KMs have been proposed to occur due to delayed tooth eruption and odontogenic cysts [2, 3], and related to mucopolysaccharidosis [4], the mechanism of KMs development has not been completely deciphered. So far, 57 cases of KMs have been reported, of which 7 were juveniles (< 18 years old) [4,5,6,7,8,9,10]. All the seven cases had class I or class II KMs, the direction of the occlusal surface was near centrifugal, and the root of the tooth was complete (Table 1).
Table 1 KMs detected in younger patientsKMs are classified based impacted teeth type into class I (mandibular first molar and second molars), class II (mandibular second molar and mandibular third molars), and class III (mandibular third molar and mandibular fourth molars [11]. Nedjat-Shokouhi et al. [5] and Menditti et al. [12] classified KMs with contact between occlusal surfaces as true KMs and those without occlusal surface contacts as pseudo KMs. They further distinguished KMs into cystic variants with cyst-like transmission images and those without cystic variants without cyst-like transmission images on X-ray images. Moreover, the fourth molars impaction, defined as class 3, is the fourth most common after maxillary median, maxillary fourth molars, and maxillary lateral incisors [13, 14]. Class III KMs are further classified into molars and posterior teeth KMs based on their location [15]. KMs are further classified based on structure into cylindrical, nodular, and funnel-type forms [16, 17] and based on buried positions into vertical, inclined, and horizontal KMs [18].
