
Remember me
Class II malocclusions are common and constitute a significant proportion of patients seeking orthodontic treatment.[1] In the treatment of Class II malocclusions, there are several treatment methods depending on the etiology of the malocclusion.[2] Growth modification with functional appliance therapy is a common first-phase treatment modality for patients in the growth development phase.[3] After the first phase of treatment, a second phase of treatment is usually applied with fixed orthodontic appliances to correct crowding and improve occlusion.
In Class II div 1 patients with an increased mandibular plane angle and lower facial height, it is known that the combination therapy of a high-pull headgear and a functional appliance in the late permanent dentition causes inhibition of anterior growth of the maxilla, inhibition of mesial and vertical displacement of the maxillary teeth, development of the mandibular posterior teeth, condylar and glenoid remodeling.[4] However, the effect of functional appliances on Class II patients has been reported to be controversial.[3] Many studies have suggested that functional treatment has a minimal skeletal effect, its effect is primarily dentoalveolar and the growth-modifying effects may not be long-lasting.[1,5]
Camouflage treatments are another treatment option for Class II malocclusions, usually including pre-molar extractions.[6] Extraction of two or four pre-molars corrects crowding, aligns teeth, and corrects overjet and procline incisor positions. In Class II patients with crowding and/or convex profile and difficulty closing the lips, pre-molar extraction is recommended to correct crowding and improve the patient’s profile.[7,8]
