
Remember me




The main aim of this study is to test the feasibility of implementing individual music therapy (IMT) and group music therapy (GMT) as an intervention for service users (SUs) experiencing symptoms of depression and/or anxiety and engaged with CSMTSs. In order to approach the primary aim, our objectives are (I) to measure qualitative data on SU satisfaction with the MT program, (II) to measure retention in treatment and (III) to collect their feedback over the course of the treatment. The secondary aims of this project are to examine the feasibility of applying a pre-test, posttest, and in-session assessment battery as well as to measure the effects of MT (GMT and IMT) on mental health and the neural processing associated with it. We aim to explore the effects of MT in addition to standard treatment (ST) versus standard treatment alone. Further secondary aims concern the exploration of features of the therapeutic relationship and the role of music technology in the delivery, recording, and analysis of music therapy sessions. In order to approach the secondary aims, our objectives are: (I) To measure the effects of MT in addition to ST on the following treatment outcomes in comparison to ST alone: (a) substance use, (b) physical, mental wellbeing and quality of life, (c) retention in treatment, (d) engagement with treatment, (e) completion rate, (f) emotional processing, (g) psychological symptomatology. (II) To measure reduction in craving intensity after single MT sessions. (III) To compare the effect of MT in addition to ST versus ST alone on craving, inhibitory control, depression, anxiety and the respective associated neural signatures. (IV) To explore the perceived therapeutic alliance in IMT sessions. (V) To explore the neural dynamics of emotional processing during IMT sessions. (VI) To explore SU experiences of using music technology in an MT intervention. (VII) To explore how music technology can be utilized in the subsequent analysis of audio data of musical interaction recorded during MT sessions.
We expect that an MT intervention, carried out alongside the ST, will (a) be feasible and acceptable for individuals receiving community-based substance misuse treatment; (b) lead to a decrease in the symptoms of anxiety, depression and craving that correlates with changes in the underlying neural processes; (c) improve treatment outcomes for SU in CSMTSs; (d) improve inhibitory control that correlates with a change in the underlying neural process and, potentially, with changes in the craving intensity.
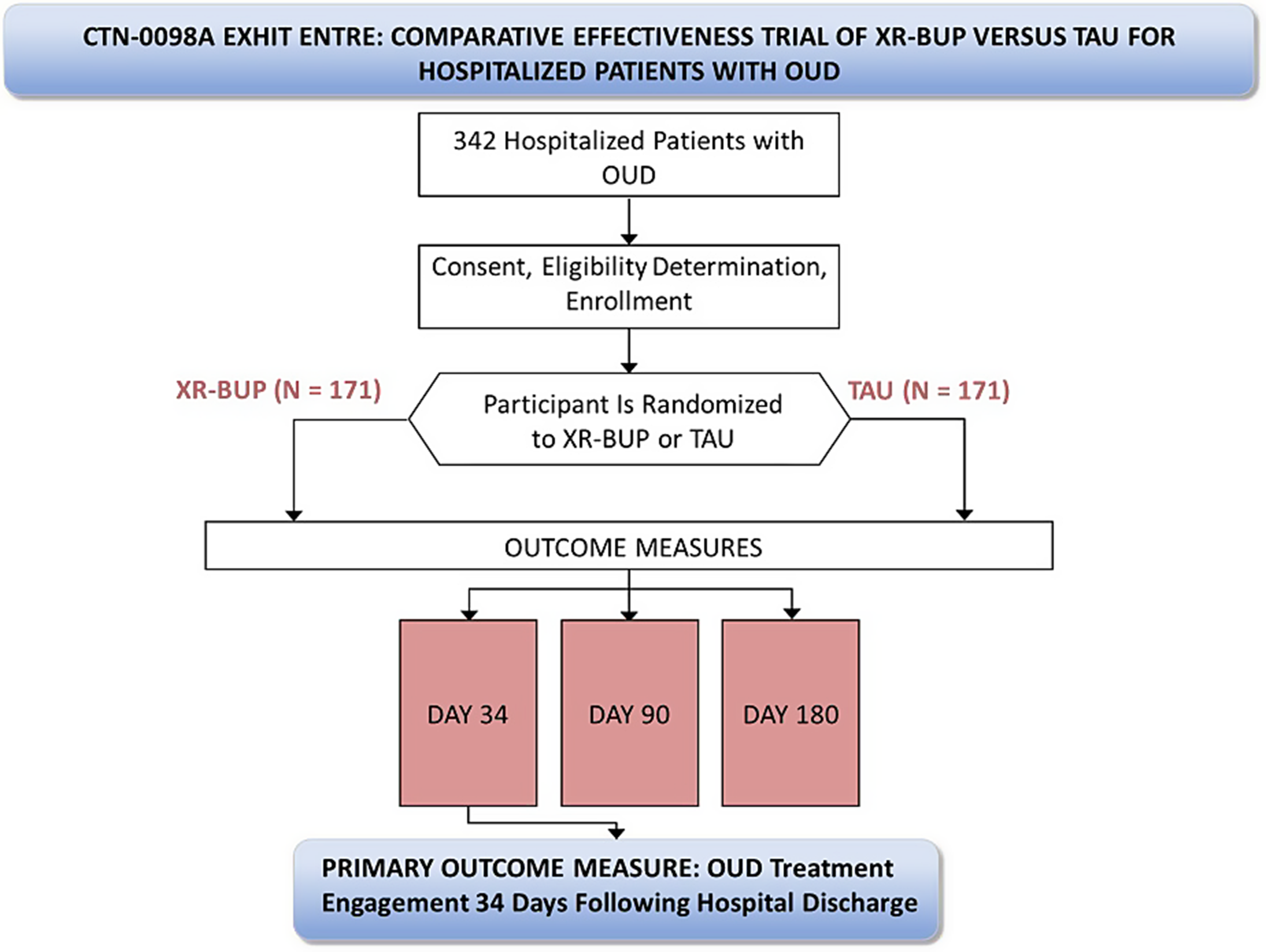
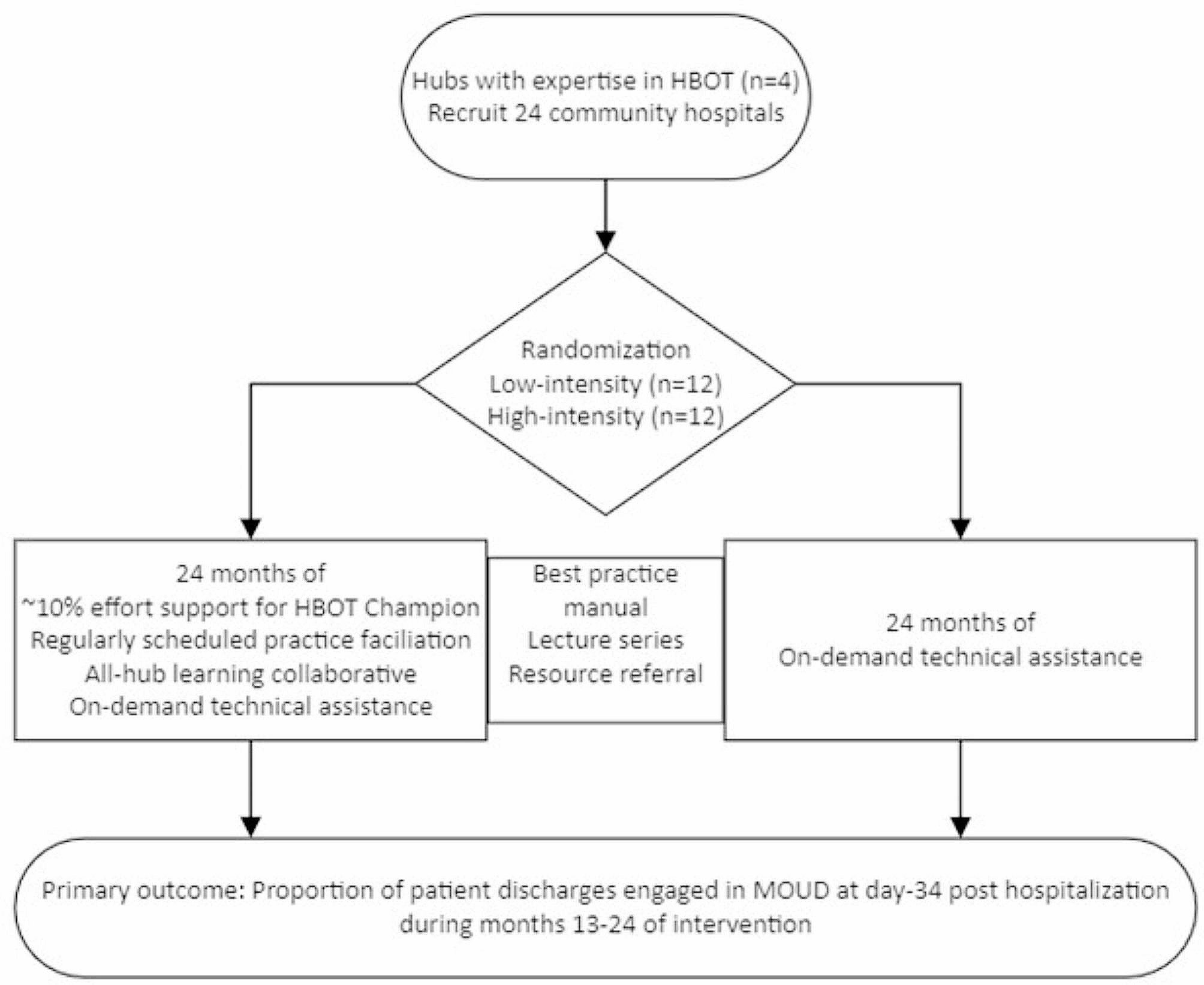
