1. IntroductionThe devastating effects of the COVID-19 pandemic on global health have been widely described. Reduced access to care and essential health care disruptions secondary to outbreaks have disproportionately affected the most disadvantaged populations, increasing the burden of poverty related diseases [
1,
2,
3]. In 2021, the WHO registered for the first time in more than a decade, an increase in tuberculosis (TB) mortality [
1] and in the coming years, the drop in case detection and subsequent treatment would probably lead to an increase in transmission and a rise in the number of cases. In children, BCG vaccination has decreased by an estimated 5% and up to 63% of children and adolescents under 15 years of age did not receive TB treatment globally [
4]. The risk of TB progression is higher during childhood and adolescence, and failure to diagnose latent infection in these vulnerable populations may significantly increase the burden of disease.Spain is one of the European countries with the most confirmed cases of SARS-CoV-2, only surpassed by France, Germany, the United Kingdom and Italy; it ranks 12th of countries with the most cases in the world, despite its small geographical area [
5]. In Spain, the number of cases diagnosed with TB also decreased in the post-pandemic years. However, there has been an increase in cases with bilateral infiltrates probably caused by the delay in diagnosis [
6].Unaccompanied migrant minors (UM), children and adolescents that migrate without accompanying adults, represent one third of all asylum seekers in the European Union (EU) [
7]. In 2015, the numbers peaked in the EU, with 92,000 minors registered as asylum applicants. Since then, there has been a generalized decreasing trend. In 2020, despite the Coronavirus outbreak, the number of UM seeking asylum reached 13,600, which is only a 4% lower than in 2019 [
7]. This is a highly vulnerable population posing both legal and health care challenges [
8,
9,
10,
11,
12,
13] who concentrate in certain countries of the EU. Although Spain has not been traditionally among the preferred countries to request asylum—Germany, France or Italy were usually at the top of the list—the number of asylum seekers in Spain has grown progressively since 2015 in contrast with European statistics [
7]. During 2022, the effect of the pandemic was already unnoticeable in the country, accounting for over 11,000 first-time asylum seekers, representing 14.8% of the EU total. The instability in regions such as Venezuela and Colombia is probably one of the reasons that has caused the registered shifts, and owing to the language and the cultural and historical links between Spain and Latin America. Due to its position in the western Mediterranean migration route, Spain is also a hot spot for migrants from Sub-Saharan and Northern Africa [
12], the origin of many UM in the EU, right behind Afghanistan and Syria. The screening of imported diseases in UM is key to prevent transmission and long-term sequelae. However, there are many obstacles in their access to the health system (e.g., language and cultural differences, overcrowding and lack of resources in the refugee centers), which complicates their linkage to care and follow-up [
8,
14,
15,
16,
17,
18]. This is a concern, especially for the prevention of TB, which requires long treatments often not well tolerated, with frequent adherence issues.
The aim of this study is to describe the effect of the COVID pandemic on the screening of UM at a Reference Pediatric Tropical Unit in Madrid, Spain. We describe the prevalence of tuberculosis and other infectious diseases, the diagnostic performance of a tailored protocol for the screening of imported diseases and the longitudinal follow-up.
2. Methods 2.1. Study Design and Participants
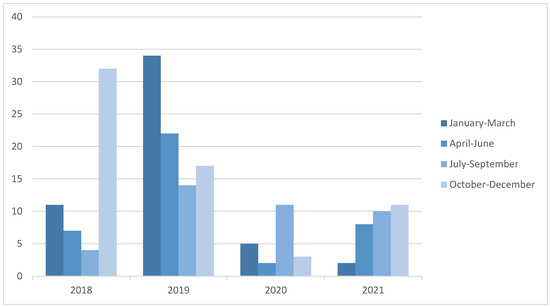
A retrospective, observational study was performed at a National Reference Unit for Pediatric Tropical Diseases in Spain. All UM below 18 years of age referred for health control from primary care, the emergency room and/or reception centers for asylum seekers and refugees between January 2018 and December 2021 were included. Medical records were reviewed. All patients were managed according to a unified protocol to screen for imported diseases. Blood tests (complete blood count, biochemistry including renal and liver function) and serology for helminths, congenital and vaccine-preventable diseases were conducted. Three fecal samples were collected for stool concentration microscopy.
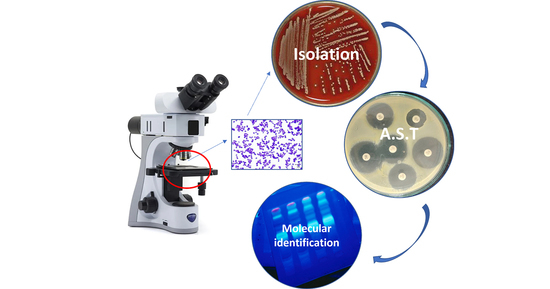
TB screening was carried out according to the protocol of the unit and the criteria of the clinician. Most PPD tests were performed in primary care centers before being referred to our unit, IGRAs were performed simultaneously or sequentially and in those with positive results, chest radiography was performed. In cases with suspected TB disease, samples of sputum and/or gastric aspirate were collected for culture and PCR.
