
記住我
Maxillary expansion has been a common practice for orthodontists to correct maxillary transverse discrepancy and aid in space generation to help alleviate crowding during Phase I orthodontic treatment. Conventionally, heavy orthopedic forces have been applied to separate the midpalatal suture and other surrounding sutures to expand the maxilla.[1] Indications for maxillary expansion include the need to correct a posterior crossbite, to correct an arch-width discrepancy between the maxilla and the mandible. More recently, it has been noted that a potential beneficial side effect of expansion can be increased airway volume.[2] During the growth phase, craniofacial bones are considered malleable structures and lack the interdigitation of maxillary sutures due to which they can be easily modified to generate skeletal changes.[3,4] Starnbach et al. suggested that maximum maxillary expansion can be achieved with the use of various removable or fixed appliances during a critical period when cranial sutures have not fused in children.[5]
Crossbites occur when the maxillary dentition has a greater amount of constriction relative to the mandibular dentition or when maxillary width is within the normal limits and the mandible is wider than its normal range, especially in cases of skeletal class III malocclusion with prognathic mandibles. To date, the treatment of choice to correct posterior crossbites is maxillary expansion using rapid or slow maxillary expansion (SME).[6] Rapid maxillary expansion (RME) has usually been defined as two activations per day, or about 0.5 mm expansion/day.[7] SME achieves similar results compared to RME with less force applied over a longer period. If using a jackscrew device, SME can be achieved with one activation, or 0.25 mm expansion/day, every other day.[3] The mechanism of action behind SME is based on both midpalatal suture and surrounding tissues, working to separate the suture to achieve greater transverse width.
Many studies have analyzed the benefits and impact of traditional means of maxillary expansion, such as a Hyrax, quad helix, or Schwartz appliance. However, the efficacy of skeletal expansion and dentoalveolar movement resulting from Phase I clear aligner treatment has not been evaluated. In the past three decades, clear aligners have become an integral component of orthodontic treatment. Invisalign® and, now, many other clear aligner systems use gentle and continuous orthodontic forces to move teeth. Dental caries is the most prevalent disease seen in young patients; thus, improved oral hygiene is an attractive benefit of aligner use.[8,9] As a result, clear aligner companies have expanded to provide Phase I treatment to pre-adolescent and adolescent patients. Because aligners can be removed and individuals are able to floss between teeth, periodontal health has also been noted to be improved with clear aligner treatment.[10] Based on the increasing use of clear aligners by both orthodontists and general dentists, clear aligner treatment will be adapted to a wide variety of dental conditions.
The aim of this study was to assess maxillary expansion in Phase I orthodontic treatment with clear aligners and to perform model analysis on pre-treatment and post-treatment intraoral scans to determine total movement of the dentition. We also compared post-treatment intraoral scans with the planned treatment as prescribed using Invisalign ClinCheck® to obtain a percent yield of expansion in both the canine and the molar area. Moreover, we analyzed pre-treatment and post-treatment cone-beam computed tomographies (CBCTs) to measure molar tipping, intermolar distance, canine tipping, and intercanine distance. The null hypothesis was that there would be no difference in the prescribed and actual maxillary expansion using clear aligners in the growing mixed dentition patients.
MATERIAL AND METHODS Sample populationA sample of 54 patients was selected and all were treated at one location, a private practice orthodontic office in San Francisco between August 2016 and February 2020 with clear aligners through the Invisalign® platform. All patients had to fit certain inclusion criteria to be included in this study – patients with mixed dentition, no history of previous orthodontic treatment, before and after intraoral scans, had to have some kind of expansion planned, and had to be treated with clear aligners only. Patients that had any craniofacial abnormalities, history of trauma, or were unable to complete treatment with clear aligners only were excluded from this study.
Intraoral scanning and CBCTAll intraoral scans were captured with an iTero Element or iTero Element 2 intraoral scanner. The iTero Element 2 replaced the iTero Element in 2018, so the patients who had scans after this year had them done on the iTero Element 2. CBCT images were taken in a 16 × 13 cm field of view using an iCAT FLX (Henry Schein Dental). The voxel size used was 0.3 mm and each scan required 8.9 s with total exposure of 623.9 mGy/cm^2. All patients were seated upright, and the chin was positioned in the chin cup with adjustments made to the chair height to align the horizontal laser light to match the patient’s smile line. All patients were informed to swallow, bite down into centric occlusion, and to remain still. The occlusal plane was set to match the tragus-ala line in the horizontal dimension.
