
記住我








Given the toll the life of a surgeon exerts on oneself mentally, emotionally, and physically, a call to action is warranted. It is evident that the issue of burnout is too prevalent and pervasive to simply be addressed by a single person, group, or process. A multi-faceted plan to address burnout is essential. This idea of addressing burnout at multiple levels was described in depth by Dr. Shanafelt et al. in a Lancet publication in 2016 [44]. Further exploration of this topic in the Journal of Internal Medicine described how addressing burnout should be a “shared responsibility across healthcare systems, organizations, institutions and individual physician.” [45]. Most recently, in October 2022, the National Academy of Medicine published its National Plan for Health Workforce Well-Being. This model creates a Clinician Well-Being Collaborative Systems Map which is a multi-item intertwined web including health systems, patients, health workers, academic institutions, professional and specialty societies, clinical training programs and academic bodies, health information technology companies, insurance and payers, and federal, state, and local governments [46].
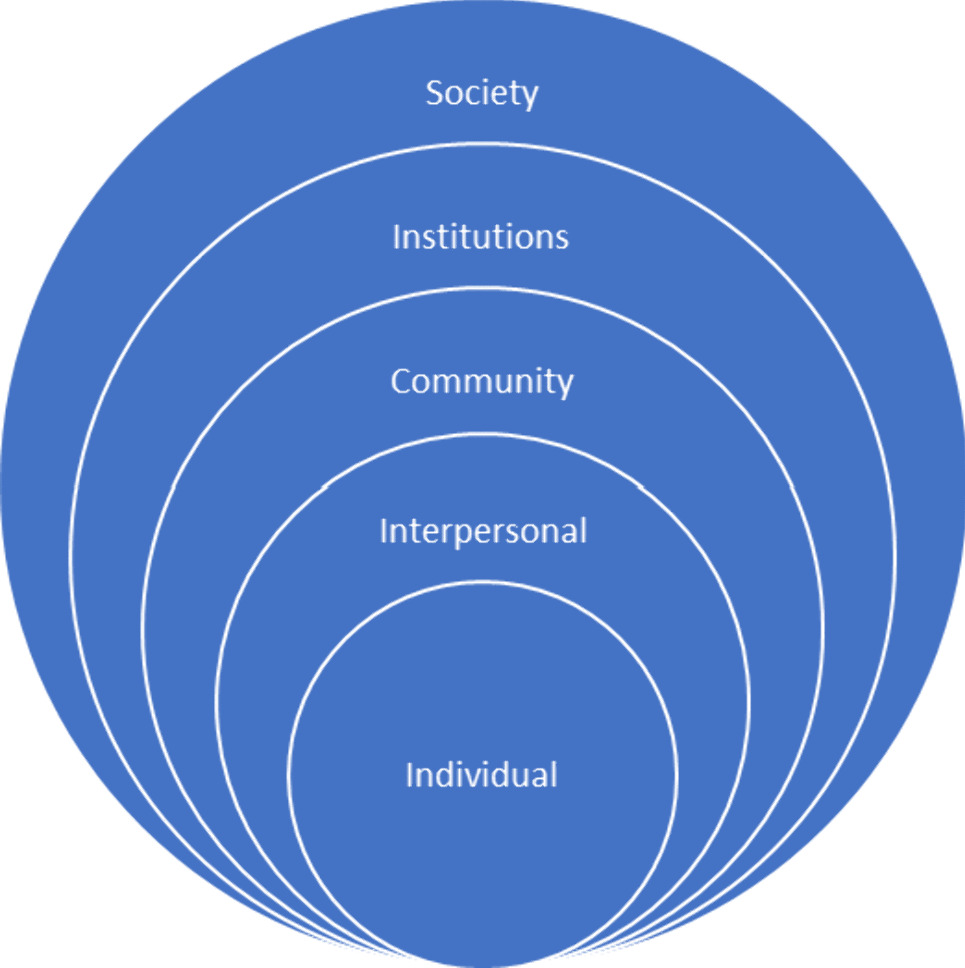
A proposed three-pronged approach, based on these aforementioned ideas, but narrowed in scope to specifically address burnout in surgeons, is demonstrated as a Conceptual Model in Fig. 2. The model includes actionable items on the individual, institutional, and national levels with defined ideas introduced at each level. The double-sided arrows in the model represent engagement and interaction between the categories, which is compulsory for sustainable and durable results. Surgeons should use these examples as a guide to tailor their own personalized wellness toolbox. Table 1 depicts studies dedicated to improving burnout under the categories of individual, institutional, and national.
