Summary of results
The meta-analyses results determined that the pooled success rate for implants was 92% and for grafts, 95%, though both had significant heterogeneity. Implants in fibular grafts had a 2.91 times higher failure rate than those in natural bones, which was statistically significant. However, no significant difference was found when comparing free fibular grafts with other grafts. Additionally, radiated bone and smoking were identified as factors influencing implant failure, with radiated bone having a 2.29 times higher risk of failure and smokers having a 3.16 times higher risk compared to their respective counterparts.
Meta-analyses for patient-reported outcomes, radiographical assessments, and the effects of malignancies and HBO on implant success were not possible due to variations in methods and measures.
In the studies reviewed, various assessments were conducted to evaluate implant success, such as X-ray evaluations, bleeding on probing, and pocket depth measurements.
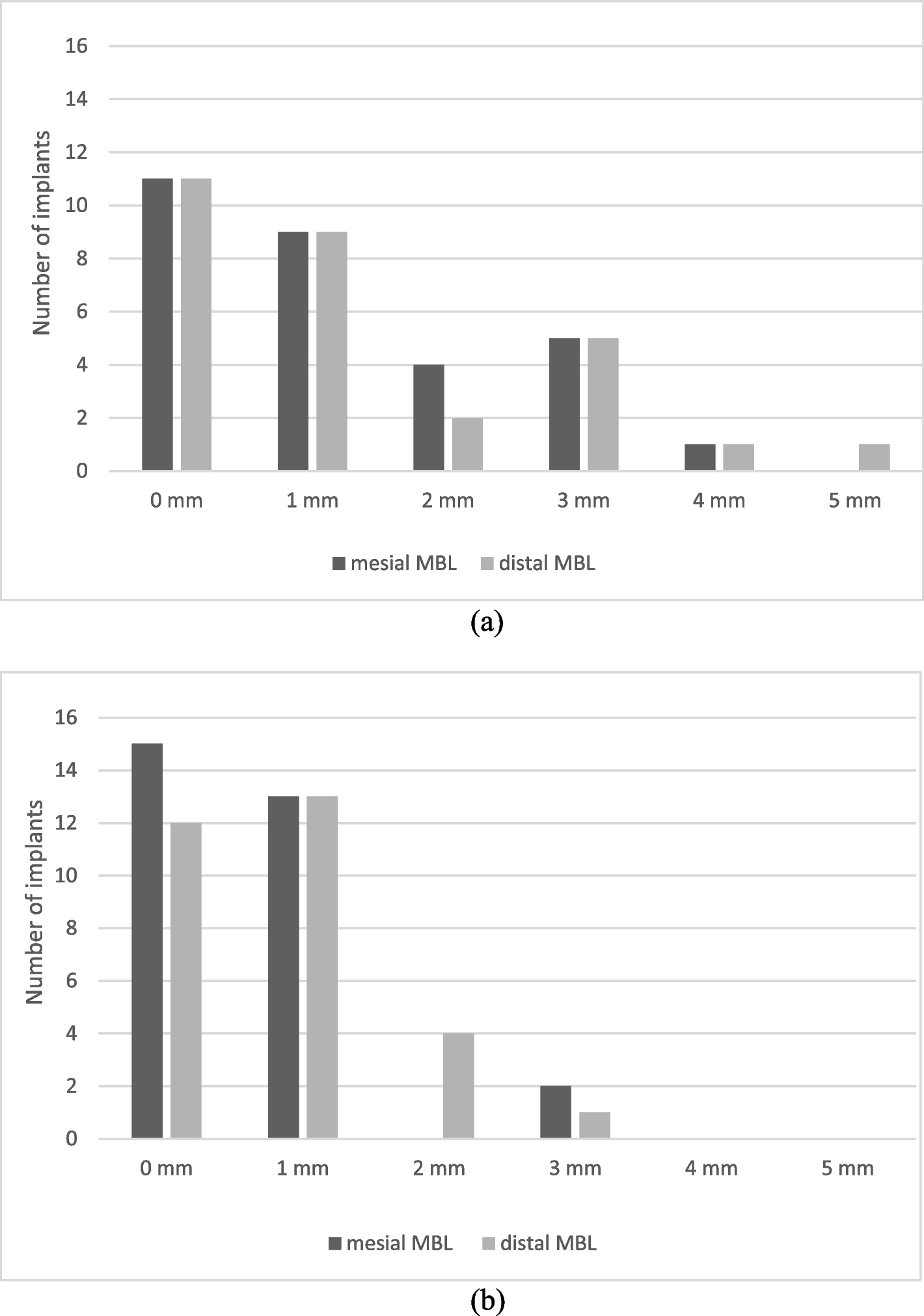
Attia et al.’s radiographic evaluation reported that 93 implants exhibited ≤ 1 mm of bone resorption, 11 had 1–2 mm, and 14 showed ≥ 3 mm. Their probing depth measurements revealed normal depths (1.0–4.0 mm) in 111 implants and 5.5 mm in 7 implants. Additionally, they found no sign of bleeding in 88 implants during the bleeding on probing assessment [17].