The research was reviewed and approved by the Ethical and Research Committee of Hospital Universitario La Paz (PI-3348). Due to its retrospective nature, no informed consent was required.
2.2. Definitions
The pre-pandemic period included two years prior to the pandemic (2018, 2019) and January–February 2020, whereas the pandemic years included March 2020 to December 2021.
Parasitism was defined when at least one parasite (pathogenic or not) was identified. Co-parasitism was considered when at least two parasites were found. We subsequently analyzed pathogenic and nonpathogenic parasites. Pathogenic parasites considered all helminths and pathogenic protozoa: Giardia intestinalis, Cryptosporidium parvum and Entamoeba histolytica. Parasites with a controversial pathogenic effect were categorized with nonpathogenic parasites: Endolimax nana, Blastocystis sp., Entamoeba dispar/hystolitica when not differentiated, Entamoeba dispar, Entamoeba coli, Entamoeba hartmanni, Iodamoeba bütschlii and Dientamoeba fragilis [
19].Anemia was defined according to WHO as hemoglobin (Hb)
20]. Eosinophilia was defined when peripheral eosinophil count >500/microL [
21]; relative eosinophilia when an absolute eosinophil count 5% of circulating leukocytes [
18]. A peripheral leukocyte count above 11.000/mm3 defined leukocytosis [
22], whereas increased total serum immunoglobulin E (IgE) levels when >100 U/mL [
18]. Hypertransaminasemia was considered when AST > 50 U/L and/or ALT > 45 U/L [
23]. Hypercholesterolemia was defined as total cholesterol >200 mg/dL or LDL-cholesterol >130 mg/dL [
24].Body mass index (BMI) was automatically calculated and considered low below 18.5 kg/m2 and elevated when >25 kg/m2 [
25]. 2.3. Diagnosis
For the detection of parasites, both direct and indirect methods were used. Direct techniques consisted of the examination of three stool samples taken on alternate days. Firstly, the Mini Parasep® SF fecal parasite concentrator was used, and then optical microscopy looking for ova, cyst, larvae or parasites. Additionally, in patients coming from an endemic area and/or presenting with eosinophilia in which schistosomiasis was suspected, a urine sample for ova of Schistosoma was analyzed using Millipore Swinnex® membrane filter-holders (25 mm) and Whatman Nuclepore® membrane (10 μm). Indirect tools consisted of commercial serologic tests for Strongyloides (SciMedx microwell-ELISA®), Toxocara (NovaTec IgG-ELISA®) and Schistosoma (NovaTec IgG-ELISA®). ImmunoCAP Specific IgE-EIA tests (Thermo Fisher®) for Ascaris lumbricoides and Anisakis simplex were performed on an individual basis and usually on a second stage. Tuberculosis PCR was performed using GeneXpert® Ultra (Cepheid®). The cut-off was established by the manufacturing company.
2.4. Statistical Analysis
We used descriptive statistics to summarize demographic and clinical characteristics. Categorical variables were presented as absolute frequencies and percentages. Continuous variables were presented as the mean, with its standard deviation (SD). Categorical variables were compared using the Chi-square test, likelihood ratio test or Fisher’s Exact test, as appropriate. Continuous variables were compared by Student’s t-test or the Mann-Whitney–U test according to their distribution. A two-tailed p-value was set at 0.05 for all tests. All statistical analyses were performed using IBM-SPSS Statistics v.23.
4. DiscussionThe results of this study show the impact of the COVID-19 pandemic on access to health among UM arriving to the EU, with a 63% decrease in referrals. Two years after the first outbreak, the numbers have not recovered, whereas according to the official statistics, the rate of asylum seekers in the region has grown again. Latent tuberculosis infection was extremely frequent, with a comparable prevalence in the pre- and post-pandemic periods (69.3% vs. 82.7%; p = 0.087). However, in absolute numbers, there was a decrease by half in the number of cases. These findings are in line with the 2021 WHO Global Report [
26] that describes a drop in case notifications of new diagnosis worldwide [
27,
28]. The data, combined with the poor adherence and linkage to care observed, with 21% of patients not even starting treatment and around 40% of patients lost to follow-up over time, are extremely worrisome and endanger the control of transmission. Although those infected are usually asymptomatic, parasitosis was also common in this population, underlying the need for defining surveillance strategies, and optimizing screening and follow-up plans for this vulnerable population.