Fig. 2
Novel conceptual model for classifying actionable measures for surgeons at the individual, institutional, and national level
Table 1 Burnout and well-being in surgical literature at the individual, institutional, and national levels (2017–2022)IndividualThe ability to recognize and subsequently address feelings of fatigue, depersonalization, and lack of accomplishment in one’s self is critical in the mission to combat burnout. Three factors positively correlated with well-being are emotional intelligence (EI), resilience, and mindfulness. High EI has consistently been shown to protect against burnout [21, 47, 48]. Resilience, or the capacity to recover quickly from adverse and challenging situations, is inversely associated with burnout risk [9]. Prior mindfulness-based interventions have demonstrated improved performance, stress-management, and quality of life [49]. The following subsections depict specific examples in each of these categories that have shown to be successful in decreasing burnout at the individual level. Additional studies are listed in Table 1.
Emotional IntelligenceSelf-compassion, a positively described method to respond to oneself in challenging times, contributes to emotional intelligence. Common humanity and self-kindness are deemed compassionate responses. Self-criticism and isolation are negative dimensions of self-compassion and are related to healthcare worker burnout. Kratzke et al. thus modified a previously developed self-compassion program to administer to surgical residents over a 3-year period at a single academic institution [50]. The program consisted of multiple sessions over a 6-week course by certified teachers of mindful self-compassion with the goals of both explaining how self-compassion can promote well-being and to provide tools to practice self-compassion. Post-program there was improvement in depression and emotional exhaustion.
A more wide-scale example of an EI related initiative is the randomized control trial (RCT) conducted nationally examining the impact of a virtual Professional Development Coaching Program on 237 women surgery resident participants [51]. Coaching has been shown to promote reflection while strengthening awareness and motivation. Through the Association of Women Surgeons, female surgery residents were recruited and randomized to intervention with three 1: 1 coaching sessions over a nine-month period or the control group which entailed receiving wellness resources via email. Those in the intervention group had an increase in personal fulfillment, self-valuation, PERMA scale (positive emotion, engagement, relationships, meaning, and accomplishment), and decrease in burnout.
An opinion piece was published in 2017 in the American Journal of Surgery entitled “Sustaining a Career in Surgery” [6]. The article points out the high attrition rate of trainees emphasizing the need to highlight the importance of well-being early in the surgical career path. A table in the article lists individual emotional strategies which include the following: “protect and mature important relationships, debrief with trusted friends and family after stressful events, and seek professional help for symptoms of depression or anxiety.” These recommendations are pertinent from intern year to a surgeon nearing retirement.
ResilienceIn a single-institution study, surgical interns attended 8 resilience coaching sessions by a certified professional coach over the course of one year. The course included both group and individual components with the individual sessions specific to the resident’s needs. The residents stated the sessions provided useful skills and appreciated being able to talk to an unbiased party about any issues they may be struggling with at work or in life [52]. The Brief Resilience Scale scores increased significantly, though the interns noted that people who were more dedicated to the program likely got the most out of it. The PGY-1 residents had concerns with the durability of the coaching program; thus, feedback was to have the sessions for all years of residents, not just interns [52].
Two small randomized trials were performed to determine the effects of Enhanced Stress Resilience Training (ESRT) in surgeons [53]. At two institutions, ESRT was given to surgical interns for 8 weekly 2-h classes. The results demonstrate that ESRT may benefit executive function, burnout, and psychological distress. The authors recommend further tailoring the intervention for more optimal results.
MindfulnessLebares et al. performed a pilot RCT of a modified mindfulness-based stress resilience training on surgical interns over the course of 8 weeks [54]. The structure included 2-h classes and 20 min of suggested practice at home. The results demonstrated that the interns were feasibly and independently able to integrate learned mindfulness skills into personal and professional settings.
A pilot study investigating mindfulness in the operating room was performed at the Medical University of South Carolina [49]. Described as a brief intervention, a 25-min mindfulness training and a 4-min audio recording of a breath awareness practice were administered to attendings, residents, and anesthesiologists in attempts to improve mindfulness, focus, and stress. The authors concluded that the intervention is feasible and efficient and improved factors associated with burnout including decreasing stress and increasing mindful awareness.
InstitutionalWhile individual insight is crucial to abate burnout, it is too large an issue to remain at this level alone. To quote Lebares et al. “to address burnout and distress in medicine, institutional change is necessary” [53]. Since the detrimental effects of burnout have been brought to light in the surgical community, multiple hospitals and residencies began to incorporate strategies into their programs in attempts to alleviate burnout. This section highlights institutional endeavors across the country, specifically focusing on initiatives, mentoring, and support. The different initiatives are varied in duration and time-commitment with diverse efforts trialed across the country. Additionally, many expert opinions call attention to the importance of mentorship in surgery [55]. Unique surgical mentorship models have been described, with the intent of creating long-lasting and trusting relationships. Of note, Accreditation Council for Graduate Medical Education (ACGME) Program Requirements state “self-care and responsibility to support other members of the healthcare team are important components of Professionalism” [56]. The takeaway of the support aspect is the importance of the department’s willingness and assistance to personalize and adapt these initiatives to maximally benefit the group. In Table 1, the studies dedicated to improving burnout at the institutional level are detailed, a representative sampling described below.