Identical (monozygotic) twins have the same genotype and tend to show the same phenotypic traits. However, depending on epigenetic effects and environmental factors, there may be changes in the phenotypic patterns of individuals.[9,10] Despite the known effects of functional appliance therapy and camouflage therapy, to the best of our knowledge, there are no studies in the literature on the comparative effects of these treatments in twin patients. Therefore, the key question of our study is: “Are the skeletal, dental, or esthetic outcomes of a one-phase camouflage treatment with pre-molar extraction different from a two-phase treatment with functional appliances followed by fixed orthodontic treatment in monozygotic twins?”
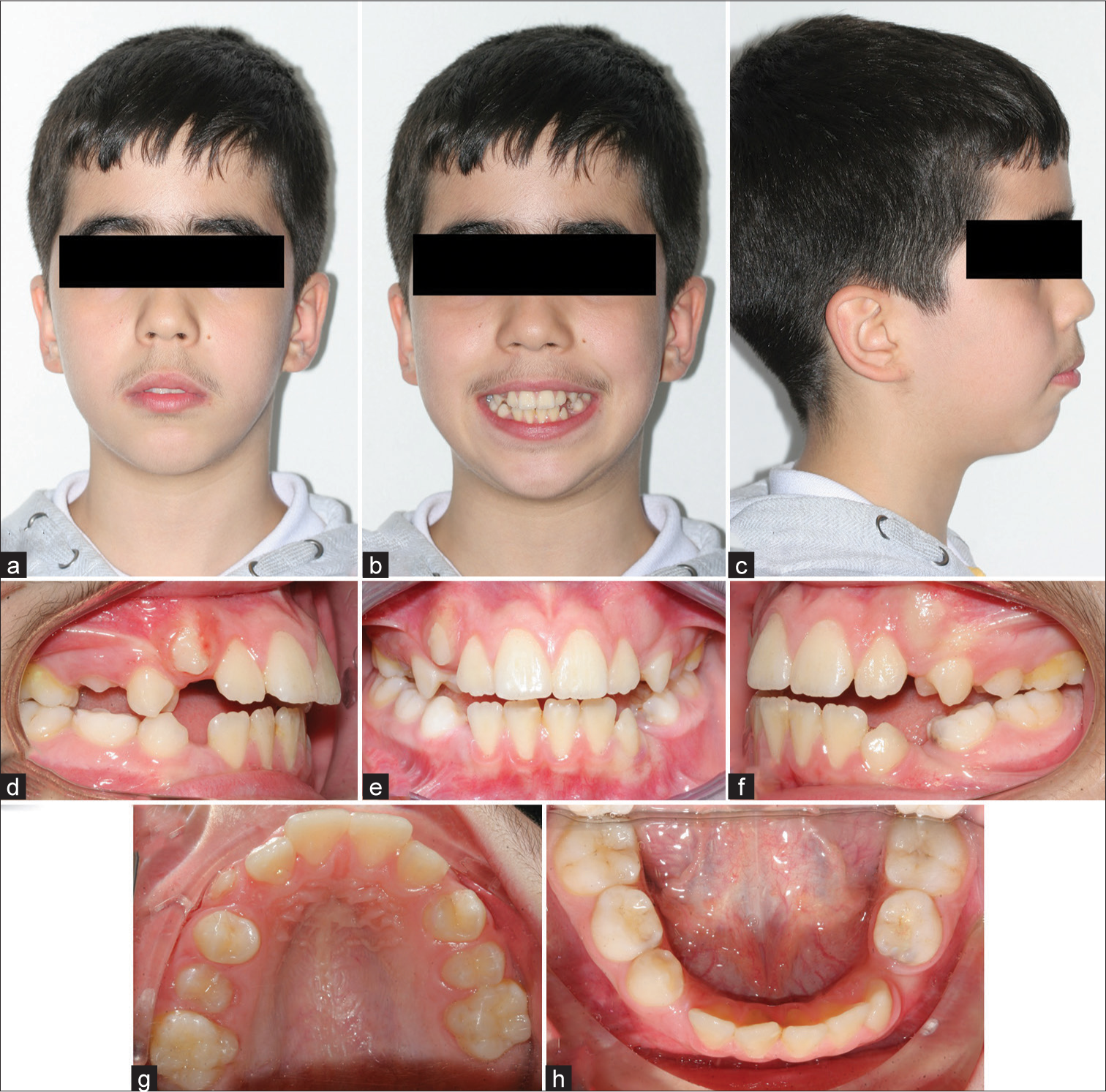
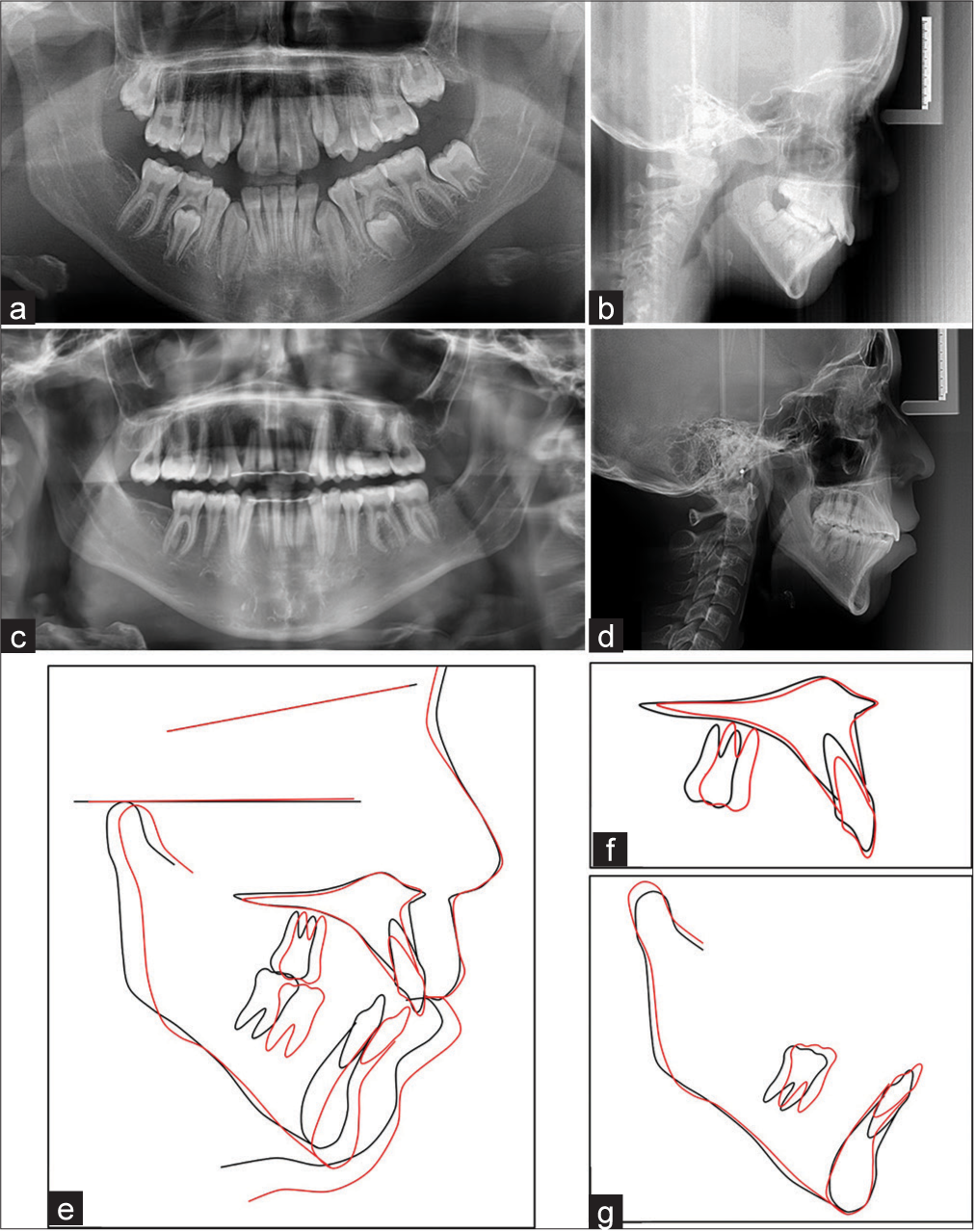
CASE REPORT12-year-old male monozygotic twins presented to the dental clinic with complaints about their anterior teeth. Patients were in the pubertal period. Intraoral examination revealed that the patients were in the late mixed dentition stage. In Patient 1, a Class II relationship was observed in the right and left molars. In Patient 2, the right molar relationship was Class II, while the left molar relationship was Class III due to the early loss of deciduous tooth number 74. Extraoral examination of the patients revealed forward angulation of the lower lip, incompetence of lip seal, and a convex profile. Intraoral and extraoral photographs of Patient 1 pre-treatment are shown in [Figure 1], and intraoral and extraoral photographs of Patient 2 pre-treatment are shown in [Figure 2]. In a panoramic radiological examination of patients, it was observed that there was