Imported diseases are a public health concern inherent to population movements. Infectious diseases such as TB or parasitosis are extremely linked to poverty and the social determinants of health, and often pauci are asymptomatic for long periods of time. Screening for imported diseases in asylum seekers and migrants is both an opportunity for early diagnosis and treatment that can avoid future sequelae and a public health need. However, the need to adjust diagnostic tests to symptoms and local epidemiology and the scarce evidence available limits our ability to standardized protocols. In the evaluation of UM, the epidemiology at origin needs to be supplemented with the potential risk exposure during the migration process, which is often extremely long and arduous. Still, cultural and language barriers often impair a proper anamnesis (as described in this series), and fear and the sense of helplessness are difficult to overcome. The benefits of tuberculosis screening might be clear, but the optimal test to use may vary according to availability. A PPD skin test is cheaper and accessible, but requires two visits, and it may be misinterpreted because of BCG vaccination among other factors. Interferon-Gamma Release Assays (IGRAs) are more accurate for screening but are expensive and usually not available in primary care centers. In our sample, PPD tests were done at arrival in primary attention centers, whereas IGRAs were done in the first visit to the hospital in selected cases (32 patients, 16%) to confirm diagnosis. Despite the advantage of not requiring a second visit for interpretation, some patients were lost to follow-up before the IGRA results were available.
Our results also suggest that parasitosis are frequent in this population, in line with previous studies [
10,
11,
14,
16]. Cost-effectiveness of the screening of parasitic infections is also controversial. Although the potential for overdiagnosis when using serology limits their usefulness according to some authors, others rely on the benefits of early treatment to prevent long-term sequelae [
14]. From our point of view, in the unique population of UM, overtreatment may be less harmful than an underdiagnosis, considering the long-term sequelae and scarce access to health care systems.
The optimal management of this population in terms of immunizations is also unclear. Vaccination cards are unavailable, and no information can be obtained from families in the specific case of UM. Serologies may help for adjusting the schedule, but the cost-effectiveness of this approach is questionable, and measurement of vaccine response is usually not available for many immunizations in routine clinical practices. To ensure protection is crucial, from both an individual but also from a public health perspective, as these children and adolescents may spend many months in institutions, often overcrowded, until their legal status is resolved. Protection against meningococcal disease, hepatitis, varicella, measles, rubella and mumps should be acquired as soon as possible. Our results demonstrate that vaccination coverage is good for most vaccine-preventable diseases, except for measles and hepatitis B. Performing serologies may help to adjust schedules, avoiding unnecessary shots and prioritizing the administration of meningococcal vaccines and a booster dose of HVB and measles. If administering a booster is enough or a full immunization is required should be addressed in further studies.
If improving diagnostic performance is important, ensuring treatment adherence and linkage to care in this population is an urgent need. In a highly transmissible disease such as TB, a lost-to-follow-up rate above 40% is unacceptable. The arrival of new, ultra-short regimens for TB treatment is encouraging, but ending global TB epidemics will require a specific effort in adolescents, with the design of targeted interventions and the development of multidiscipline units, including cultural and probably also peer support and all the innovative technologies available. Facilitating same day treatment initiation, a strategy that has demonstrated success in HIV treatment, should also be considered. In this study, 21% of patients had not even started treatment. Combined pills are important to increase adherence among adolescents, but are usually more expensive and supply shortages are not uncommon. The fact that all minors included in this study were, at least initially, in the institutional protection system is especially worrisome. A less hostile environment, specific training to overcome cultural barriers, together with translators and cultural mediators, need to be part of the attending teams, to ensure that all barriers are addressed. Although the high rate of patients diagnosed with parasitosis that never started treatment may be related to the complexity of acquiring certain antiparasitic drugs not available in Spain (accessible only via the pharmacy at the Ministry of Health), this is not the case for tuberculostatic drugs.
Our study has several limitations. The characteristics of our unit and references for tropical pediatric diseases limit our ability to generalize results, as many patients are referred because of symptoms and/or abnormal findings during health examinations at primary care or asylum seekers’ centers, including a positive PPD. This fact explains the higher prevalence of LTBI found compared to other studies [
1,
2,
3], and may have influenced the prevalence of certain parasitosis, as some patients were referred because of unexplained eosinophilia. The retrospective design impairs us from tailoring the study protocol, which did not contemplate the screening of other infections such us sexually transmitted diseases. With limited education and skills, unaccompanied children are extremely vulnerable socioeconomically, frequently exposing themselves to sexual and reproductive health risks [
29]. However, the evidence is surprisingly scarce, and there is controversy regarding the need for STD screening in this population. Further studies will be needed to answer these questions.


Comments (0)