
記住我
Allogeneic, xenogeneic, and synthetic bone have been widely used in dentistry. Among them, synthetic bone has a lower risk of cross-infection and is more competitively priced than the others. However, the clinical use of synthetic bone graft materials is limited because of their structural properties and decreased osteogenic activities [7].
A new synthetic material, beta-TCP, has recently gained popularity owing to its high biocompatibility [11] and osteogenic potential [12, 13]. Nonetheless, it has poor mechanical strength and is easily absorbed [14]; hence, it is usually applied as a mixture with HA to improve the mechanical properties while maintaining the graft volume. HA cannot be replaced with natural bone at the graft site; therefore, a new technology was applied to develop a pure beta-TCP with improved mechanical strength and a lower resorption rate [15, 16].
Neo Bone® is manufactured using the nanocrystal particle treatment method [16], which increases the mechanical strength of the pure beta-TCP by forming uniform particles [17]. Neo Bone® can preserve the high osteogenic potential (osteoconduction and osteoblast activation) of beta-TCP. It ensures high chemical purity and uniformity of the chemical composition and crystal phase by calcifying beta-TCP below the phase transition temperature to minimize the aggregation of raw materials. The micro-crystal coating between the beta-TCP particles guarantees uniformity and improves the mechanical strength and brittleness, so it is not easily broken [17].
Beta-TCP is absorbed by macrophages and multinucleated giant cells [18, 19]. In one study, the volume retention rate of NeoBone® was higher than those of an allogeneic bone graft (survival rate of 80.3% at 6 months after surgery) and a 1:1 mixture of allogeneic and xenogeneic bone (84.1%), thus acting as a scaffold [20]. In another study using conventional pure beta-TCPs, 75.6% of the original graft area was retained 6 months after surgery [20, 21]. Interestingly, 97.5% ± 26.8 of the original graft area remained 6 months after surgery in the current study. This finding indicates that Neo Bone® can achieve preservation of the volume by overcoming the disadvantages of conventional pure beta-TCP grafts. NeoBone® showed a higher volume retention rate 6 months after surgery than the hydroxyapatite and beta-TCP mixture, which retained 82% of the original graft area [17]. Thus, Neo Bone® has served as a support for an extended period until new bone was formed, while the implanted bone was resorbed during the osteosynthesis period. Furthermore, it overcame the clinical weaknesses of existing pure beta-TCP grafts, maintained the volume and height of the bone graft site after surgery, and achieved better volume preservation compared to other bone graft materials.
Conventionally, a mixture of hydroxyapatite and beta-TCP has been used to maintain the volume of the implantation site and improve the mechanical properties [11, 18, 19]. However, conventional synthetic bone to which HA is added has a disadvantage in that the implant must remain in the body for life after bone transplantation. Alternatively, the pure beta-TCP used in the present study not only serves as an adequate scaffold for new bone formation when used alone, but also has the advantage of significantly lowering the possibility of infection caused by the complete absorption of implants at a later point. The findings of the present study indicate that Neo Bone® may be considered as an alternative to a successful bone graft material in various dental surgery cases.
According to the radiological findings, 97.5% ± 26.8% of the Neo Bone® graft area supported volume preservation until 6 months after surgery, and most of the 25 patients had the same or increased relative bone density values. Thus, the graft was gradually replaced by new bone after 6 months.
Histomorphometric analysis to confirm the formation of new bone tissue was not performed for ethical reasons. However, previous studies have reported these findings using histomorphometric analyses of beta-TCP and radiologic evaluations [16, 22].
Okada et al. found that high-purity beta-TCP is safe with excellent osteoconductive properties, even in patients who underwent maxillary sinus augmentation with beta-TCP alone [20] Furthermore, a histological analysis comparing beta-TCP with other materials showed that the rate of new bone formation was significantly increased between 6 months and 1 year, followed by a significant decrease. These findings were corroborated in the present study. Thus, the radiologic data in this study might represent new bone formation in the defect. The relative bone density of the graft was similar to or increased with time when compared to that of the surrounding bone (Table 6). This change in graft density implies that some degree of bone regeneration has progressed into the graft area during the observation period. A retrospective study using a beta-TCP bone graft showed similar results under favorable conditions [23].
Dentoalveolar bone grafting is mainly performed by elevating the oral mucosa in the oral cavity. The oral cavity consists of a large number of bacteria and is exposed to masticatory forces. Furthermore, the mucosa covering the upper part of the graft is mechanically weaker than the skin or muscle layer. These factors increase the likelihood of wound dehiscence at the graft site. Therefore, the infection rate after bone graft during dental treatment is high, and it is expected to be higher in the case of synthetic bone [24]. Accordingly, postoperative systemic antibiotics have been prescribed to reduce infection [25]. No infection or wound dehiscence was observed in the present study; this, Neo Bone® might prove to be biocompatible with the oral mucosa.