InitiativesErgonomics training has been a popular adjunct to well-being initiatives given that studies demonstrating physical pain are positively correlated with burnout and posture may be associated with depression. The University of Miami piloted a 3-module training course taught by physical therapists over the span of one year. After completion of the modules, 85% of residents reported reduced neck and lower back pain and 93% stated they believed they would “physically perform better in the operating room” [57]. A study out of Northwestern organized a didactic teaching and a personal posture coaching session for their general surgery residents which both improved knowledge about ergonomics and reduced the severity of residents’ musculoskeletal symptoms [58].
As a response to increasing rates of burnout in surgeons nationally, a program called “Balance in Life” was established at one residency program. Elements of Balance in Life include 24-h fridge with snacks, peer mentorship program, annual team building retreats, weekly facilitated group intervention, and 90-min therapy sessions every 6 weeks with a psychologist. The faculty have ensured protected time for residents to be able to attend. The authors note how having contact with a licensed therapist through the program has in turn led to residents seeking their therapists independently [59].
At the University of Arizona in Tucson, a formal resident well-being and resilience program was instilled through monthly experimental sessions [60]. The sessions occur during educational time and are interactive, based on energy leadership, which is an executive coaching model. A qualitative assessment showed that the skills were applicable to daily life as a resident and they are working to further modify and tailor the program to evolving needs of the residency. This intervention decreased residents’ perceived stress and emotional exhaustion while it improved their life satisfaction and emotional intelligence.
MentoringStructured mentoring programs have also been associated with decreased burnout and attrition rates. Lack of faculty mentorship has been associated with lower scores of personal fulfillment [40]. In a novel and innovative mentor structuring system, a group at University of Michigan came up with anastomosis families [61]. The mentoring program consisted of vertical groups (7) with 1–2 medical students, a PGY-1 intern, a PGY-1 research resident, and a faculty member. The groups had casual meetings every 3–4 months with an agenda of half the meeting focused on reflection and the other half holding an evidenced-based discussion on a surgical topic. The researchers hope to analyze and publish the perceptions of this program in a mixed-method study in the next 1–2 years.
At University Hospitals in Ohio, Bingmer et al. created a model for formal mentorship in residency [62]. It was structured as a year-long program with assigned mentors with two social events and recommended mentorship meetings. After the intervention, there was an improvement of resident perception of faculty in the categories of involvement and support, which can be seen as protective against burnout and attrition.
SupportDepartments, in essence, determine success of aforementioned initiatives by demonstrating their dedication and prioritization of the efforts. Specifically, the department needs to be flexible to resident and faculty scheduling to increase attendance, offset clinical responsibilities during these times, and not just recognize but champion the importance of the interventions [50]. If the leadership in the department is not supporting the anti-burnout initiatives, the fear is they will not be well-attended or strictly enforced [52].
At Stanford, a team created a human-centered design (HCD) sprint where residents over a 1-h time period interviewed one another regarding what is most important for their own well-being during residency. Of the participating residents, 77% deemed well-being lectures, emails, and curriculum “Not Useful” and 42% replied the same “Not Useful” in regard to mental health reflection and therapy. For the response of “Most Useful,” 42% of residents responded with scheduled breaks or free time, and there was a strong preference for increased social activities. This initiative demonstrates support by soliciting feedback on previous and current interventions. The responses are sent to department leadership to effect changes and continue work to optimize their wellness programs. The authors summarize the importance of tailoring programs and opportunities specifically to the needs of their own residents [43].
Another simple and time-efficient tool that may be used to quickly assess well-being weekly is fuel gauge [63]. This single-item survey was distributed over 2 years at the University of Texas Southwestern (UTSW) Medical Center with the question “Overall my well-being fuel tank is” and the response 1–5 on a Likert score from empty (1) to full (5). There is a space to add any additional comments if desired. The residents reported it was feasible and well-received while the program administrators valued its utility in ascertaining which residents may be struggling. When a score of 1–2 was submitted, the program director (PD)/associate program director (APD) would reach out to the resident and check in, offer support, or give certain resources as needed.
NationalThe ultimate component of the call to action for addressing burnout exists at the national level. It is imperative to recognize that without the aid and encouragement of national surgical organizations, individual and institutional ventures have limitations. National committees and leaders dedicated to surgeon well-being both strengthen and enforce the cause. Official policies legitimize and ensure durability of proposed solutions. Opportunities created across state lines increase camaraderie and provide for an exchange of ideas at a broader level. National leaders have a responsibility to their constituents to prioritize the surgeon epidemic of burnout. Examples of papers exhibiting national-scale effects are displayed in Table 1.