De Santis et al.’s X-ray evaluation indicated low bone resorption (1–2 mm below the head of the implant) after 1 year, although a specific percentage was not provided [23].
Gbara et al. observed that crestal bone resorption was less than 1 mm in 62 implants (53%), 1 to 2 mm in 35 implants (29.9%), and greater than 3 mm in 20 implants (17%). They reported no pathological probing depths in 93 of 121 implants, with depths ranging from 2 to 3 mm. Their sulcus bleeding index averaged 0.78, with 20 implants showing probing depths of 4 to 6 mm and an average sulcus bleeding index of 1.8. In 4 implants, probing depths exceeded 7 mm, with an average sulcus bleeding index of 3.5.
Pellegrino et al. reported bone resorption ranging from 0.5 to 8.1 mm (mean 2.2 ± 1 mm) at the 10-year follow-up, without providing a percentage. Their pocket depth measurements ranged from 2 to 9 mm, with a mean of 3.8 ± 2 mm [24].
These findings suggest that implant success in fibula free flaps is generally favorable, with minimal bone resorption, manageable probing depths, and limited bleeding on probing.
For patient-reported outcomes of functional rehabilitation after graft and implant placement, several studies have reported varying degrees of improvement in key areas such as dietary intake, mastication, speech, and esthetics. Ariga et al. observed improvements in dietary intake, mastication, and speech, along with high satisfaction regarding esthetics for the majority of their patients [16]. Similarly, Bodard et al. reported prosthesis satisfaction in most cases, with esthetic and dietary improvements observed more frequently in patients with fixed prostheses compared to removable dentures [19]. Furthermore, Lodders et al. found that functional dental rehabilitation was achieved for a majority of their patients, though patients with irradiated FFFs experienced slightly lower success rates [12].
Another study by Lodders et al. evaluated patient-reported scales for quality of life and functional rehabilitation, finding better emotional functioning, cognitive functioning, speech, mastication, speech, and reduced diarrhea for patients with implant dental rehabilitation (IDR) compared to those without [26]. Menapace et al. reported that patients in the primary implantation group experienced a shorter timeframe for nasogastric tube removal and had better oral competence and speech outcomes than those in the secondary implantation group [27]. However, these differences were not statistically significant and could be attributed to multiple factors. Overall, these studies indicate that functional rehabilitation outcomes can vary but generally show improvement in key areas such as dietary intake, mastication, speech, and esthetics following graft and implant placement.
Factors influencing the success rate
The impact of smoking on implant success warrants further discussion, particularly when comparing active smokers and ex-smokers. Burgess et al. found that both ex-smokers and active smokers had lower survival rates (78% and 72%, respectively) compared to nonsmokers (94%) [20]. This suggests that even ex-smokers may be at a significantly higher risk of implant failure compared to nonsmokers which is similar to the results of graft success rate in the Chen et al. study [31]. Consequently, it is important to consider patients’ smoking history before graft and implant procedures and to provide additional interventions aimed at increasing implant success for these higher-risk individuals.