no tooth germination of tooth number 47. Pre-treatment cephalometric measurement values are shown in [Table 1]. Cephalometrically, their skeletal-facial types were classified as Class II div 1 long-face types (gonial angle, mandibular plane angle, and lower facial elevation were increased).
Table 1: Lateral cephalometric measurements.
Variables Patient 1 Patient 2 Pre-treatment Post-treatment Pre-treatment Post-treatment Skeletal Variables SNA (°) 74 75.9 74.7 79.5 SNB (°) 70.18 73.3 70.59 72.9 ANB (°) 3.82 2.6 4.11 6.6 NV-A (mm) −6 −4.1 −6.20 −0.4 NV-Pog (mm) −22.01 −14.4 −22 −16.37 Occlusal plane angle (SN/Occ°) 22 23.88 23.43 25.36 Mandibular plane angle (SN/Go-Gn°) 46.56 46.37 47.85 50 Dental Variables U1/SN (°) 97.09 96.2 103.81 94.68 U1/NA(°) 21.38 21.1 28.29 21.02 U1-NA (mm) 5.11 7 7.87 4.96 L1/GOGN(°) 88,5 95.3 88,7 80.1 L1/NB (°) 29.9 34.24 27.29 23.6 L1-NB (mm) 6.6 9.5 9.29 5.2 U1/L1 (°) 122.6 117.8 124.8 138.9 Soft-tissue variables Ls-E line (mm) 3 1.7 2.4 0.4 Li-E line (mm) 3.4 4.1 3.5 3.1 Nasolabial angle (°) 103.74 103.35 104.82 104.9 Upper lip length1 (mm) 26.7 29.0 26 28.1 Upper lip thickness2 (mm) 10 10 11.9 13.2 Lower lip length3 (mm) 41.4 53.1 41.5 51.5 Lower lip thickness4 (mm) 15.1 14.3 14.2 15.2
Export to PPT
Export to PPT
Treatment objectivesThe treatment objectives for Patient 1 were (1) phase 1 treatment involving inhibits the vertical growth of the maxilla, controls the eruption of the molars, and promotes the growth of the mandible; (2) achieve a Class I relationship between the canines and molars with the extraction of the pre-molars; (3) phase 2 treatment involving fixed appliance treatment to correct remaining orthodontic problems; and (4) retention.