Clear aligner platformAll treatments rendered were completed using Invisalign® (AlignTech). Invisalign First® was available for use in 2018; therefore, Invisalign Teen® was used for the cases that started before 2018. All patients had anywhere from 1 to 6 sets of aligners delivered over the course of treatment. The average number of aligner sets delivered was 2.44. Any warranty sets that had no changes to the tooth movements but had to be sent for unforeseen circumstances (e.g., lost, defective, and non-tracking aligners) were not included in the sets that we tallied.
Morphometric data collectionAll digital cast measurements were performed using the measurement tool in OrthoCAD version 5.9.0.36 (copyrighted by Align Technology, 2016). The intermolar distance was measured between the mesiolingual cusps of the maxillary 1st permanent molars [Figure 1]. The intercanine distance was measured between the cusp tips of the maxillary primary canines [Figure 1]. In the event that one or both of the primary canines were missing on the initial or final intraoral scans, the measurement was done from the center of the alveolar ridge at the position where the primary canine would be. All tooth measurements were performed in ClinCheck® Pro 5 using the grid measurement tool to quantify the prescribed interdental expansion. All planned measurements were taken from the last active aligner from the last refinement treatment plan accepted.

Figure 1:: Digital cast intermolar and intercanine width.
Export to PPT
CBCTs were analyzed using Anatomage Invivo6 with a custom configuration with plotted anatomical landmarks. The configuration inputted these landmarks to give specific measurements on the pre-treatment and post-treatment CBCTs. These measurements were as follows: Upper 1st Molar Cusp Width [Figure 2], Upper 1st Molar Cementoenamel Junction (CEJ) Width [Figure 2], Intermolar Angle [Figure 2], Upper Primary Canine Cusp Width [Figure 3], Upper Primary Canine CEJ Width [Figure 3], and Intercanine Angle [Figure 3]. The intermolar width measurement was defined as the distance between the mesiolingual cusps of the maxillary 1st permanent molars. The intercanine CEJ width measurement was defined as the distance between the CEJs at the cingulum of the maxillary primary canines. In the event that one or both of the primary canines were missing on the initial or final CBCT, the measurement was done from the center of the alveolar ridge at the lingual boundary of the alveolar bone. The intermolar and intercanine angles were also measured to access the change in the pre- and post-treatment molar and canine angulations. The intermolar angle was measured from the angle of intersecting lines tangent to the mesiobuccal and mesiolingual cusp tips of the maxillary right and left first permanent molars [Figure 2]. The intercanine angle was measured from the angle of intersecting lines following the long axis of the primary canines [Figure 3]. In the event, one of the primary canines was missing on the initial or final CBCT, a line was constructed from the center of the alveolar ridge to the cusp tip of the permanent canine. This line would then be used as an estimate for the long axis of the primary canine had it been present.[11-13]

Figure 2:: (a-c) Molar intercuspal width, molar cementoenamel junction width, and molar angle.
Export to PPT

Figure 3:: (a-c) Intercanine width, intercanine cementoenamel junction width, and canine angle.
Export to PPT
Statistical analysisStata Software was used for statistical analyses for both the model and CBCT analyses. For model analysis, an exact Wilcoxon signed-rank test was used to compare the samples and assess whether the population mean ranks differ. This test was used to measure two aspects of the before and after models – changes in the intermolar and intercanine distances from the prescribed expansion in ClinCheck® compared to the actual expansion. The null hypothesis was that the planned expansion was equal to the actual amount of expansion. Because multiple tests were performed on the same sample, Bonferroni’s method was used to correct for the traditional p-value threshold of P < 0.05. Since two tests were performed, one for the intermolar distance and another for the intercanine distance, the threshold for this test was set at P < 0.025. To compare female and male samples, a two-sample Wilcoxon rank sum test was used for sex-specific analysis. The null hypothesis was that there would be no significant difference between female and male patients.
For CBCT analysis, an exact Wilcoxon signed-rank test was used to compare six measurements of the before and after CBCTs, as stated above. To reiterate, these measurements were (1) changes in the intermolar distance, (2) changes in the intermolar angle, (3) changes in the intermolar CEJ distance, (4) changes in the intercanine CEJ distance, (5) changes in the intercanine distance, and (6) changes in the intercanine angle. The null hypothesis was that there would be no significant difference between pre- and post-treatment measurements. It is important to note that p-value was not corrected for multiple comparisons. To ensure the accuracy of data collection, a Spearman rank correlation test was done to compare interobserver error and the null hypothesis was that there would be no differences in measurements of the two observers.