Furthermore, differences in the effects of radiation before and after implant placement should be considered. Ch'ng et al. demonstrated that preoperative radiation resulted in a lower survival rate (92%) compared to postoperative radiation (96.8%) [21]. Studies by Khadembashi et al. and Kniha et al. also found that pre-implant radiation significantly reduced implant success rates compared to those irradiated after implant placement [14, 30]. This is consistent with findings from other studies on implantation and radiotherapy in natural bone [32]. Some authors, such as Pompa et al. and Laverty et al., recommend implant insertion before radiation therapy to allow initial osseointegration to occur before irradiation, thus reducing the risk of late complications [33, 34]. Moreover, Lodders et al.’s study found that all the implants in actively smoking patients who underwent radiation failed, indicating that a combination of these risk factors may further exacerbate implant failure rates and emphasizing the need for careful patient selection and management in these cases [12].
Another aspect to consider is the difference in outcomes between primary and secondary reconstruction. Primary reconstruction refers to grafting performed immediately after the ablation of pathological bone, while secondary reconstruction occurs at a later time and in a separate surgery following the initial ablation. In the Chiapasco et al. study, no significant differences were found between these two methods in terms of implant success rates. However, it is important to note that the number of patients with secondary reconstruction in this study was relatively low (17), which may limit the conclusiveness of the findings [22].
The effects of various factors such as age, sex, alcohol consumption, and diabetes on implant success rates should also be considered. Khadembashi et al. found that increasing age and male gender increased the risk of implant failure, while Ch'ng et al. discovered that the success rate of implants in patients over 65 years of age was lower, although not statistically significant [14, 21]. Studies on implant outcomes in native bone have also reported mixed findings regarding the impact of age on implant failure [35]. Regarding alcohol consumption, Lodder et al. found no statistically significant differences between alcohol consumption and implant or graft failure. As for diabetes, Ch'ng et al. observed that in patients with controlled diabetes, there were no significant differences between the implant success rates of diabetic (96%) and nondiabetic patients (97%) [21].
HBO has been proposed as a potential method for improving implant success rates, particularly in patients with compromised healing conditions [36]. HBO involves the administration of 100% oxygen at pressures greater than atmospheric pressure, typically between 2 and 2.5 atmospheres absolute. This treatment increases the amount of dissolved oxygen in the bloodstream, which can enhance tissue oxygenation, reduce edema, and promote angiogenesis [37]. These physiological effects may contribute to improved healing and, consequently, increased implant success rates.
Several studies have reported positive outcomes when using HBO as an adjunctive therapy in dental implant procedures, particularly in patients who have undergone radiotherapy or have other risk factors that impair healing. HBO has been shown to improve bone quality, soft tissue healing, and implant osseointegration in these patients, leading to better overall success rates [38, 39]. Furthermore, HBO may reduce the risk of osteoradionecrosis in patients who have undergone radiotherapy. In our review study, two studies by Lodders et al. and Parbo et al. utilized HBO in all of their patients who had undergone radiotherapy [12, 13]. Despite the use of HBO therapy, these studies still found significant differences in the success rates between radiated and non-radiated implants. This observation suggests that HBO might not be as essential in implant success rates as some other studies claim. However, since all the radiated patients in these studies underwent HBO therapy, it is impossible to fully assess the effects of this treatment on radiated free fibula graft patients.
Nonetheless, HBO therapy could still be suggested as a possible intervention for patients with risk factors, particularly those who have undergone radiotherapy. It is important to note that the results from these studies should not be taken as definitive evidence against the benefits of HBO therapy but rather an indication that further research is needed.