The treatment objectives for Patient 2 were (1) achieve a Class I relationship between the canines and molars with the extraction of the pre-molars, (2) correct the increased overjet and decreased bite, (3) create enough space for the eruption of teeth number 23 and 43, (4) place the procline incisors in the correct position, and (5) retention.
Treatment alternativesA two-phase treatment was planned. The use of a high-pull headgear combined with a twin block to correct skeletal anteroposterior and vertical malocclusions with growth modification and then fixed orthodontic treatment was planned. However, problems related to some factors, such as psychosocial and behavioral factors, complexity, and duration of treatment, may occur in early appliance treatments.[7] Patient 2 did not comply with the treatment, complaining that the use of the device could cause esthetic problems and difficulties in use. Therefore, camouflage treatment with extraction of four pre-molars was planned as another treatment option for Class II patients in Patient 2.
Treatment progressSigned consent forms were obtained from the parents for the treatment of the patients.
Patient 1A wax bite was recorded to position the mandible approximately 6 mm anteriorly and 4–5 mm interocclusal vertically at the level of the first pre-molars, and the twin block was prepared in the laboratory. For the high-pull headgear, right and left tubes were placed on the occlusal surface of tooth 5 on the upper part of the twin block. The extraoral arms of the headgear were angled upward by 25– 30° so that they were at the level of the second pre-molars, to transfer the force through the center of resistance of the maxilla and maxillary dentition. The patient was instructed to use the twin-block appliance full time, except for meals and sports activities, and to use the high pull headgear with a force of 550–600 g for 12–16 h. After six months of appliance use, the canine and molar Class I relationship was achieved, and fixed orthodontic treatment was started. In fixed orthodontic treatment, a 0.18-inch slot Roth braces system was used.
Patient 2A 0.18-inch slot Roth braces system was used for fixed orthodontic treatment. After the extraction of four premolars, the canines were distalized by loop bending using the segmental arch technique. After distalization of the canines, the right and left posterior teeth and the anterior teeth were fixed with wire ligature, and the maxillary arch was formed in three blocks. 16 × 22 beta-titanium T-loop arches were used to close the gaps in the maxillary and mandibular arches with incisor retraction.
Treatment resultsTreatment of both patients was completed in 28 months. Patient 1 was performed with a fixed and an Essix retainer at the end of treatment. Patient 2 was fitted with an Essix retainer for retention, as recommended by the specialist, depending on the ongoing periodontal treatment. For the missing tooth number 47, both patients were followed up for the planned implant and prosthetic restoration. Intraorally twin patients, bilateral molar and canine Class I relationship, correct overjet and overbite are illustrated in [Figures 3 and 4]. Cephalometric measurements pre and post-treatment are shown in [Table 1].

Export to PPT

Export to PPT
DISCUSSIONThe advantage of using monozygotic twins in such a comparative case report is that beyond measurement error, all differences in skeletal growth can be assumed to be non-genetic and therefore environmental.