Study designWestminster Drug Project (WDP) is a substance misuse service provider delivering services within the UK. WDP’s Innovation & Research Unit (IRU) and the Cambridge Institute for Music Therapy Research (CIMTR), Anglia Ruskin University, have designed a mixed-methods feasibility study to address these aims and objectives. The study is designed as a three-armed study (Fig. 1) with group 1 receiving 6 weekly sessions of GMT alongside ST (see section “interventions”), group 2 receiving 6 weekly sessions of IMT alongside ST, and group 3 serving as a control group (CG), receiving 6 weeks of ST only. All participants will take part in pretest–posttest assessment (i.e., baseline and post-intervention measures) including subjective (i.e., multi-item questionnaires), behavioral (i.e., Go/No-Go task) and EEG measurements to assess several mental-health-related clinical endpoints. SUs allocated to group 2 will receive IMT while simultaneously EEG-hyperscanning is being recorded during the 2nd and 5th therapy sessions. After these two sessions, participants will undergo a semi-structured interview to select moments of therapeutic interest and complete a multi-item questionnaire measuring the quality of therapeutic relationship. Each participant allocated to GMT and IMT will also complete a single-item questionnaire to assess the intensity level of craving. Feedback from participants will be collected throughout the study and, where possible, requests will be implemented into the subsequent session. Engagement and treatment status of participants will be assessed 6 months post-intervention. After the intervention two different focus groups will be conducted: one involving MT participants and another involving a Staff Group (SG) of 4–8 WDP staff members who work with the service users involved. The SG focus group will explore the feasibility of MT from several perspectives, including those involved in the set-up of the MT sessions. Whilst the duration of the entire study is outlined to be a period of 3 months, participants will be committed for 8 weeks.
Fig. 1
Consort flowchart representing study design and procedure
Patient and public involvementThe research team attended a SU consultation, organized by WDP, to present the project design and gather feedback from a SU perspective. A total of 7 SUs attended this consultation. The aim of this consultation was to get initial views of the design, participant time commitment, general interest in music therapy and thoughts on the EEG element. The research team received positive feedback from the SU's in attendance. The consultation also provided some input into the music therapy sessions, with suggestions on which instruments should be available. Further to this consultation, the research team will hold drop-in session within the WDP service during the recruitment window. This drop-in session will seek to aid recruitment and provide further information about the project and what participation will involve. Interested service users will also be able to ask the research team questions regarding the study and offer feedback.
