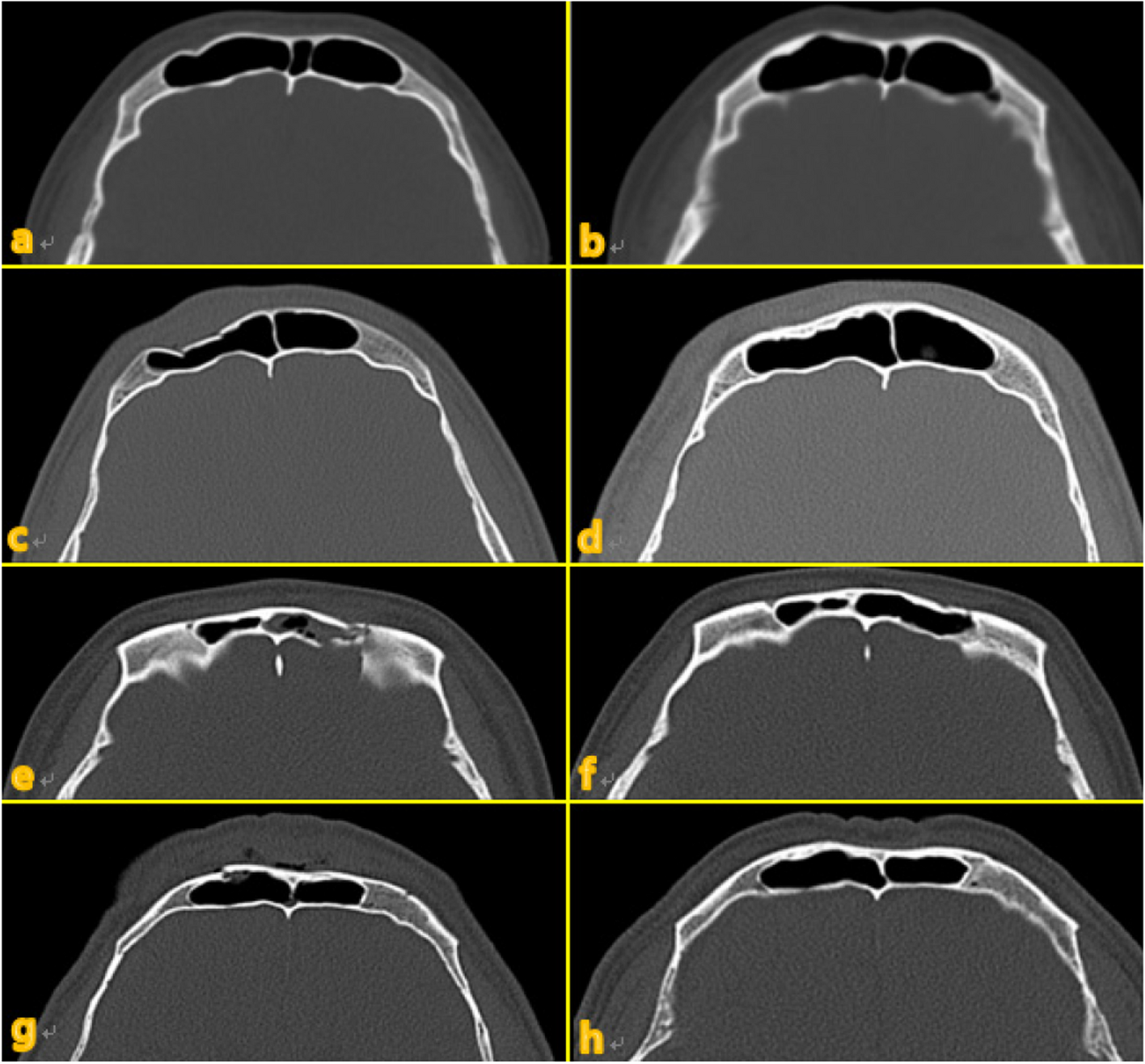
According to the 2005 WHO classification, the treatment strategy for primary AC is the same as that for the secondary (dedifferentiated) endosteal/periosteal type, and the advanced secondary type is difficult to distinguish histopathologically from the primary type. Therefore, the 2017 classification was revised to a single disease classification [6,7,8]. The incidence of AC is reported as 11 cases (0.21%), out of 5,231 odontogenic tumors, and in other countries, it is reported to account for approximately 1.6–2.2% of all odontogenic tumors [9,10,11]. The average age of AC incidence is 45.9–49.4 years, males are approximately twice at risk compared to females, and involvement of the mandible is approximately twice as common as that of the maxilla [12, 13]. Clinically, AC is more destructive and invasive than ameloblastoma (AB). It is also characterized by a variety of symptoms including swelling with rapid growth, cortical bone perforation, pain, ulcer or fistula formation, facial asymmetry, dysphagia, and dysesthesia [2,3,4,5]. However, approximately 38% of ACs may be characterized only by painless swelling and lack typical clinical symptoms [2, 3]. Furthermore, the diagnosis rate of preoperative AC is reported, invasion as low as 39%, and preoperative diagnosis is considered difficult [14]. In the past 10 years, 13 (61.9%) of 21 cases of AC in the area of the bone of the jaw were diagnosed as benign tumors (Table 1) [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31]. On the other hand, 7 cases (33.3%) led to a diagnosis of a malignant tumor. In this case, the preoperative diagnosis was SCC. The CT images of ACs are often characterized by malignant tumor images with indistinct borders, bone destruction, invasion into the surrounding soft tissues [2, 32, 33]. However, similar to ABs, ACs are often associated with well-defined, single/multifocal radiographic findings [4, 5]. In this case, CT images showed bone disruption and soft tissue invasion in the surrounding area. MR images showed a strong high signal on diffusion-weighted images, and the tumor parenchyma could be identified. Histopathologic features of AC are pleomorphism, fission, focal necrosis, perineural invasion, and hyperchromasia of the nuclei, in addition to the histopathologic findings of AB. Hall et al. reported