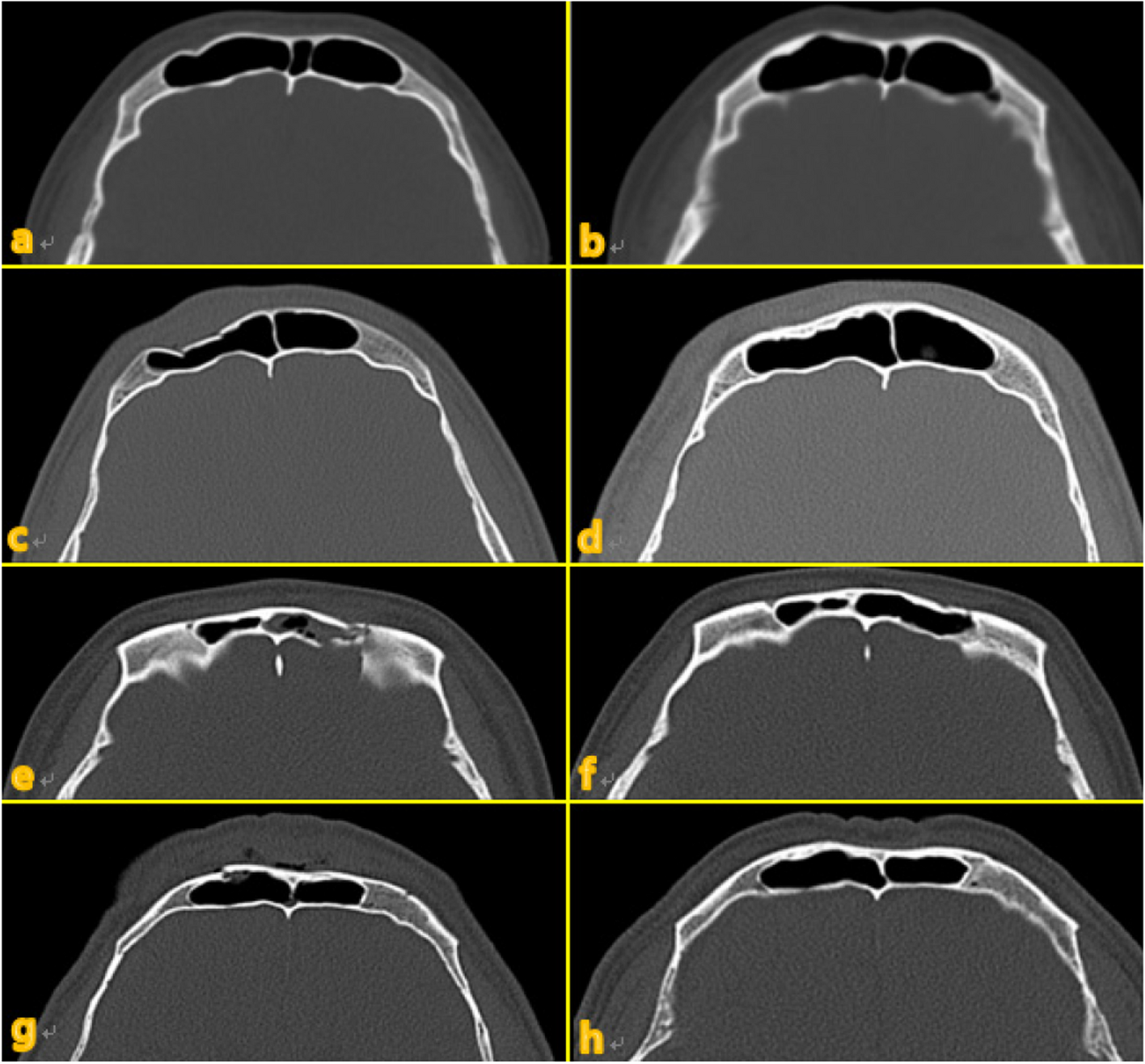
However, evaluation of the morphology and impacted position of the tooth are difficult in people with incomplete root formation and alignment of teeth. Moreover, in class III KMs with incomplete root formation and KMs located on the buccal side, detection of impaction is difficult using panoramic X-rays.
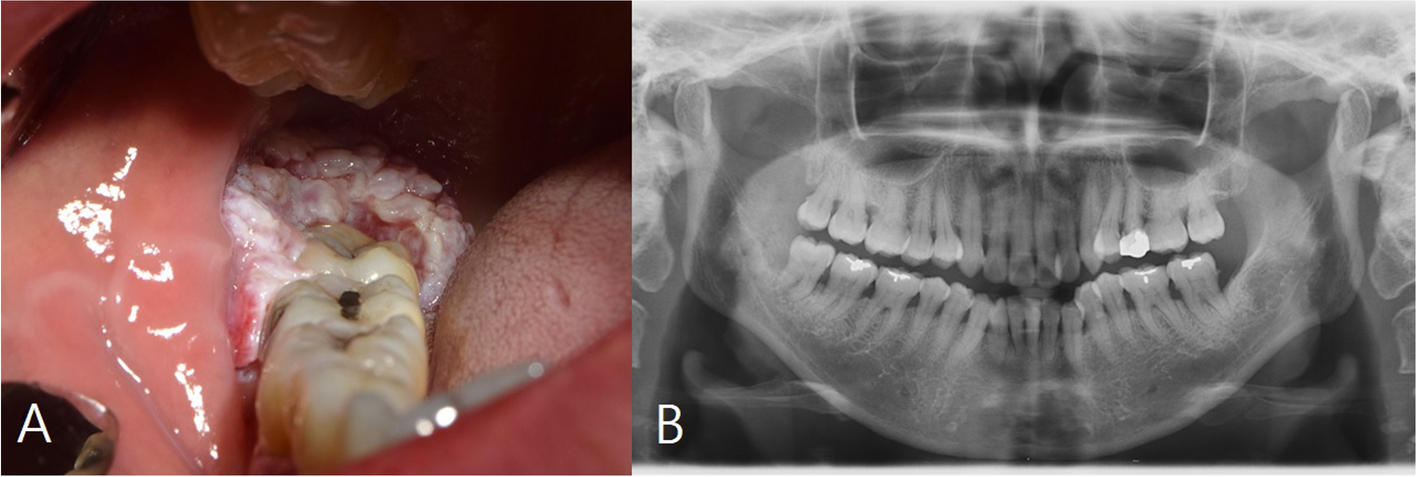
Shahista et al. have reported the case of the youngest patient so far with class III KMs [19]. As the patient was 21 years old, we propose that class 3 KMs are rarely detected early. Moreover, young people generally do not consider wisdom tooth extraction unless symptoms appear or orthodontic treatment becomes necessary. In this case, the patient was referred from a nearby dental clinic, and an odontogenic cyst was detected based on panoramic X-ray images with no excess teeth protruding. These results suggest that in many cases, KMs are confirmed by dentists after the root formation and wisdom teeth eruption. The movement of impacted teeth within the jawbone [20] occurs in the bone marrow with little resistance during root formation as teeth move toward the crown due to the blood flow pressure through the apical foramen. Moreover, impacted teeth movement is more common in single root teeth and teeth with little root diastasis. Thus, class III KMs are impacted on the buccal side during the embryogenesis stage and move in the jawbone during teeth root formation.
