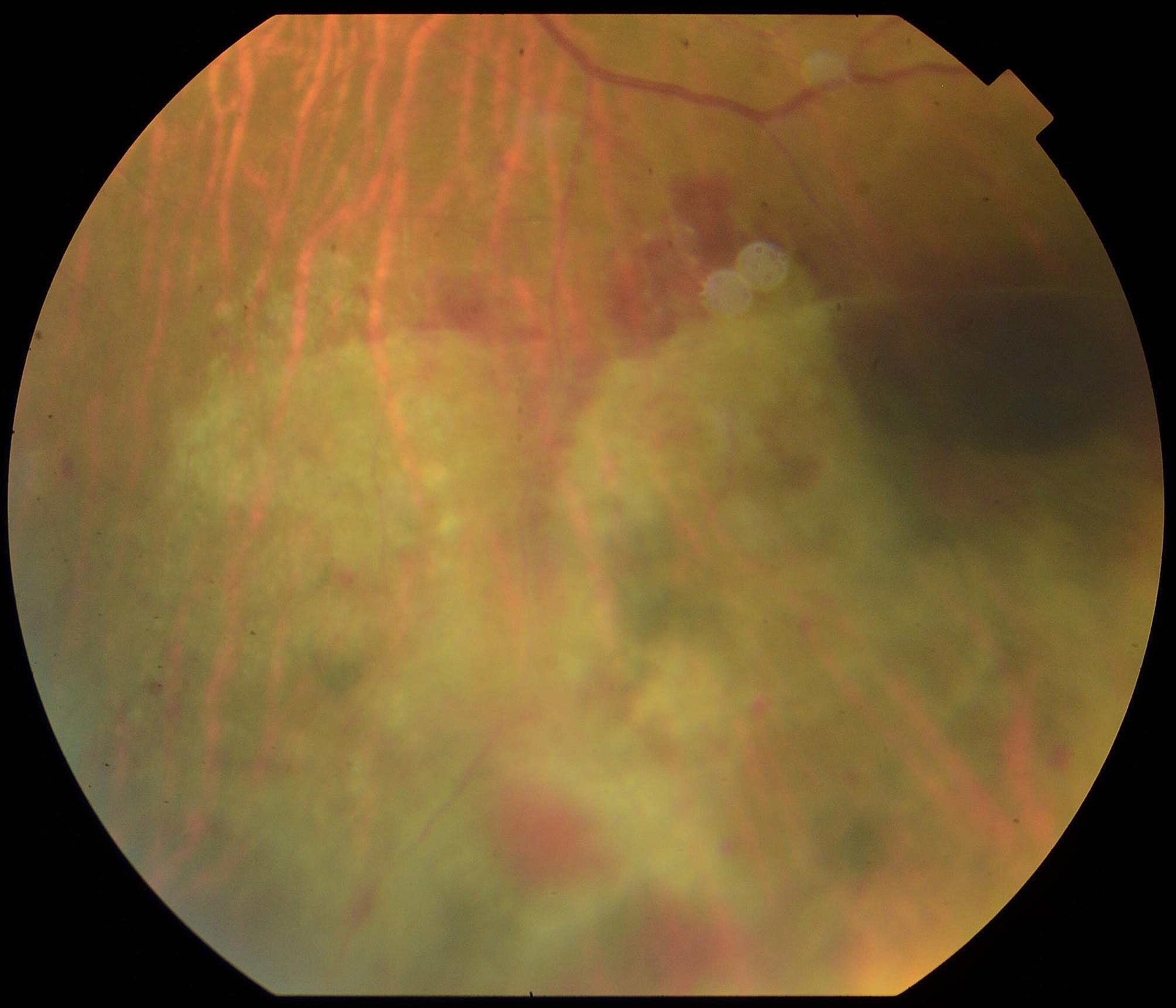
A Optos ultra-widefield pseudocolour fundus picture showing bilateral cotton wool spots, located along the temporal arcades in the right eye and along the avascular arcade surrounding the optic disc in the left eye. B Optos ultra-widefield fluorescein angiography showing bilateral vascular leakage in the absence of areas of capillary non-perfusion
At the 8-week follow-up, when the patient was on Prednisolone 10 mg/day, the ophthalmic examination did not show signs of intraocular inflammation, and a repeat of FFA showed bilateral residual peripheral vascular leakage and left persistent capillary leakage at the macula. A second-line immunomodulator steroid-sparing agent (mycophenolate mofetil) was started. Four weeks later, the patient came back with a bilateral decrease in visual acuity and high intraocular pressure in the right eye. The IOP was 28 mmHg in the right eye and 16 mmHg in the left eye. Both eyes showed 0.5 + anterior chamber cells with small KPs and unremarkable posterior segment examination. Lowering intraocular pressure eye drops and topical dexamethasone were started. Four-week follow-up showed no inflammation and normal intraocular pressure in both eyes. Eight weeks later, on MMF 1 g bd for 12 weeks and Prednisolone 7.5 mg/day, the patient presented again with decreased vision in both eyes. Ophthalmic examination revealed bilateral mild anterior chamber inflammation and new onset of bilateral vitritis. Prednisolone was therefore increased up to 40 mg once a day, and a decision to start Adalimumab was made. However, four weeks later, while waiting for the Adalimumab to be started, the patient presented with a bilateral reduction in vision (BCVA was 6/24 in the right eye and 3/60 in the left eye), normal intraocular pressure, corneal oedema with Descemet’s membrane folds and coin-shaped endothelial lesions (Fig. 2A), mild anterior chamber inflammation, and peripheral retinal haemorrhages (Fig. 2B). OCT showed a dry macula in both eyes. Ultra-widefield FFA showed bilateral severe occlusive vasculitis with peripheral areas of capillary non-perfusion (Fig. 2C). Based on the characteristic anterior segment features, CMV endotheliitis was suspected and an anterior chamber tap was performed. Aqueous polymerase chain reaction (PCR) analysis was positive for CMV. MMF was stopped, Ganciclovir 0.15% eye gel 5 times a day and Valganciclovir 900 mg bd were started, with topical and oral steroids continued. Two weeks later there was an improvement of the endotheliitis with near complete resolution of the coin-shaped lesions. Corneal oedema had improved but was not completely resolved. Repeated ultra-widefield FFA at 8 weeks showed significant peripheral ischemia in both eyes, requiring laser panretinal photocoagulation. The patient continued on a maintenance dose of Valganciclovir tablets 450 mg twice a day. 6 weeks later, his right cornea was almost completely clear, but the left still showed inferior oedema. BCVA was 6/12 in the right eye and 6/24 in the left eye. The first laser panretinal photocoagulation session was performed in both eyes.