the pathological findings of general AC to be the absence of a central stellate reticular region and the presence of epithelial cell aggregates, cytosolic plexiform or insular, hyperchromatin, dense cellular arrangement, atypical nucleoli, focal necrosis, and neural and vascular invasion [34], which can make it difficult to distinguish from AB. Therefore, immunochemical staining is used to differentiate ACs from ABs. In particular, Ki-67, p53, and α-SMA are known to be useful markers [33, 34]. Ki-67 and p53, markers of tumor cell proliferative activity, are highly expressed in AC. Kase et al. proposed diagnostic criteria for AC as a Ki-67 positivity rate of 10% or higher [35]. In addition, ACs with clear cells have anaplastic features and are more invasive than ACs without clear cells and have higher recurrence and mortality rates [36, 37]. In this case, there were no clear cells, and the tumor cells formed foci with stellate cell like cell proliferation, keratinization, squamous metaplasia, vacuolation, and blister necrosis; lymphatic invasion was also observed. Ki-67 showed more than 80% expression in the affected area, and AC was finally diagnosed. The occurrence of AC has been considered attributable to the contact of malignant epithelial tumors with calcified, dentin-like, and bone-like hard tissue formations, and the tumor epithelium of AC is thought to have an inductive effect on the tumor mesenchyme [38]. Other reports are suggesting that the remaining tissue of the tooth embryo may have originated from the entrapped salivary gland epithelium, but this remains to be clarified [31, 38]. Surgical resection is the first choice of treatment for ACs, and the efficacy of radiation chemotherapy has not been established [31, 35]. There is no association between prophylactic neck dissection and improved survival, and postoperative radiation therapy has been shown to be beneficial in cases of invasion into the surrounding soft tissue or positive margins [39]. In this case, the preoperative diagnosis was SCC (rT4aN0M0); therefore, prophylactic neck dissection was performed with a safety margin of 10 mm according to the procedure for malignant tumors. Intraoperative rapid diagnosis confirmed the negative margins; the final preparation also had negative margins, and there were no metastatic findings in the excised lymph nodes.
