BPs are commonly used for the prevention and treatment of skeletal-related events that are linked to both metastatic cancer and osteoporosis. It is undeniable that BPs can enhance the quality of life, prevent bone loss during chemotherapy, prevent hypercalcemia associated with malignancy, and aid in the prevention of cancer. Despite their benefits, BPs pose a risk of BRONJ for patients who receive them. Therefore, it became necessary to develop a drug that can provide the same therapeutic benefits as BPs without the risk of side effects such as ONJ. This has led to the discovery of DMB, which is a human monoclonal antibody that can impede osteoclast function [4]. In June 2010, the US Food and Drug Administration (FDA) approved the use of DMB, marketed under the trade name Prolia® (Amgen in Thousand Oaks, California, USA). This particular formulation is intended for use in postmenopausal women at risk of osteoporosis, with the standard regimen being a subcutaneous injection of 60 mg DMB every six months. In November 2010, the FDA approved DMB in the form of Xgeva® (Amgen, Thousand Oaks, California, USA), for the prevention of skeletal-related events in patients with bone metastasis from solid tumors [4].
With the increasing number of patients taking DMB, clinicians have started observing denosumab-associated osteonecrosis of the jaws (DONJ), which shows a similar clinical presentation to BRONJ. There are several hypotheses aimed at explaining the unique localization of ONJ when related to systemic anti-resorptive medications. The literature suggests similar mechanisms for the pathophysiology of DRONJ and BRONJ [9]. These theories include altered bone remodeling, inhibition of angiogenesis, repetitive and persistent microtrauma, impaired tissue protection and soft tissue anatomy, toxicity of BPs, and bacterial infection [10, 11].
However, DMB and BPs have different mechanisms of action, and it has been reported that the pharmacokinetics of DMB are more favorable in managing ONJ than those of BPs. The main factor contributing to this difference is that BPs, once absorbed, have a half-life of approximately 10 years, whereas the interaction between DMB and bone is more reversible [12]. DMB is a fully human monoclonal immunoglobulin 2G (Ig2G) antibody that works by inhibiting a critical step in the differentiation of osteoclasts, which leads to a decrease in bone metabolism. Specifically, DMB blocks the binding of RANKL to its receptor, receptor activator of nuclear factor kappa (RANK), which is located in the cell membranes of both osteoclasts and osteoclast precursor cells. Pharmacologically, DMB acts by mimicking the function of the endogenous molecule osteoprotegerin (OPG). RANK, RANKL, and OPG are all members of the tumor necrosis factor superfamily of proteins with OPG having a particularly strong antiresorptive effect. OPG has a significant impact on the regulation and balance of osteogenesis by inhibiting the formation, attachment, and activation of osteoclasts, as well as increasing osteoclast apoptosis [13]. Working together, RANKL and OPG maintain a healthy balance of bone resorption. However, if the RANKL/OPG ratio increases, it can tip the balance in favor of bone resorption, leading to skeletal diseases [14].
Unlike bisphosphonates, DMB circulates in the bloodstream and does not accumulate in bone tissue. This is due to differences in their pharmacological mechanisms. While the elimination half-life of DMB is much shorter (26 days) than that of bisphosphonates (10 years), its pharmacodynamic half-life, which refers to the duration of its antiresorptive effect, is longer than its elimination half-life [15]. A study by Bone et al. found that it took 9 months for the antiresorptive effects of a 60-mg dose of DMB for osteoporosis to fully reverse. Based on this, it can be assumed that the antiresorptive effects of a 120-mg dose of DMB would last for at least 9 months [16]. However, for most oncology patients, DMB is a life-prolonging drug that cannot be discontinued for such a long period.
Despite the potential of DMB to cause osteonecrosis due to its mechanism of action, the summary of product characteristics for Xgeva® (DMB 120 mg) does not indicate that MRONJ occurrence is a contraindication for reintroducing the drug [17]. Normally, DMB is administered in two dosage schemes: 60 mg subcutaneously every 6 months for the treatment of osteoporosis or 120 mg subcutaneously monthly for the prevention of skeletal-related events in cancer patients. In this study, all four cancer patients received DMB 120mg (Xgeva®) every 4 to 6 weeks.
The prevalence of ONJ in cancer patients is estimated to be similar for both BP-related cases (1.1 to 1.4%) and DMB-related cases (0.8 to 2%). The prevalence may increase to 3% in patients receiving adjunctive therapy with anti-angiogenic agents, especially in renal cell carcinoma [8]. According to the literature, the incidence of MRONJ in cancer patients treated with DMB 120 mg ranges from 0.7 to 11.4% [17].