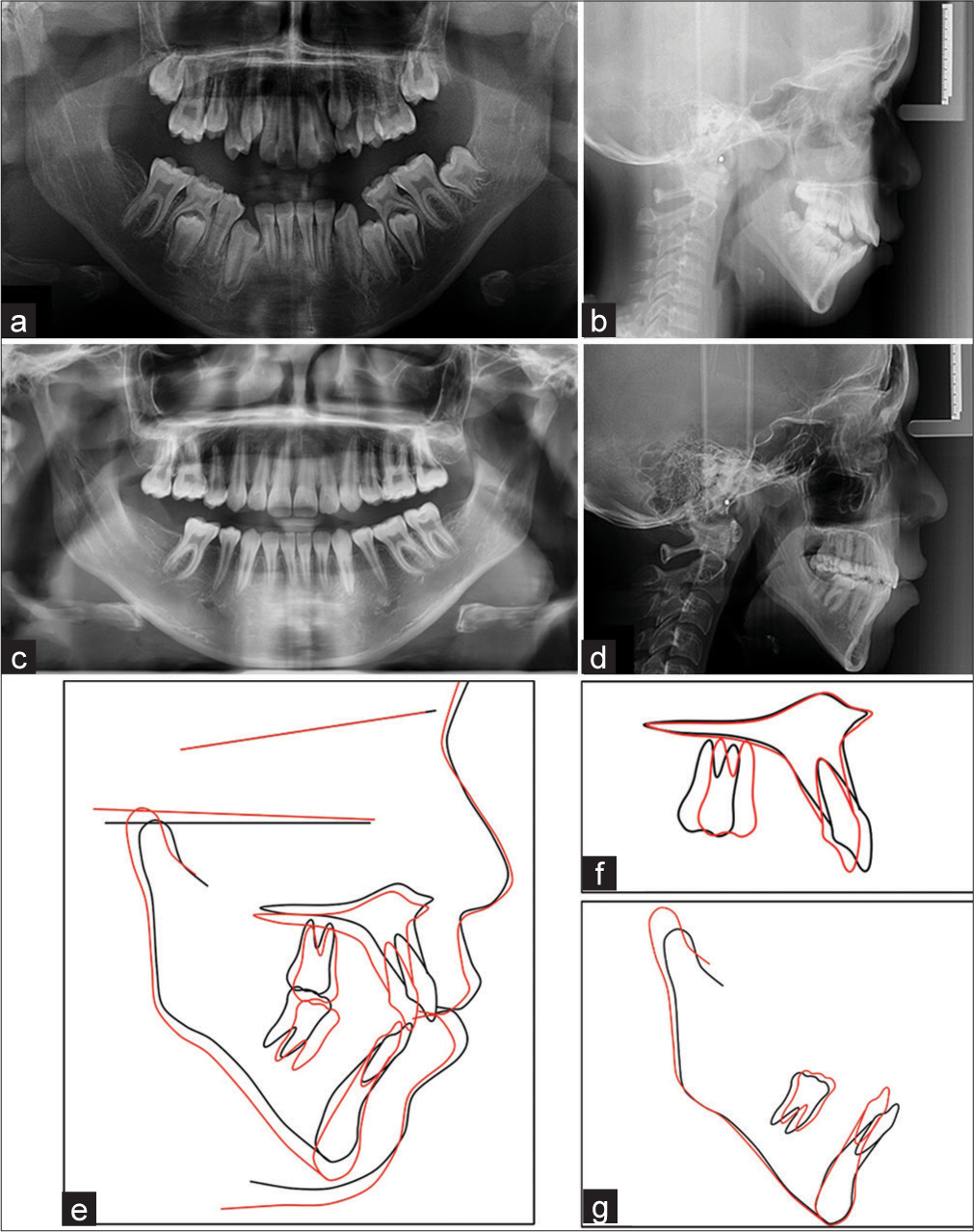
It has been reported in the literature that the combined treatment of twin block and high pull headgear allows the anterior development of the mandible while limiting the anterior and downward development of the maxillary complex.[4,7,11] In the study, an increase of 4.8° in the angle between sella-nasion- A point (SNA) (5.63 mm increase on Nasion vertical- point A (NV-A)) was observed in Patient 2, while an increase of 1.9° (1.9 mm increase on NV-A) was observed in Patient 1 [Table 1]. This is similar to the literature in which the combined twin block high pull headgear treatment prevents anterior growth of the maxilla.[7] In the superimpositions, downward growth of the maxilla and extrusion of the maxillary first molar was observed in Patient 2, while vertical growth of the maxilla and maxillary first molar was inhibited in Patient 1 using the occipital headgear.
While the literature has reported positive treatment effects of removable functional appliances on mandibular length increase,[12,13] effective condyle growth, and mandibular growth,[14] Koretsi et al.[1] reported that the skeletal effect of removable functional appliances is minimal and of insignificant clinical importance when considering the natural growth pattern of patients without removable functional appliances. While an increase in the angle between sellanasion- B point (SNB) angle of 3.19° (7.61 mm increase on Nasion vertical- point B (NV-B)) was observed in Patient 1, an increase in the SNB angle of 2.31° (5.63 mm increase on NVB) was observed in Patient 2 [Table 1]. In terms of functional treatment, some articles confirmed that more correction was achieved by dentoalveolar changes than by skeletal changes.[1,15]
In Patient 1, the forward movement of the mandibular molars with the twin-block appliance was significantly obvious on superimposition [Figure 5]. Considering the dentoalveolar findings of our study, it is suggested that the effects of the twin block high pull headgear combined treatment on the mandible are mainly dentoalveolar and supported by skeletal changes.