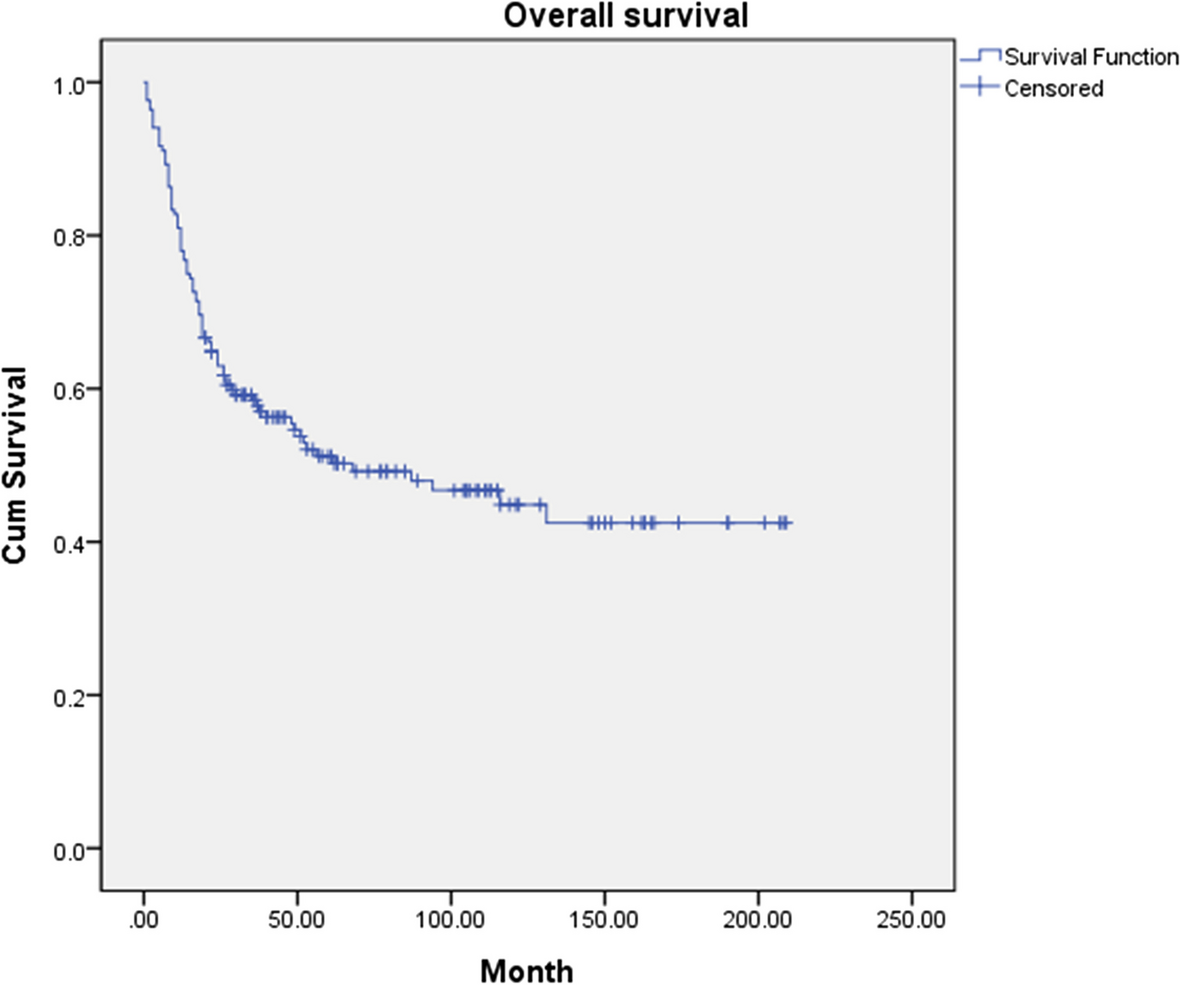
In our review and meta-analysis, all the included studies had a follow-up period of at least two years after loading the implants. A notable observation across these studies was the considerable drop in implant success rates over time. For example, in the study by Khadembaschi et al., the success rate of FFF implants was 93% at 1-year, 90% at 2-year, 86% at 5-year, 83% at 7-year, and 69% at 9-year follow-up [14]. Similarly, in the Pellegrino et al. study, the success rate for FFF implants was 97.2% at 12-month follow-up, 86.5% at 60 months, and 79.3% at 120 months [28]. This decline in success rates highlights the importance of long-term follow-up when evaluating the effectiveness of dental implant procedures in free fibula graft patients.
The drop in success rates could be attributed to various factors such as aging, changes in health status, or the long-term effects of radiotherapy, which might impact the osseointegration and stability of the implants. Given these findings, it is crucial for future studies to consider the significance of long-term follow-up when assessing the success of dental implants in free fibula graft patients. Consistent monitoring and reporting of implant success rates at different stages of the follow-up period can help identify potential challenges and develop appropriate interventions to address them.