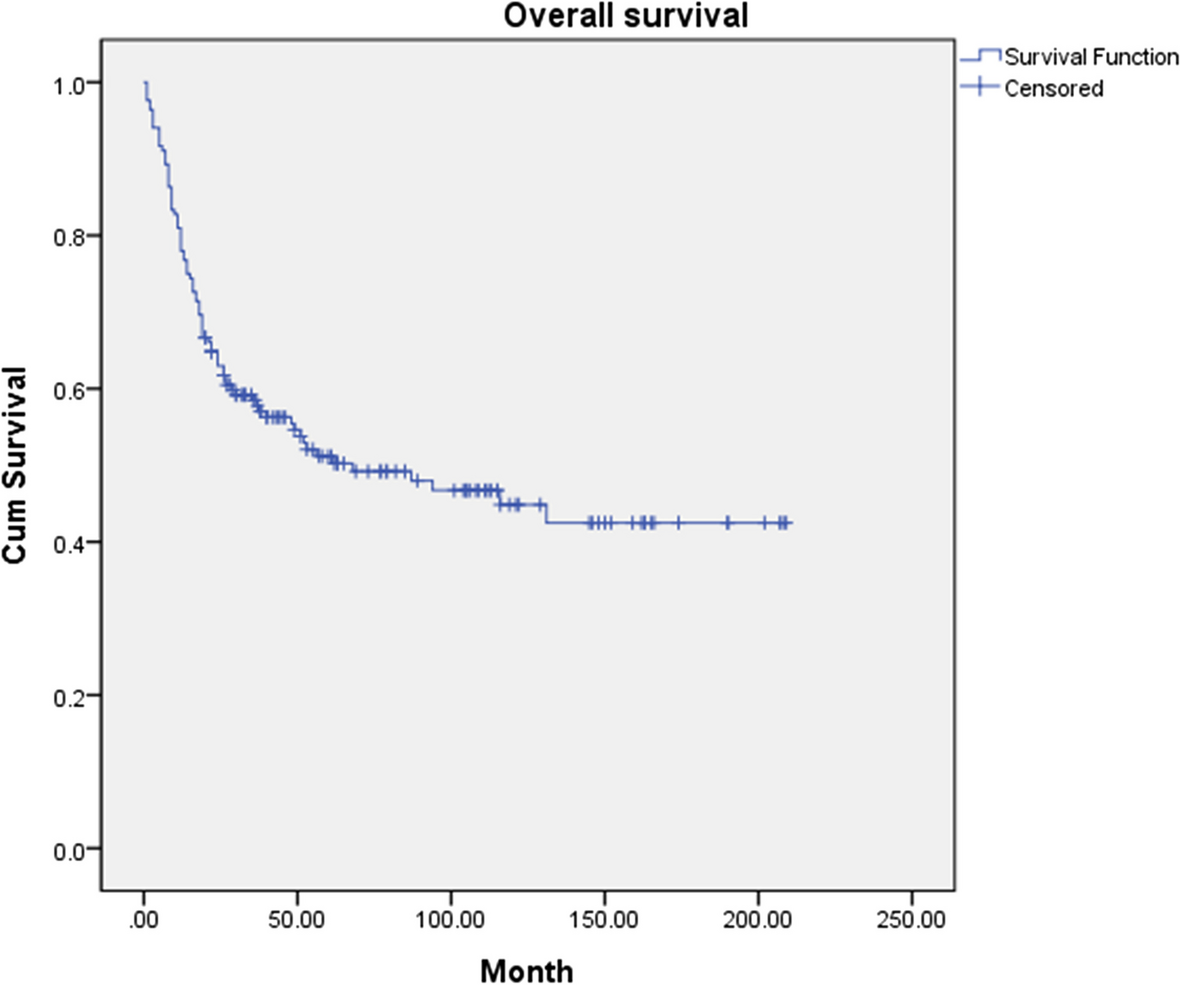
Table 1 Reports of AC in the jawbone region in the last 10 yearsThe 5-year survival rate of AC is 69.1–83.2%, which is relatively high [39,40,41], but it decreases to 0–21.4% in metastatic cases [39, 40], and the recurrence rate is said to be 20.9–38.4% [12, 32, 41]. As for distant metastases, the lungs are the predominant site, with an incidence of 15.4–22.0% [32, 42, 43]. A characteristic feature of AC is the long time until recurrence or distant metastasis: the time to recurrence is 47.5 months, and the time to distant metastasis is 84.7 months, although cases occurring after 156 months have also been reported [40]. Therefore, long-term follow-up of ACs is important [39, 40], and Jaitley et al. recommend CT evaluation every 6 months [43].
Recent developments in molecular biological techniques have improved tumor therapy. Osteogenic tumors are associated with a high incidence of BRAF-V600E mutations, which have been suggested to be associated with AB invasion [42, 44,45,46,47]. Two targeted agents, dabrafenib, which blocks the action of BRAF mutations, and trametinib, a MEK inhibitor, have been reported to be effective in patients with ABs and lung metastases [48]. In the future, targeted drug therapy for ACs with BRAF-V600E mutations is suggested. In this case, there was no suspicion of recurrence or metastasis on CT at 6 months postoperatively. However, it is necessary to perform long-term local and systemic follow up in such cases.

留言 (0)