ParticipantsFifteen SUs and, from a minimum of 4 to a maximum of 8 staff members, will be recruited from WDP. In total, we will recruit between 19 and 23 participants. The inclusion criteria for the recruitment of SUs include: (I) being a SU in structured treatment for drug and/or alcohol misuse, (II) being 18 years old or older, (III) reporting symptoms of depression and/or anxiety, (IV) being deemed suitable to take part in a group/individual setting by their key workers (who are Recovery Practitioners responsible for coordinating and delivering psychosocial interventions for SUs), (V) being right-handed.
The exclusion criteria for the recruitment of SUs include: (I) having a legal requirement to attend as part of a Drug Rehabilitation Requirement or Alcohol Treatment Requirement as this may impact engagement results, (II) being unable to provide informed consent due to a lack of mental capacity, (III) little/no understanding of spoken English as all sessions will be carried out in English and instructions for subjective measures used in this project are in English, (IV) being left- and mixed-handed: an outcome measure utilized (i.e., the EEG frontal alpha asymmetry) is modulated by handedness direction (i.e., left-handed, right-handed) providing empirical justification for the practice of excluding left-handers and mixed-handers when exploring relationships between this neural marker and other variables [34], (V) not being registered with a general practitioner (GP)/unable to provide GP details: we will require GP details to notify them in case of any incidental EEG findings. Furthermore, participants who disclose in the consent form that they had experienced a Stroke, Traumatic Brain Injury, or Epilepsy will be contacted by the research team to discuss if they can wear an EEG cap and participate in the measurements. Our inclusion and exclusion criteria are broadly based on the eligibility criteria for SUs to attend most groups in the service. We expect participants to either be abstinent or present with low to moderate substance use. Participants would also likely be housed and have access to public funds. While this presents a sample with diverse substance use patterns and individual circumstances, this is more representative of the cohort that would use this type of intervention. The diversity in participants may aid determining feasibility and acceptability of the intervention and provide value in planning further more focused studies. Regarding SG, only members of WDP staff will be included in this group.