In this case, the fourth molar was located on the buccal side from the impacted position, and the third molar was horizontally impacted. Additionally, the pulpal cavity morphology of the X-ray image suggests that the third molar had a single root, and the excess tooth had a compound root. Thus, with no treatment, the third molar with no single root may have moved upward in the bone marrow at the anterior edge of the mandibular branch instead of in the direction of the dense buccal shelf due to the presence of the compound root of the excess teeth. Therefore, the patient may be diagnosed with true KMs class III with cystic variant exhibiting an inclined buried position.
Treatment of KMs is often selected on class classification using X-ray images, the presence or absence of cystoid transmission image, and clinical symptoms. Tooth extraction is performed in all cases with cyst-like transmission image observed in past reports. Moreover, class III cases are difficult to induce eruption, and tooth extraction is often recommended [21]. However, class I and II cases are often juvenile. Orthodontic treatment is recommended in cases where dentition can be guided regardless of the presence or absence of cyst-like transmission image, using fenestration in combination [8].
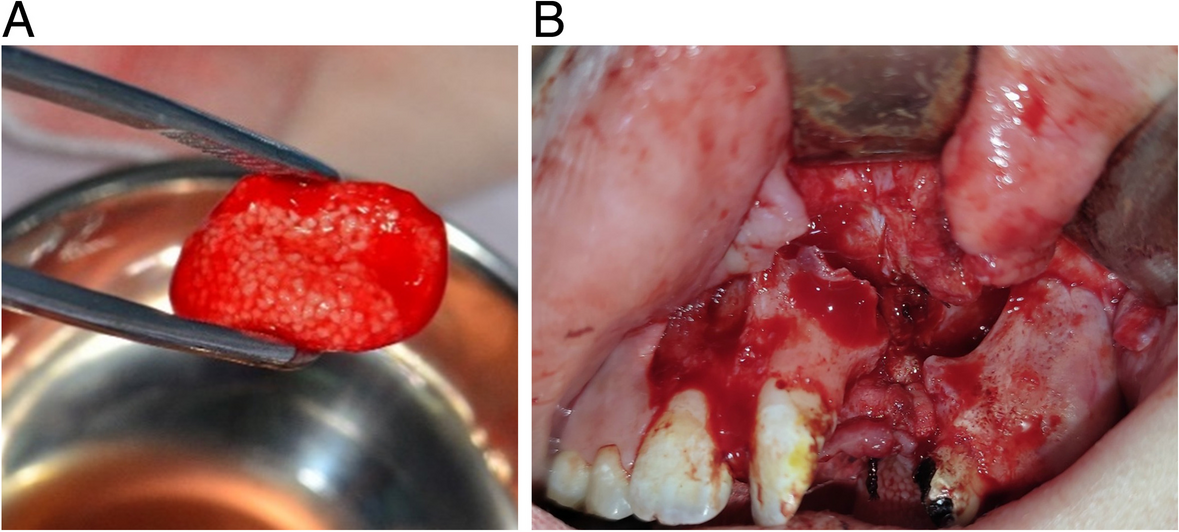
In this case, tooth extraction was selected because of (1) awareness of discomfort during occlusion, (2) KMs being class III, (3) the necessity of removal of cyst-like structures, and (4) the possibility of complicated malocclusion and tooth extraction procedures with the completion of the tooth root formation.
The recommended timing for extraction of KMs is not reported yet. However, early tooth extraction should be considered regardless of age, especially in class III cases.

留言 (0)