And finally, in the prospective study by Zweifel et al., the authors investigated the precision of simultaneous guided dental implantation in microvascular fibular flap reconstructions with and without additional guiding splints [29]. The study involved two groups: a trial group using additional tooth-borne and plate-borne splints for implant position and angulation verification and a control group following the standard preplanning protocol without additional splints. With a total of 8 patients, the results revealed that the average positioning error at the bone level was lower in the trial group (0.9 mm) than in the control group (1.3 mm). Similarly, the angulation errors in both buccolingual and axial planes were generally lower in the trial group. The use of intraoral and/or extraoral verification splints proved effective, with minimal additional operating room time required. This study underscores the potential benefits of employing additional guiding splints in dental implantation procedures for microvascular fibular flap reconstructions.
Comparison with similar studies
There are other systematic reviews and meta-analysis to evaluate the success rate of implants in free fibular grafts. For example, Gangwani et al. assessed the success rate of implants in 10 retrospective studies [40]. Gangwani et al.’s study reported a 94% success rate (CI = 0.91 to 0.96) with an annual implant failure rate of 0.02 (CI = 0.01 to 0.03). Our study’s pooled success rate was 92% (CI = 0.89–0.95) for implant success and 95% (CI = 0.92–0.99) for graft success. We also investigated factors influencing implant failure, such as radiotherapy and smoking, which Gangwani’s study did not address.
Our study, which included 18 studies with 16 of them being part of the meta-analysis, provides a more comprehensive analysis compared to the systematic review and meta-analysis by Gangwani et al., which consisted of 10 studies. Our analysis evaluated not only the success rate of osseointegrated dental implants placed in fibula free flaps but also the factors affecting the success rate. In contrast, Gangwani et al. focused solely on the success rate of dental implants in fibula free flaps using the Albrektsson and colleagues’ criteria.
Furthermore, study done by Ardisson et al. focused on the implant success rate after mandible reconstruction with vascularized fibula bone grafts [41]. Their systematic review included 13 cohort studies which reported a success rate of approximately 98% for fibular reconstructions and 92.6% for implants placed in vascularized fibular grafts after a mean follow-up period of 40 months. They also observed that implant survival in irradiated patients was lower compared to nonirradiated patients, but alcohol and tobacco use showed no significant association with implant failure.
Our success rate results are closely aligned with those from the Ardisson et al. study, which reported a 95% graft success rate and a 92% implant success rate. Both studies found that radiotherapy negatively impacted the implant success rate. However, our study identified a significant difference in implant failure due to tobacco use, whereas Ardisson et al.’s study did not.
It is important to emphasize that Ardisson et al.’s study did not conduct a meta-analysis to evaluate the effects of tobacco and radiation on implant failure. Instead, they relied on a review of individual studies. In contrast, our study utilized a meta-analysis approach to assess these factors, providing a more rigorous and reliable assessment. Furthermore, our study included a larger number of studies (18), which adds to the robustness and reliability of our findings. Consequently, our study offers a more dependable evaluation of factors influencing implant success, including tobacco use and radiation exposure.
Limitations and suggestions for further researchLimitations
High heterogeneity was observed in the meta-analyses for both implant and graft success rates, which could affect the reliability of the pooled success rates.
The majority of the studies were retrospective, potentially introducing biases such as selection and recall biases.
Due to variations in intervention methods and outcome measures, some meta-analyses (e.g., for patient-reported outcomes and radiographical assessments) were not possible, limiting the comprehensiveness of the results.
Suggestions for further research
Future studies should focus on conducting prospective, controlled trials to reduce biases and improve the quality of evidence in this area.
Standardization of outcome measures and intervention methods would facilitate more meaningful comparisons and enable more comprehensive meta-analyses.
Researchers should investigate the long-term success rates of implants and grafts in different patient populations, considering factors such as age, smoking history, and radiation therapy status.
Further research should explore the relationship between different implant and graft types and functional rehabilitation outcomes, such as dietary intake, mastication, speech, and esthetics, to inform clinicians on the best course of action for each patient.
Studies should examine the effectiveness of interventions aimed at increasing implant success rates in higher-risk individuals, such as smokers and those with a history of radiation therapy.

留言 (0)