
記住我

A total of 500 HCWs were enrolled in this study. The mean age of participants was 33.9 ± 7.9 years (range 20–73 years). About 70% were females. Among the female participants, 5.7% were pregnant. About 72% were married, 23% were single, and the remaining were divorced or widows. Furthermore, 45% had secondary school education, 21.4% had bachelor’s degrees, and 33.6% had postgraduate degrees.
Regarding occupation, more than half of the participants (51.2%) were nurses, 28.6% were physicians, 12.4% were pharmacists, and 7.8% were technicians. The highest percentage (57.2%) were working in Suez Canal University Hospitals, 24.8% were working in Ministry of Health-affiliated hospitals, and 18% were working in Suez Canal Authority-affiliated hospitals.
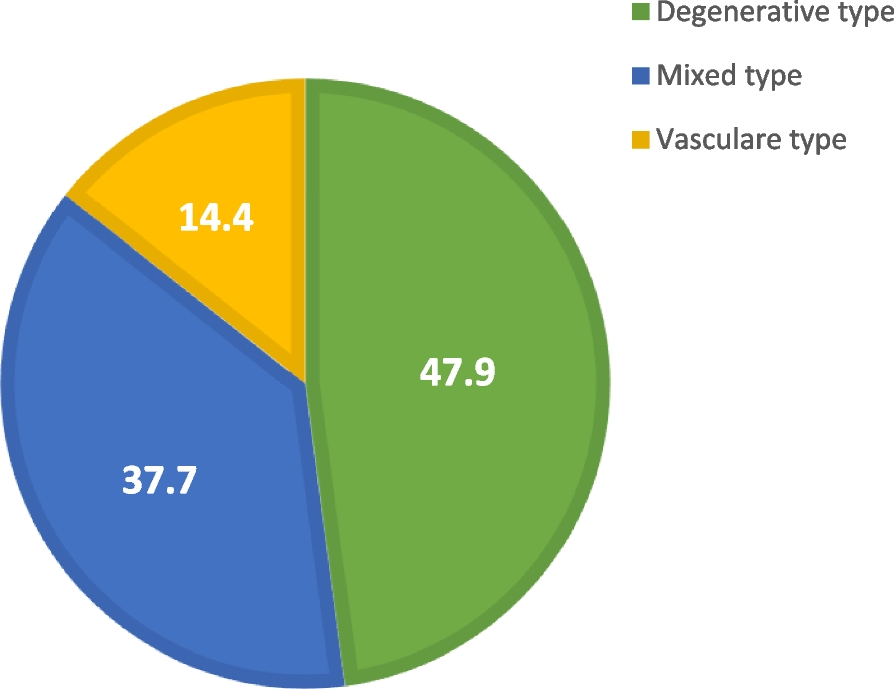
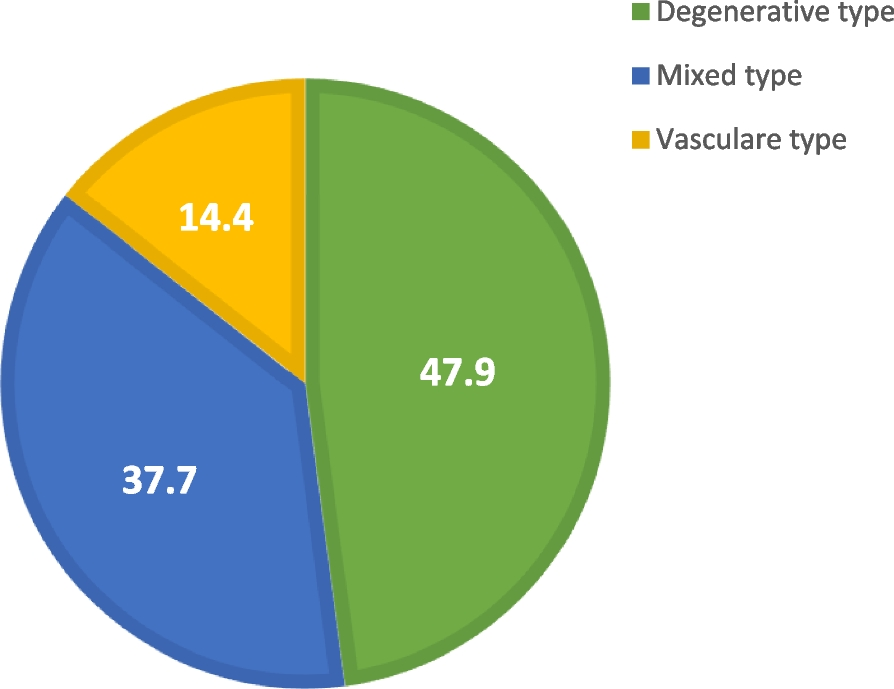
The participants’ history of COVID-19 infection was presented as a confirmed infection by polymerase chain reaction (PCR) or positive immunoglobulin M or immunoglobulin G test, confirmed symptoms or suspected symptoms, or never having an infection (Fig. 1). Additionally, 49% were not infected with COVID-19 before.