Fig. 2
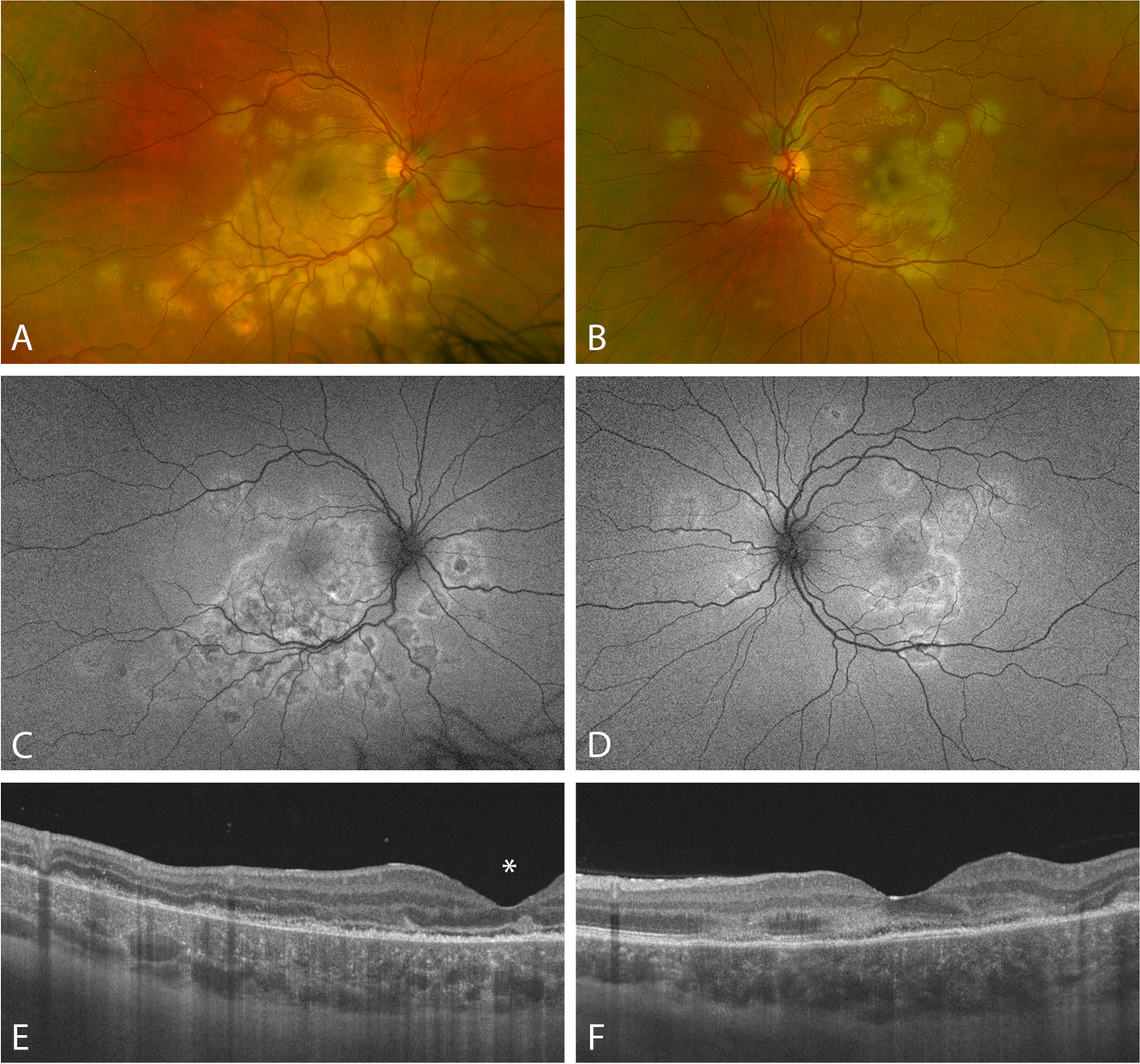
A Topcon anterior segment photographs of both eyes showing CMV endotheliitis with Descemet’s membrane folds (white arrow), corneal oedema (asterisk), and coin-shaped keratic precipitates (white arrowheads). B Optos ultra-widefield pseudocolour fundus picture showing bilateral peripheral retinal hemorrhages. C Optos ultra-widefield fluorescein angiography (early and late phases) showing bilateral severe occlusive vasculitis with peripheral areas of capillary non-perfusion
Comments (0)