RecruitmentOpportunistic sampling will be used, with eligible SUs being identified and then provided an information sheet detailing the project. The service will also feature a poster advertising the project and asking interested SUs to contact WDP staff for more information. SUs volunteering to participate will be asked to complete an informed consent form. Once participants are recruited the researchers will randomly assign participants to one of the three groups (GMT, IMT or CG).
Recruitment will be carried out by advertising the project in the community and by WDP staff identifying eligible SUs through WDP's case management system. SUs can choose to opt out from being approached about research, so only those who have indicated that they are happy to be approached about research will be contacted. For those that have not been identified through the case management system but approached by their key worker, the key worker or service administrator will ascertain eligibility through the case management system and in keywork sessions. SUs identified as eligible will be provided with the information sheets and consent forms and asked to return these. Consent will be taken with a member of the research team or WDP staff present. This is to ensure that someone is there to help with questions and understanding. The long version of the participant information sheet is a comprehensive document including information on the project, ethical information, benefits, and potential risks of participating in the study. The short version of the participant information sheet includes a brief overview of the project and what participating in the study entails.
The staff cohort will be recruited by directly approaching staff members who were involved in the project or may be involved in future forms of the program. This will be done by emailing them directly or attending staff meetings and asking for volunteers to participate. Staff members will also be invited to attend the drop-in session. SUs who participate will be rewarded Capital Card® points. Points will be awarded for each session completed, including the focus group and interview. WDP Capital Card® is a reward card scheme to help SUs with their recovery journey ([35]; https://www.wdp.org.uk/the-capital-card). Where the project has issues recruiting the full number of 15 SU participants, we will extend the recruitment window to 2–3 months and we will re-run the drop-in session to attract more SUs. We will also contact WDP key workers to promote the study. Recruitment for GMT will continue until 5 participants are recruited and allocated to this group. If the 5 participants are not recruited within 2 months, the GMT sessions will start once at least 3 participants have been allocated. The GMT will continue while 3 participants remain in the study. The start of the IMT sessions will be staggered: SUs allocated to the IMT group will start their MT sessions within 1–2 weeks of being allocated to this group. If a participant in the IMT group drops out within the first 2 weeks, we will re-recruit and the new participant will start from week 1. We will only re-recruit twice before continuing with the remaining IMT participants. If after 3 months, the project does not have enough participants to go ahead, the research team will discuss additional recruitment strategies, widening the inclusion/exclusion criteria or a possible change in study location. The research team will take any feedback from SUs or staff around recruitment and incorporate where necessary. Where a participant decides to withdraw from the study, they will be provided an exit survey and withdrawal confirmation form. This form gives the participant the option to decide if the data collected up to their withdrawal will be kept and used in the final analysis or destroyed and not used in the final analysis. If they choose not to complete this survey or ask that all their data collected up to their withdrawal is deleted, the exit survey will be destroyed.