PoliciesIn an opinion piece, the author states that people need to embrace the generational changes and accept changes, many for the better, in what is expected from oneself, our co-workers, and our employers. Progressive policies need to be instated including, but not limited to, parental leaves, mid-career retraining, part-time work opportunities, and an emphasis on career development [64]. There is also mention of the utilization of medical scribes and/or other routes to decrease the burden of documentation. The administrative burden of documentation is both something that is not required for a physician to practice their profession and that can be performed by other individuals with training in this area. However, until policies are put into place to offload clerical work to another party, physicians will continue to experience increased dissatisfaction with the job and a reduced sense of personal accomplishment.
Conflict between family obligations and work as a surgeon has been linked to decreased career satisfaction and burnout. This phenomenon has been demonstrated in both sexes; thus, progressive policies in categories such as breast-feeding and maternal/paternal leave are critical. Paternal leave has been a controversial topic, and thus, Castillo-Angeles et al. sought to identify program directors’ perspectives on the issue [65]. They found that male residents tend to take shorter leaves than desired due to fear of stigma. Lactation support programs have been developed for surgeons as well [66]. Creating a formalized policy emphasized that wellness was a priority of postpartum residents by the chair and department. Greater strides should be taken to solidify these policies at a national level.
OpportunitiesThe Surgical Education Culture Optimization through targeted interventions based on National comparative Data (SECOND) Trial implores quality performance improvement methods in attempts to reduce trainee burnout and mistreatment [67]. There are 215 surgical residency programs enrolled currently in the trial. By interpreting ABSITE survey data from residents (individual), the SECOND trial principal investigators (PI’s) discuss feedback with each program (institutional) across the country (national). This is an ideal approach to integrate all three of the levels through one study. By identifying areas for improvement unique to each residency, a program personalized wellness toolkit is then created to guide recommendations.
It is suggested to offer rural and global rotations as part of the residency curriculum [68]. The thought is participation in humanitarian efforts rekindles the passion for a career in surgery. Additionally, the diversity of cases and commitment to communities may expand breadth of skills, facilitate interpersonal relationships and connections with patients, and overall strengthen one’s passion and commitment to surgery, thereby having positive effects on resilience.
Another important discussion is the opportunity to pursue other endeavors in research and professional development. More than one-third of surgical trainees pursue time off from clinical residency for these reasons. The motivation for going into lab years seems to be threefold: career planning, professional development, and personal rejuvenation [69]. The authors state “the need to take time off for more personal reasons, including burnout, was pervasive.” Another quote from the qualitative study of note was “I think it gives you time to really take back some of your time and take back some of your focus, and really put energy into the things that energize you and make you excited about choosing this career in the first place.” Seen as a positive in many aspects, it should be questioned why faculty are not easily offered similar opportunities for their personal growth and well-being.
LeadershipNational leaders emphasizing and modeling the importance of well-being in surgery are of utmost importance. Described best by Song et al. in their Journal of Surgical Education paper in 2020, there is a “general consensus that well-being initiatives would not be strictly enforced unless there was buy-in from leadership.” Having presidential speeches at large conferences highlighting the importance of adequately recognizing and addressing burnout. During the 2020 Association for Academic Surgery Presidential Address, a talk was given to this effect [70]. The address combined discussing aspects of the SECOND trial with giving general recommendations to stop “Fanning the Burnout Fire.” These include embracing change, appreciating trainees, stopping bullying, focusing on wellness, modeling excellent behavior, and giving feedback and mentorship.
Additionally, surgeons taking time to write opinion pieces about preventing burnout in surgery are necessary and beneficial to the cause. For instance in a piece called “Physician Heal Thyself” by a team at University of Michigan with the senior author being the section head of general surgery, they call for a dissolution of structural barriers as well as combating slow to change cultural factors [71]. A few examples given are eliminating guilt for prioritizing one’s own health, building a sense of community to be invested in co-worker’s health, and normalizing self-care.
Leaders throughout all fields of medicine have recognized the importance of support on the national level. One such example highlighting organizational involvement is the extensive list of resources created by the American Medical Association (AMA). Easily accessible on their website, the AMA offers an array of approaches to improve well-being in medical practices. One such example is the AMA STEPS Forward Program which details eight practice innovation topics from time-saving practices to behavioral health integration. There are webinars, videos, podcasts, toolkits, and more resources available to appeal to a wide audience. Though the AMA is not a surgeon-specific organization, their efforts are still applicable to general and trauma surgeons and imitable for a surgical society to construct surgery-specific resources and strategies [72].
留言 (0)