Export to PPT
Patient 1 showed a decrease of 1.22° in the angle determined by points A, N and B (angle between SNA and SNB) while Patient 2 showed an increase of 2.49° [Table 1]. This finding is due to the use of the combined twin block high pull headgear, which inhibited maxillary growth and promoted mandibular growth in Patient 1, whereas maxillary growth and development continued in Patient 2.
In Patient 1, a decrease in mandibular plane angle was observed [Table 1]. Although it has been reported that twin-block treatment can cause rotation in the mandibular planes, the result is related to the effect of the use of the high-pull occipital headgear, which prevents vertical eruption of the maxillary molars. In Patient 2, an increase in the mandibular and occlusal plane angle was observed. In the treatment of Class II malocclusions, it has been reported that the mandible rotates counterclockwise in pre-molar extractions,[1] while other studies have reported an increase in the angle between the Sella Nasion plane and the Go-Gn line-mandibular plane angle (SN-GoGn).[16] The mesial movement of the first molars during the closure of the extraction spaces may be related to the prevention of clockwise rotation of the mandible. In the study, mesialization of the maxillary and mandibular molars was observed in cephalometric superimposition [Figure 6], but continued extrusion of the maxillary molar may have increased the angle of the mandibular plane.
Export to PPT
In fact, in Patient 1, upper incisor retroclination and lower incisor proclination were observed. These results are the expected effects of the use of the twin-block occipital headgear.[7,15,17] Retrusion effect of pre-molar extraction orthodontic treatment on incisors has been reported.[18] In Patient 2, upper and lower incisor retroclination was observed. The interincisal angle was optimized at the end of the treatment [Table 1].
In Patient 1, the upper lip was retruded due to upper incisors retroclination, while the lower lip was protruded due to lower incisors proclination (upper lip 1.3 mm back, lower lip 1 mm forward according to E-line). In addition, the backward movement of the upper lip with respect to the E plane is explained by the forward movement of the mandible with the twin block. In Patient 1, the lower lip thickness was reduced, and the lower lip length increased due to reduced overjet and lower incisor protrusion. The increase in the length of the lower lip can be explained by the reduction of the overjet and the release of the lower lip from the locking of the upper incisors, similar to the literature.[19] It can also be supported by the change in perioral muscle tone and posture caused by the patient keeping the mouth closed during the use of the twin block appliance.
In Patient 2, who underwent pre-molar extraction, significant retrusion was observed in the upper lip, whereas no significant change was observed in the lower lip (upper lip 1.3 mm and lower lip 0.4 mm back according to E-line). The results are consistent with the results of lip retrusion in extraction treatment.[2,18,20] It has been reported in the literature that lip retraction in extraction treatments can support passive lip sealing and contribute to facial esthetics by enhancing the contour of the chin.[20] In the study, while the thickness of the lower and upper lips increased in Patient 2, the patient with incompetent lip closure at the beginning of the treatment was able to passively lip seal.
Due to the multifactorial etiology of Class II malocclusion and the varying recommended treatment protocols, there is currently no consensus among experts.[21] At the end of the treatment, both patients were satisfied with the esthetic results. Based on the study findings, pre-molar extraction treatments are effective in achieving lip closure and providing a good occlusion in Class II patients with, vertical direction growth, crowding, space problems, and proclination of the incisors. In addition, it is believed that patient compliance and co-operation are among the most important factors for successful results in functional treatments. Extraction treatments can also be a successful treatment option for patients in the growth and development phase who are not compliant with functional treatment.
CONCLUSIONDespite the different treatment modalities, both twins achieved a Class I canine-molar relationship and ideal overjet and overbite. Patients can close their lips with improved soft-tissue profiles. It is observed that the effects of early appliance treatment are primarily dentoalveolar and support skeletal changes. The criteria for the choice of one-phase or two-phase treatment depend entirely on the requirements of the patient. Environmental and psychosocial factors need to be carefully considered.
Comments (0)