RESULTSTo perform model analysis to compare differences in prescribed versus actual maxillary expansion, 54 patients (22 females, 40.74%; and 32 males, 59.26%) with an age range between 7 years, 7 months old and 11 years, 6 months old (average age = 8.77 years) were analyzed. The estimated treatment time ranged from 6 to 24 months with an average of 13.44 months. The actual treatment time ranged from 2 months, 27 days to 20 months, and 22 days with an average of 10.11 months. For CBCT analysis, 29 patients (14 females, 48.28%; and 15 males, 51.72%) with an age range between 7 years, 7 months old and 11 years, 6 months old (average age = 8.91 years). The decrease in the number of patients for CBCT analysis was due to the lack of a post-treatment CBCTs for the 24 excluded patients. The estimated treatment time for the 29 patients ranged from 6 months to 24 months with an average of 13.86 months. The actual treatment time ranged from 5 months, 15 days to 20 months, and 22 days with an average of 11.25 months. Of the 29 patients, 12 had their post-treatment CBCTs taken within 1 month of their treatment completion, whereas 17 had post-treatment CBCTs ranged between 3 months and 9 days to 28 months and 14 days. As a result, a statistical test to account for time was included in this project.
Phase I treatment of all 54 patients was completed during the study with the clear aligners. On average, the estimated prescribed treatment time was 13.44 months and the average patient completed treatment in 10.11 months. Therefore, the overall treatment time was decreased by an average of 3.33 months. However, 7 patients (12.96%) exceeded the estimated treatment time. Sex was not observed to be a significant predictor of expansion success due to intermolar change P = 0.058 and intercanine change P = 0.329. Therefore, we accepted the null hypothesis since no significant sex-specific differences were observed. However, intermolar changes tended to be greater in males compared to females.
Digital model findings and comparison with Clincheck® setupUsing the landmarks [Figure 1] to measure intermolar and intercanine distances, all 54 patients showed at least some amount of dentoalveolar expansion in the posterior region. The expansion ranged from 0.25 mm to 6.10 mm. When including all 54 samples, there was an average expansion of the maxillary molars of ~2.4 mm [Figure 4]. Because not all patients necessitate expansion as part of the treatment, a percent yield of expansion was calculated to determine the predictability of achieving the planned expansion in the posterior region. ClinCheck® estimated an average planned expansion of 5.22 mm between the maxillary molars [Figure 4]. The actual maxillary, posterior expansion was determined to be 2.67 mm or 51.15% of the estimated expansion.

Figure 4:: Planned versus actual maxillary molar expansion.
Export to PPT
When analyzing the maxillary primary canine region, 53 out of the 54 patients showed dentoalveolar expansion in the anterior region [Figure 5]. The expansion ranged from 0.15 mm to 11.3 mm. The lone patient who did not show any expansion also did not show any constriction, and the treatment plan was to maintain the intercanine dimension, which was reflected in a 100% yield of the planned movements. When including all 54 samples, there was an average expansion of the maxillary primary canines of 4.01 mm [Figure 5]. A percent yield of expansion was again calculated to determine how predictable clear aligner treatment is at achieving planned expansion in the anterior region. ClinCheck® estimated an average planned expansion of 5.88 mm between the primary canines [Figure 5]. The actual maxillary, posterior expansion was determined to be 3.80 mm or 64.73% of the estimated expansion.