ProcedureOne week prior to the start of the interventions, the baseline measurement battery (secondary outcomes) will take place. Handedness will be assessed with the Edinburgh Handedness Inventory and a pre-EEG screening questionnaire will be administered.
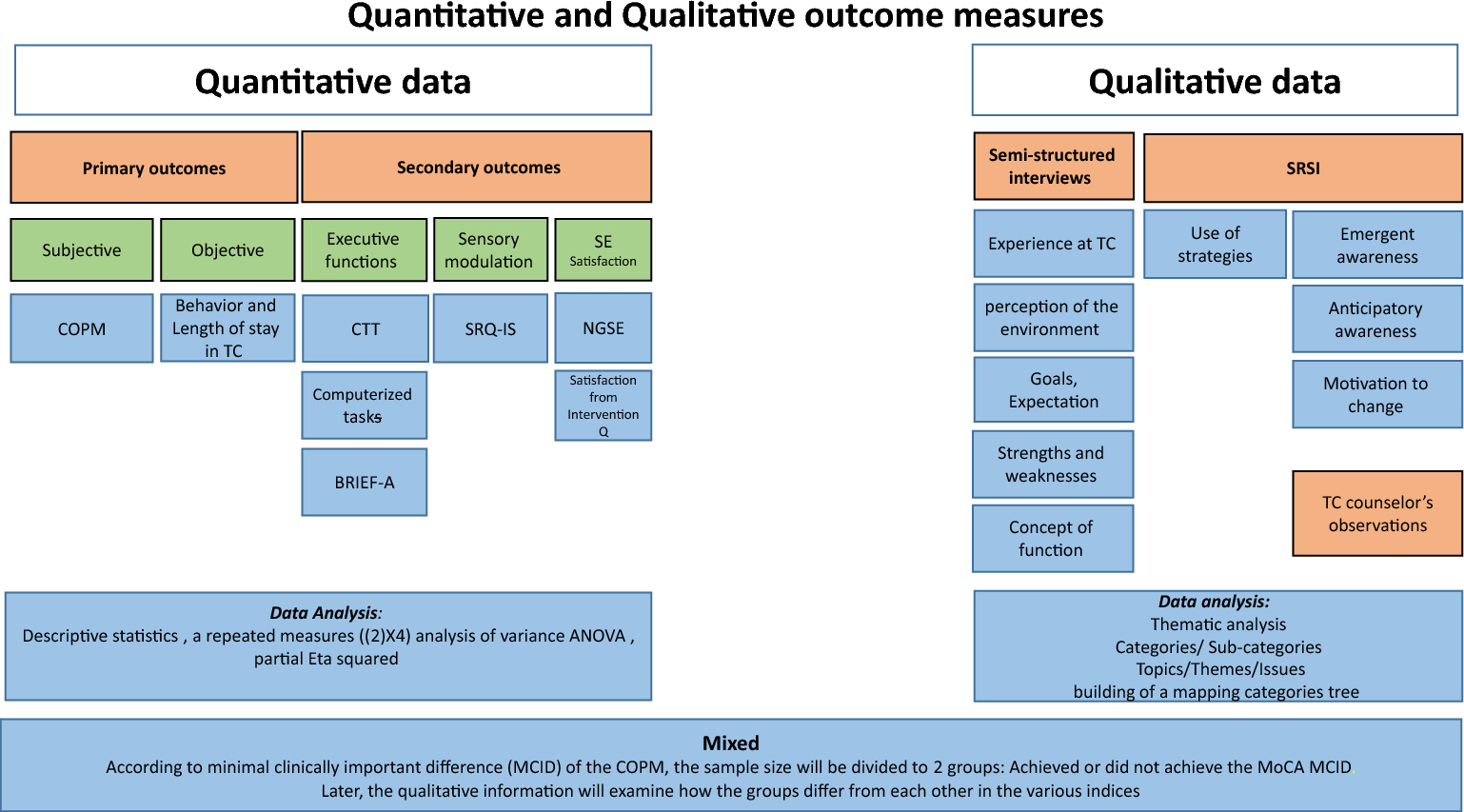
This includes questions about SU use of alcohol or any other substances, previous episodes of Stroke, Epilepsy, Brain Injury, or other conditions that may make wearing a cap or head garments difficult, uncomfortable, or painful. Furthermore, we will ask if participants are currently prescribed any antipsychotic, anti-depressive, or anti-anxiety medication. Quantitative and qualitative data will be collected through the outcome measuring tools (Table 1).
Table 1 Representation of primary and secondary outcomes, their labels and timepoints of administrationIndividuals allocated to GMT and IMT will be asked to attend 6 weekly therapy sessions each with a duration of 60 min. However, due to the planned EEG hyperscanning and necessary preparation time (ca. 35 min) as well as semi-structured interviews (20 min) in weeks 2 and 5 in the IMT group, participants in this group are required to attend for ca. 115 min in these weeks. Individuals allocated to CG will be asked to attend their usual care by the WDP care team. The ST that participants will receive from WDP may vary from week to week but will include a range of psychosocial and clinical interventions delivered in 1:1 and group formats. Over the 6 weeks we expect a participant to receive up to 180 min of ST (approximately 3 × 60-min WDP key work sessions—see below) but this is depending on individual needs. The participant may also attend other groups or appointments at WDP. After the interventions, GMT, IMT and CG will complete the same secondary outcomes measures again. Primary outcomes will be measured after the interventions in weeks 8 and 9 with a participant satisfaction survey and focus groups, respectively.
InterventionsMT involves the use of sounds and music within an evolving relationship between participants and therapist to support and encourage physical, mental, social, emotional, and spiritual wellbeing. Sessions will be delivered by a qualified music therapist, registered with the UK regulator for health and care professions, the Health and Care Professions Council (HCPC). Registered music therapists must have undergone training through an accredited Music Therapy training course, which is offered in the UK either in the form of a two year full time or three year part time masters level training (accredited by the HCPC).
MT sessions will be based upon musical improvisation, composing and writing songs, analyzing lyrics of preferred songs, singing and talking. Participants are not required to have any previous instrument or other music experience. During GMT, active and passive music activities will be conducted as a group. During MT sessions participants will be introduced to a range of both electronic and acoustic instruments, including tuned and untuned percussion, from which they can choose to play and improvise freely. The music therapist will accompany participants in the improvisation. This form of improvisation, with the support of the music therapists, provides participants with an opportunity to connect with emotions and feelings connected to unconscious material. Following improvisations, the therapist and SU may identify moments of interest which can be further explored either verbally or through further improvisation. Utilizing Electronic Music Production Instruments (EMPIs) provides participants with additional creative opportunities while utilizing contemporary timbres and music making techniques, thus offering participants a way to explore their musical and cultural identities [36]. The use of EMPIs also enables the recording of the music created in the sessions, which in turn provides dual benefits: firstly, participants can, if they wish, take a copy of the music they created away, and secondly, the recording can be used in the analysis of sessions.