In this study, we observed four cases of ONJ among 74 patients who received DMB therapy for metastatic cancer. Among the four patients who developed ONJ, three had prostate cancer, while the remaining patient had a history of breast cancer. The patients with prostate cancer were being treated with docetaxel and enzalutamide, whereas the patient with breast cancer was receiving trastuzumab. Furthermore, three out of the four cancer patients were also taking corticosteroids.
Studies have reported that ONJ induced by BP usually occurs after approximately 39.3 months and 35 infusions in oncology patients. However, it is interesting to note that all reported cases of ONJ related to DMB occurred early in the course of DMB therapy, regardless of the number of prior administrations [18]. In these reported cases, the average number of DMB injections was 8 and ONJ occurred within 1 year of starting the therapy (Table 1).
The relationship between anti-angiogenic medications and osteonecrosis of the mandible has been well established, and this is believed to be the underlying cause in cancer patients. The risk of ONJ may be increased when anti-angiogenic agents and steroids are used concomitantly with anti-resorptive agents, which is becoming more common in clinical practice [19].
Trastuzumab, a monoclonal antibody that inhibits epidermal growth factor, is an anti-angiogenic agent that is commonly used in the treatment of breast cancer. Previous studies have identified it as an independent risk factor for the development of ONJ. In some cases, ONJ has been reported to occur during concurrent treatment with bisphosphonates and trastuzumab [20]. Additionally, there have been case reports in the recent literature of ONJ developing solely due to trastuzumab treatment [21]. However, an association of trastuzumab with the occurrence of ONJ has not been clearly stated in these reports.
The anti-neoplastic agent TAX is frequently used in the treatment of prostate cancer. However, the present findings suggest that leukopenia induced by TAX is more relevant than TAX use itself in the development of ONJ [22]. The anti-angiogenic properties of both DMB and TAX may have an additive or synergistic effect on impairing jaw vascularization, leading to a higher susceptibility to bone necrosis.
While the exact cause of osteonecrosis in patients receiving a combination of DMB and anti-cancer drugs is not clear, it is believed that the incidence may be higher due to the presence of anti-angiogenic agents and steroids, which are known risk factors for osteonecrosis. Further research is necessary to better understand the underlying mechanisms and potential preventive measures.
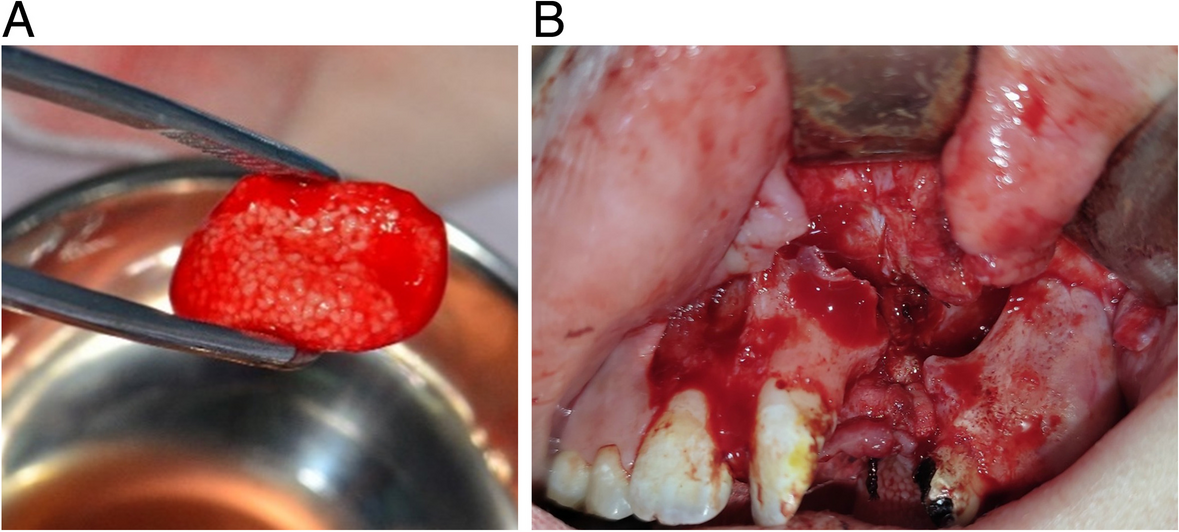
Actinomycosis was diagnosed in three out of four patients in this case report through pathological examination. The presumed cause of the actinomycete infection at the site of osteonecrosis is the immunosuppressive effect of anticancer drugs and steroids. By blocking RANKL activity, DMB can cause a decrease in macrophage and monocyte function and survival, which can ultimately impact the immune system and result in immunosuppression [23]. And this immunosuppressive effect would have resulted in an environment prone to infection with actinomycetes.