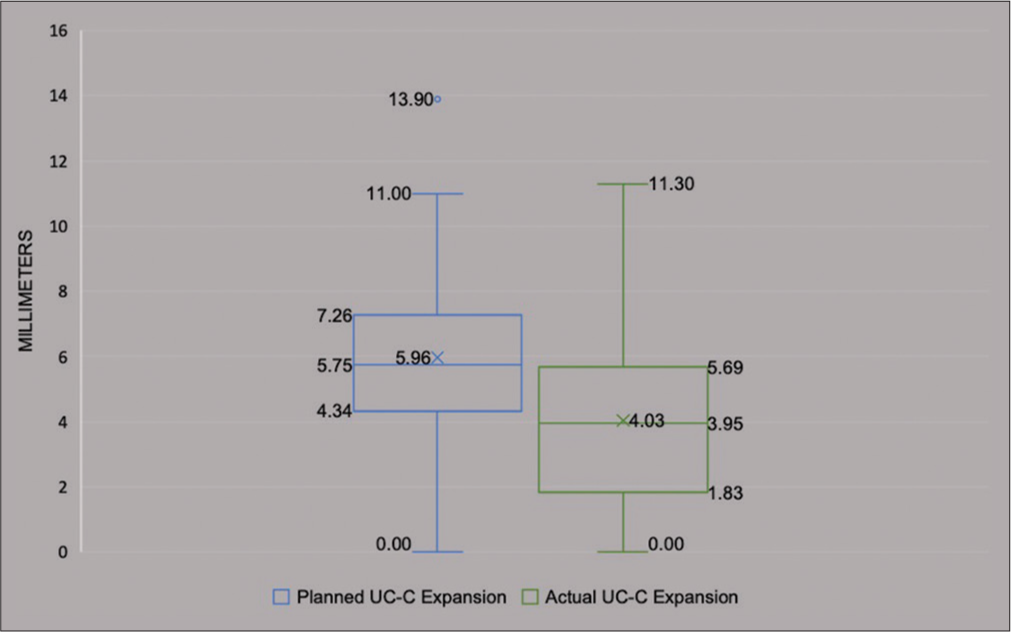
Figure 5:: Planned versus actual maxillary primary canine expansion.
Export to PPT
CBCT findingsMeasurements of intermolar distances [Figure 2] showed an average expansion of 1.89 mm for the 29 samples. When accounting for time, there was about a 0.05 mm decrease per month [Figure 6] after treatment was completed, but statistical analysis showed that this decrease over time was not significant. Intermolar CEJ distances [Figure 2] showed an average expansion of 1.87 mm for the 29 samples with ~0.03 mm decrease per month post-treatment, and statistical analysis showed that this decrease may be correlated with time. The intermolar angle [Figure 2] decreased ~1.16° for the 29 samples showing that the permanent first molars had tipped buccally by about 1.16° post-treatment. When accounting for time, there was about a 0.2° increase per month after treatment was completed. This suggests that the molars uprighted gradually over time after treatment completion, but statistical analysis deemed this increase over time to be not significant. Using the landmarks to measure the intercanine distances [Figure 3], there was an average expansion of about 3.64 mm for the 29 samples with ~0.12 mm decrease per month post-treatment, and statistical analysis showed that this decrease is in part due to time. Intercanine CEJ distances showed an average expansion of ~1.78 mm for the 29 samples with ~0.21 mm decrease per month post-treatment, and statistical analysis showed that this decrease may be correlated with time. Intercanine angle increased ~24.73° for the 29 samples showing that the primary canines had tipped buccally by ~24.73° post-treatment with ~0.016° decrease per month. This suggests that the primary canines uprighted gradually over time, but statistical analysis showed that this increase over time was not significant.
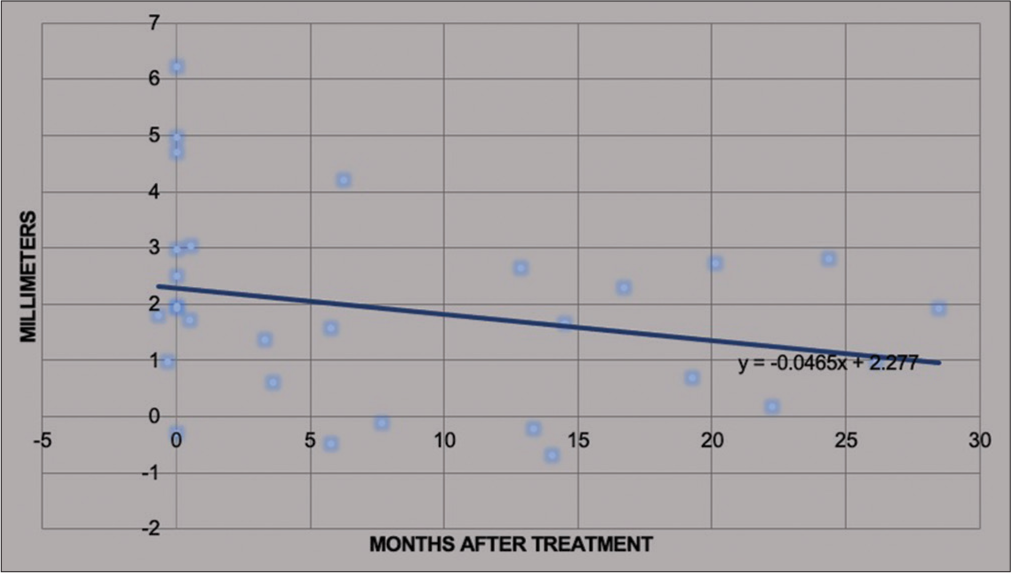
Figure 6:: Maxillary molar expansion change over time.