GMT participants will have the opportunity to share any experiences and feelings arising with the group members. Through this shared experience group members can benefit from interpersonal learning, group cohesiveness and the development of social interaction techniques. ST includes 1:1 key work sessions, other group work programs and clinical support (e.g., prescribing, counseling, and clinical interventions).
Outcome measuresObjective (i.e., EEG-based) and subjective (i.e., multi-, and single-item questionnaires), quantitative as well as qualitative (i.e., interviews and focus groups) measures will be used to accomplish the aims and objectives of the present study (Table 1).
Outcome measures for each participant (GMT, IMT and CG)In this section, we describe mental health, substance use and craving measures that will be administered prior to (baseline) and after (post-intervention) the intervention; therefore, at week 1 and week 8. To measure participants’ depressive symptoms, the Patient Health Questionnaire (PHQ-9) will be completed, and a resting-state EEG frontal alpha asymmetry (FAA) will be measured. The PHQ-9 is a validated and commonly used self-report to screen for depressive symptomatology [37] and shows a good internal consistency when administered to participants with SUD (Cronbach’s α = 0.90; [38]). The FAA is a neural biomarker representing the difference between the left and right alpha activity over the frontal regions of the brain [39] and a reduced FAA has been associated with depressive symptomatology [40, 41]. To measure participants’ anxiety symptoms, the Generalized Anxiety Disorder-7 (GAD-7) questionnaire will be completed and resting-state EEG frontal midline theta (FMT) will be measured. The GAD-7 is a validated [42] and standardized [43] self-report to screen for anxiety symptomatology showing a good internal consistency when completed by SUD participants (Cronbach’s α = 0.91; [43]). FMT is a neural biomarker that has been associated with anxiety [44] and increased resting-state FMT positively correlated with the reduction of anxiety after an MT intervention for clients with depression [16]. To measure participants’ feeling of craving in the preceding 24 h, the Brief Substance Craving Scale (BSCS) questionnaire will be completed and resting-state EEG beta frequency band will be measured. The BSCS is a validated questionnaire to assess craving in the SUD population over a period of 24 h [45]. The EEG beta frequency band is a neural EEG rhythm suggested to play a role in processing abstinence-related and cue-induced craving [46]; indeed, increased resting-state beta frequency band activity in the dorsal anterior cingulate cortex and pregenual anterior cingulate cortex have been associated with craving [46]. After the resting-state EEG recordings, participants will complete a behavioral Go/No-Go task while EEG event-related potentials (ERPs) will be measured to assess inhibitory control. The visual Go/No-Go task is a straightforward behavioral paradigm requiring participants to respond with a button press when a set of stimuli are presented (circles appearing at the top right and bottom left corners of the screen) and to withhold the response when another set of stimuli, with the same probability of occurrence, is presented (circles appearing at the top left and bottom right corners of the screen) [47,48,49]. To measure substance use, days of primary substance used, usage of primary substance per day, physical wellbeing, mental wellbeing and overall quality of life, the Treatment Outcome Profile (TOP) questionnaire will be completed. The TOP is a psychological health scale validated in a sample of SUD participants [50] and a standard measurement tool used in community treatments services in England and Wales. Biomarkers, such as Urine Drug Screening (UDS) or breathalyzers, will not be used during this feasibility study. This is due to costs and added burdens to the participants and the hosting service. While the TOP is a self-reported measure, it is a questionnaire regularly administered to all service users and we expect it to provide indicative results of which can be followed up in further studies.
Additional outcome measures for participants in the GMT and IMT groupIn this section, we describe outcome measures that will only be administered to participants assigned to the GMT and IMT group. Each participant and the therapist will complete an attendance sheet after each GMT and IMT session to monitor participation rates. To measure and monitor for instantaneous level of craving intensity, a Craving Thermometer (in the form of Visual Analogue Scale [VAS]) will be completed before and after each GMT and IMT session by each participant [51, 52]. This measure represents a quick-scan of craving intensity and a threshold score of 3 on a craving VAS ranging from 0 to 10 has been shown to sensitively predict the presence of craving (p < 0.05; [51, 52]). To assess if the MT program, carried out alongside the ST, is acceptable as an intervention in a community setting, participants will complete a participant satisfaction survey at week 8. Participants will also have the chance to provide detailed feedback on the MT program through the survey. To assess the feasibility and acceptability of MT in addition to ST in a CSMTS, a focus group will be conducted at week 9 (two weeks after the end of treatment) to collect qualitative data on SU satisfaction. An exit questionnaire will be administered to participants who disengage with the intervention to gather qualitative data regarding their reasons for withdrawing.