DRONJ is generally triggered by surgical manipulation of the affected area, such as dental extractions or implant placements. In addition to surgical manipulation, other factors such as trauma from ill-fitting removable partial dentures or full dentures, and impaction of debris under pontics, have also been reported as predisposing factors for DRONJ [24]. In this report, the main cause of ONJ was identified as surgical tooth extraction. These patients had undergone dental extractions within 2 months of their most recent DMB injection, which resulted in the induction of osteonecrosis. The recently published dental guidelines recommend that patients who are receiving a high dose of DMB (120mg Xgeva®) should receive any necessary surgical procedures at least 3 weeks after their last administration of the drug [25]. However, ONJ was still induced even though tooth extraction was performed 3 weeks after the last DMB administration. Furthermore, Hasegawa et al. have reported that a 1-month washout period before tooth extraction in patients with cancer who were receiving high-dose DMB did not reduce the incidence of MRONJ [26]. Therefore, further research is needed as there is no established guideline for minimizing the occurrence of MRONJ before dental surgical intervention in cancer patients treated with high-dose DMB. Additionally, preventive dental treatment is required before administration of DMB, as it has been found that underlying oral diseases such as periodontitis and peri-implantitis can induce ONJ [27].
In case 3, the patient developed DRONJ without surgical intervention. It is assumed that inflammation in the residual root caused the ONJ. Pre-existing periodontal disease or periapical pathology has been cited as a risk factor of MRONJ. Pre-existing inflammatory dental disease has been found to be a risk factor for MRONJ in 50% of cancer patients with the condition [27]. Therefore, it is recommended to consider periodontal disease treatment or tooth extraction prior to the administration of anticancer drugs in cancer patients to prevent MRONJ.
In this study, patients with ONJ were treated with sequestrectomy and antibiotic therapy using Augmentin. Sequestrectomy is a surgical procedure that involves removing a section of the necrotic bone that has become separated from the surrounding healthy bone. Minimally invasive surgical techniques are considered the most effective treatment for early stages (I and II) of MRONJ [28]. Among minimally invasive surgical options, debridement and sequestrectomy are commonly used. Debridement involves surgically removing dead bone tissue until healthy, bleeding bone is exposed and is typically performed when some healthy bone is still present.
Currently, there is limited understanding of the pathogenic mechanism of jawbone necrosis related to DMB treatment, and there is a lack of conclusive evidence on the effectiveness of drug suspension as a preventive measure, as well as the appropriate timing for this approach [27]. Recently, there has been a suggestion that performing oral surgery during a protective period of 5 to 7 months between the last and next dose of DMB may be a reasonable approach pharmacokinetically [29]. Regardless of the stage of the disease, cancer patients generally require more extensive surgical procedures due to the more severe progression of the disease compared to osteoporotic patients [30]. For this reason, in the case presented, the bone involvement (stage 2 ONJ) provided the indication for the debridement surgery of the necrotic bone, following the treatment guidelines based on the MRONJ staging system [27]. However, there is still a lack of conclusive evidence regarding the optimal suspension period for high-dose DMB and the appropriate timing of oral surgery in cancer patients.
For the first patient, who presented with stage 0-1 MRONJ, antibacterial oral rinse therapy was administered. However, after 4 months of treatment, the MRONJ did not improve and progressed to stage 2, indicating the necessity of surgical treatment. For the second patient, who presented with stage 2 MRONJ and did not show improvement despite over three months of antibiotic therapy, discontinuation of DMB was advised, and immediate surgical intervention was deemed necessary. As a result, surgical debridement was performed on the patient within a month of discontinuing DMB. The third patient presented with a mandibular sequestrum and had stopped using DMB 4 months prior to the visit. Consequently, a surgical plan was established on the first day of the visit, and a sequestrectomy was performed within a month.
The surgical site healed in less than 4 months for most patients. However, one patient developed postoperative ONJ at another site after 5 months and required an additional operation. It took a total of 10 months for this patient’s ONJ to fully heal.

留言 (0)