Export to PPT
DISCUSSIONWhen analyzing the samples, it is apparent that clear aligner treatment can yield maxillary dentoalveolar expansion. This study found that amount to be ~2.4 mm in the posterior and ~4.01 mm anteriorly. Other authors have found about 5 mm of expansion from increased intermolar width using SME and ~5.5 mm using RME.[13-16] Therefore, based on the model analysis, clear aligner treatment appears to provide predictable expansion to some degree. Based on the results, the anterior maxilla at the canine region had about 1.61 mm greater expansion compared to the posterior maxilla. This pattern of expansion is like the triangular pattern seen in traditional rapid and SME.[17]
The significance of the planned expansion seen in the ClinCheck® setup can provide insight as to how much to program when trying to achieve predictable results. Our results showed that the intermolar percent yield of expansion was about 51.15% while the intercanine percent yield of expansion was about 64.73%. This means that a treating orthodontist can expect to gain anywhere from about half to about 65% of what the ClinCheck® shows. One important aspect to consider is the instructions given to the Invisalign® technician. Due to Invisalign’s® customizable design, clinicians are able to specify how much expansion they would like. In our patient sample, the expansion varied for each patient. For example, the treating orthodontist specified 2 mm of expansion bilaterally for some patients and 8 mm of bilateral expansion for others.
Huynh et al. found that about a third of expansion was lost after treatment completion.[13] They also noted that retention was critical in maintaining arch width and decreased relapse by about 1 mm 2 years after treatment completion.[13] In putting this into perspective with clear aligner treatment, it is feasible that 51.15–64.73% of expansion was maintained post-treatment compared to the ClinCheck® set-up. Based on our results, it can be inferred that overtreating the expansion of the maxilla is warranted to achieve predictable results. Our results showed that it is possible to have about 0.047 mm of relapse in the intermolar cusp dimension per month, 0.026 mm of relapse in the intermolar CEJ dimension per month, 0.12 mm of relapse in the intercanine cusp dimension per month, and 0.21 mm of relapse in the intercanine cusp dimension per month. Of course, this has some confounding variables. First, none of the patients have post-retention records of their own to track how much expansion remains. Second, the protocol for each patient was variable, so comparing these samples may not be the best indication of potential relapse. Therefore, this observed decrease in arch dimension is simply a trend observed from our patient population, but future studies should consider post-retention records to observe long-term stability of expansion from the use of clear aligners.
From our data collection, the maxillary molars were shown to have an average buccal tipping of 0.58° after treatment with clear aligners. This is significantly less than the 2.3° seen with traditional slow maxillary expanders and the 3.7° seen using a hyrax.[13,18] When examining the change in molar inclination over time, the trendline suggests that about 0.1° of molar uprighting may occur per month after treatment occurs. Other studies have found the uprighting of molars to be about 6° after 2 years of retention and 3.3° of uprighting naturally when transitioning from mixed dentition to permanent dentition.[13,19] The maxillary primary canines were seen to flare buccally by about 12.37°. This change is seen to be relatively consistent despite time. There was only about a 0.01° angle change per month seen based on our sample. A possible explanation for this higher degree of tip is due to the pattern of exfoliation of primary dentition. The maxillary canine usually erupts lingually relative to the maxillary primary canine.[20] This pattern tilts the primary canine crown toward the cheek and increases the buccal crown flaring. Therefore, this angle is not very indicative of maxillary expansion.
The previous studies have demonstrated that patients treated for expansion at a younger age maintain their expansion more relative to those who were treated at an older age.[13,17] This is possibly due to the increased interdigitation of sutures leading to patient’s being more prone to expansion loss.[17,21] Given that clear aligners may be more tolerable for younger patients in comparison to traditional maxillary expanders, clear aligners can be a solution to provide treatment in that niche population that would not accept any other form of treatment.[22]
CONCLUSIONMaxillary expansion can be achieved reliably with clear aligner therapy during Phase I orthodontic treatment. This study provides an overall introduction to the capabilities of Phase I orthodontic treatment with clear aligners and has also shown that maxillary expansion does occur through the use of clear aligners. Further, research analyzing a more specific patient population will provide further insight on this topic.
留言 (0)