Additional outcome measures for participants in the IMT groupIn addition to the measures listed above, and to test the feasibility of investigating mechanisms of change with neurophysiological research methods, participants receiving IMT will undertake in-session measures. The following outcome measures will only be collected at the 2nd and 5th sessions. To measure client-therapist alliance, the Helping Alliance Questionnaire-II (HAQ-II) will be completed by the participant and the therapist [53]. The HAQ-II is a questionnaire measuring therapeutic alliance and has been validated in a large sample of SUD [53]. To select significant-nodal moments for the client, a qualitative semi-structured interview will be conducted after the session 2 and 5. Important and emotionally relevant moments of the 2nd and 5th therapy sessions can be examined by reviewing specific time frames acquired in the AV recording of the session and the corresponding EEG concomitants [22]. Additionally, during those two sessions, EEG hyperscanning technology will be adopted to measure the brain activity from the therapist and the participant while interacting. This method has already been implemented in an MT setting by members of the research team to explore the neural correlates of client-therapist relationship during selected therapeutically interesting moments [21, 22].
Additional outcome measures for participants in the GMT groupFollowing completion of the MT intervention period, each GMT participant will be interviewed (audio recorded) by the music therapist. This individual qualitative debriefing interview will focus upon participant experiences of using music technology in music therapy sessions.
Focus groups for participants and WDP staffFollowing the completion of the entire intervention, the IMT, GMT and SG will be invited to attend focus groups lasting approximately 60 min. Two focus groups will be conducted. The first one for both the IMT and GMT participants. The second focus group will only include the SG. The focus groups will capture qualitative data on SUD participants’ acceptability, session feedback and suitability. The focus group for SG will explore feasibility and future implementation.
Electroencephalography (EEG) recordingThe pre-post intervention EEG recording procedure will include a 5-min eyes-closed resting-state, after which a 5.5-min EEG ERP recording during a Go/NoGo task will be performed. Those recordings will be accomplished utilizing 32 Ag/AgCl passive electrodes (R-Net, Brain Products, GmbH, Germany). The EEG resting-state frequency bands will be analyzed with Neuroguide (NG) software [16, 54, 55] while the ERP data will be analyzed using BrainVision Analyzer software (version 2.1.2; Brain Products GmbH) and MATLAB (R2021b) [56]. The EEG hyperscanning data will be recorded throughout the second and fifth therapy session from therapist and participant utilizing 32 Ag/AgCl active electrodes (ActiCap, Brain Products GmbH, Germany). Artifact control will be guided by video recording of the IMT session and by notes taken during recording. Pre-processing and processing steps to analyze neural time-series data will be performed with BrainVision Analyzer software (version 2.1.2; Brain Products GmbH) and will follow our previously published study [22]. All baseline resting-state EEG recordings will be reviewed for potential clinically relevant findings (incidental findings) by a Consultant in Clinical Neurophysiology (A.M.).
Analysis strategy regarding the main study aimData analysis of the main study aim will be performed by comparing feasibility-related measures collected at the end of the treatment between participants allocated to the IMT or GMT groups. Descriptive statistics will be used to examine the rate of acceptability and satisfaction in these two experimental groups. Primary outcome measures (feasibility-related measures) that will be used are: (I) retention in treatment, which will be assessed by collecting attendance sheets and treatment status. The treatment status from participants receiving IMT, GMT and ST will be collected by WDP’s case management system 1-month post-intervention. This will provide information about retention in treatment, treatment engagement and completion rate. (II) Acceptability of treatment, which will be assessed by collecting a participant satisfaction survey as a post-intervention measure (at week 8) and implementing two post-intervention focus groups (FG1 and FG2) (at week 9). Primary outcome measures will only be administered/conducted after the end of the intervention with the aim of collecting the subjective perspective of the participants and staff involved in focus groups and will be subjected to thematic analysis using a specific thematic analysis model [57]. From this data themes will be identified pertaining (I) to participants' experience of MT in a CSMTS and (II) to participants’ experience of using music technology in music therapy.