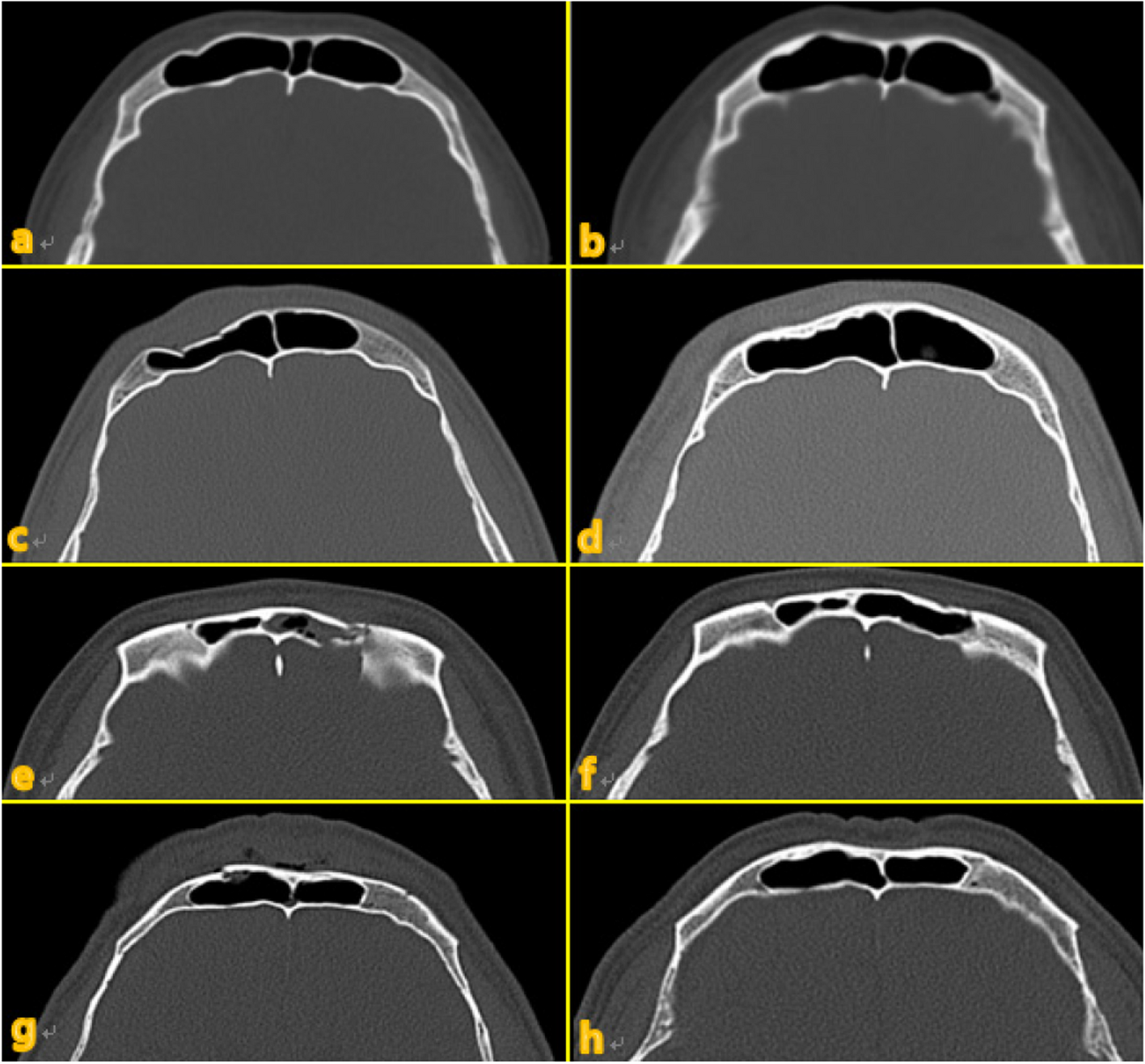
The beta-TCP used in this study has the advantage of being able to gradually replace the scaffold with new bone while maintaining its role for a sufficient period of time, unlike conventional beta-TCP. As shown in Fig. 4, it was confirmed that the volume was well maintained up to 6 months after surgery even in CBCT. However, this study has limitations as it did not include histological examination and did not use a control group for retrospective analysis. Therefore, prospective comparative studies with control groups and histological examinations will be necessary in the future.
Fig. 4
Preoperative and postoperative cone beam CT
留言 (0)