Analysis strategy regarding the secondary study aimsThe strategy for the secondary aims entails data collection and analysis of quantitative and qualitative data from the EEG, questionnaires, a behavioral task, and a semi-structured interview. To analyze the effects of an MT program (GMT/IMT) in addition to ST compared to ST only on secondary dependent variables, descriptive, graphical, and inferential analyses will be used. Effect sizes will also be computed where relevant. The present research is a feasibility study and because of the small sample size, certain inferential statistics requirements cannot be satisfied. Therefore, results related to the secondary aims are to be considered—and will be presented as—preliminary. Descriptive analyses will be conducted by calculating means and standard deviations at each time point. Inferential statistical analyses will be conducted to evaluate the effect of MT (GMT/IMT) in addition to ST on mental health and brain processing by comparing the data between pre- and post- intervention in each group using a parametric or non-parametric test (e.g., paired t-test or Wilcoxon Signed-Rank test, respectively) depending upon the data distribution. The dependent variables that we will measure are pre-post intervention changes in the following outcomes: (I) score of the PHQ-9 and resting-state FAA for depressive symptoms; (II) score of the BSCS and resting-state beta frequency band for the craving state experienced over a 24-h period; (III) score of the GAD-7 and resting-state FMT for anxiety symptoms; (IV) score of the TOP for substance use, days of primary substance used, average usage of primary substance per day, physical wellbeing health, psychological health, and overall quality of life; and (V) P3 EEG event-related potential amplitude and behavioral accuracy during a Go/No-Go task for the inhibitory control. The statistical procedure to analyze data from pre-post intervention questionnaires involves both within-subject (or repeated-measures design) and between-groups (or independent design). Indeed, a pre-post intervention comparison of scores from the questionnaires will be performed for each group (GMT, IMT and ST) with a paired-samples t-test. In case the assumptions of normality and homogeneity of the data will be violated, a non-parametric Wilcoxon Signed-Rank test will be performed. The difference scores obtained from this repeated-measures design, will be used for the independent design analysis: pre-post intervention difference scores in the questionnaires administered to the MT groups (GMT and IMT) will be compared with pre-post intervention difference scores in the questionnaire administered to the ST group utilizing independent t-test. In case the assumptions of normality and homogeneity of the data will be violated, a non-parametric Mann–Whitney test will be performed.
For the resting-state EEG data (alpha—FAA -, beta, and theta—FMT—bands) pre-post intervention comparisons will be performed utilizing z-scores from a Normative EEG database (NG software) [54]. Furthermore, to represent the pre-post intervention difference in the topographic distribution of EEG power in the selected frequency bands a paired-samples t-test will be performed for each of the three groups. If deviations from normality will be found in the data, a non-parametric Wilcoxon Signed-Rank test will be performed. Between-group power differences will be calculated as well, by comparing differences in the topographic distribution of the EEG power in participants who received MT (GMT and IMT) alongside ST vs participants who received ST only through an independent t-test. If deviations from normality will be found in the data, a non-parametric Mann–Whitney test will be performed. Relationships between changes in the pre-post intervention questionnaire scores (PHQ-9, GAD 7, BSCS, VAS, HAQ-II) and changes in the respective EEG measures (see above) will be tested using Pearson's correlation coefficients with 95% confidence interval [16]. Likewise, we will implement the same correlation procedure to test the relationship between pre-post intervention changes in inhibitory control (P3 ERP amplitude and accuracy on “no-go” trials) and changes in the scores of the Brief Substance Craving Scale. Changes in the pre-post MT (GMT and IMT) sessions scores from the craving thermometer will be analyzed graphically (i.e., scatterplot). Those who attend more than two sessions but disengage before the study ends will have the measures up to the point of their disengagement included in data analysis.
Analysis strategy regarding moments of therapeutic interest and music technologyA qualitative data analysis serves to transcribe, identify, and code relevant and pivotal moments of the therapy and associate them with neural markers of emotional processing, following the procedures described in previous studies conducted by members of the research team [21, 22]. These moments will be referred to as moments of interest (MOI) and will be selected and identified to describe a narrative of the therapeutic change process and to analyze EEG event-related temporal dynamics during MOI as compared to moments of non-interest (MONI). More specifically, we plan to analyze the time-course of EEG power in alpha and theta frequency bands [22], which have been shown to be associated with emotional processing and neuropsychiatric symptoms [40, 41, 44]. By examining changes in these frequency bands in therapist-client dyads across sessions, we may obtain an indication of the underlying neural mechanisms involved in the therapeutic process. Observations from the therapist and a semi-structured interview will be utilized to select MOI by importance and emotional relevance. Participants may also report verbally any craving-related experience, which would also allow us to describe instances of neural dynamics of craving. MOI will be identified and located in the AV recordings of sessions. These reports and their timestamp of occurrence will be entered into a therapy event log. This semi-structured interview will also be conducted to explore participants' perspective and experience of using music technology in a music therapy intervention. HAQ-II will be completed by the IMT group and by the therapist after session 2 and 5 to graphically explore the dynamics of the therapeutic relationship and correlate with outcome measures. Audio–video recordings of individual sessions will be transcribed with ELAN [58] Version 6.2, Max Planck Institute for Psycholinguistics, Nijmegen, The Netherlands). MOI and MONI will be identified by the client, the music therapist and by an independent music therapist acting as a second rater. The analysis of interview responses and transcriptions of video recordings will be subjected to thematic analysis [57]. From this data themes will be identified pertaining (I) to participants' experience of MT in a CSMTS and (II) to participants’ experience of using music technology in MT. The research team will identify themes within the free text boxes of the post-MT questionnaires, satisfaction and exit surveys, and the discussions recorded within the focus groups. Audio recordings of the musical components will be analyzed using aural and spectral analysis while Musical Instrument Digital Interface (MIDI) data will be subject to computational analysis using the Music Therapy Toolbox (MTTB) [33].
Comments (0)