Fig. 1
COVID-19 infection history among participating healthcare workers from Ismailia, Egypt in the 1st half of 2021 (n = 500)
Participants were asked about their acceptance of vaccine uptake immediately, and their answers were ranked on a Likert scale (strongly agree, agree, do not know, disagree, and strongly disagree) (Fig. 2). Responses of strongly agree or agree were assigned as accepting (about 28% of participants), responses of strongly disagree or disagree were assigned as not accepting (49% of participants), and responses of do not know were assigned as hesitating (about 23% of participants).
Fig. 2
Vaccine acceptance levels among the participating healthcare workers from Ismailia, Egypt in the 1st half of 2021 (n = 500)
Table 1 shows the differences between the three groups regarding the different determinants. Males, those having children, physicians, and those working in Suez Canal Authority-affiliated hospitals showed higher frequencies of vaccine acceptance than others.
Table 1 Determinants and barriers of COVID-19 vaccine acceptance among healthcare workers in the studied hospitals according to the state of acceptance and hesitancy to take the vaccine during March and April 2021, Ismailia, EgyptThe most important determinants of vaccine hesitancy were female gender, being a nurse, secondary education level, and working in Suez Canal University Hospitals. The higher hesitancy rate was among those who thought that there was no sufficient evidence regarding vaccine safety and effectiveness (94.7%), the vaccine was not safe (91.3%), and the vaccine had serious side effects (75.6%).
Trust in governmental policies during the pandemic and trust in the healthcare facility they work in were the most frequent barriers to vaccine acceptance. More than two-thirds (67.8%) of the participants thought that medical mistakes are common, 8.6% thought that they are not, and 23.6% did not know. This reflects participants’ trust in health professionals, which is another barrier to vaccine acceptance.
Only 14% accepted the use of emergency law to vaccinate the public, and the remaining either refused or did not know.
Furthermore, two logistic regression models were used to determine the best predictor of vaccine acceptance among the participating HCWs. The first model included sociodemographic factors, previous intake of influenza vaccine, and trust in the healthcare facility they work in. The other model included knowledge and beliefs regarding the COVID-19 vaccine. Table 2 shows the two models. From the second model, vaccine safety was the best predictor with an odds ratio (OR) of 6.28 (95% CI 3.132–12.619, p < 0.001), followed by vaccine effectiveness (OR = 2.6, 95% CI 1.282–5.262, p = 0.008) and sufficient evidence regarding vaccine (OR = 2.5, 95% CI 1.154–5.508, p = 0.020). From the first model, the best predictor was the previous uptake of influenza vaccine (OR = 3.3, 95% CI 2.048–5.217, p < 0.001), followed by education level (OR 1.5, 95% CI 1.123–1.921, p = 0.005).
Table 2 Regression models for determinants of COVID-19 vaccine acceptance among HCWs recruited from the participating hospitals in Ismailia, Egypt, during March and April 2021The outcome variable is vaccine acceptance versus not accepting/hesitating. *Statistically significant at p < 0.05
Phase 2 of the studyThe analysis of the qualitative study showed a mixed view regarding the approach toward the COVID-19 vaccine. The findings were classified into two main themes: (1) impact of the available health information about COVID-19 vaccines, which included subthemes: confusion, distress, and mistrust, and (2) vaccine hesitancy and acceptance. The subthemes of confusion, distress, and mistrust were interconnected and overlapped. Generally, the more the confusion, distress, and mistrust felt by participants about the vaccine, the less likely they were willing to accept vaccination for themselves or for their family members.
Information and misinformation about the COVID-19 vaccineParticipants mentioned various sources of COVID-19 health-related information, such as TV and radio, the Internet including Google, social media such as YouTube and Facebook, and medical journals. Participants expressed mistrust in some traditional sources of news, which was more obvious for those who search for COVID-19-related news in other countries’ news or international scientific journals. This affected how people viewed their COVID-19 vaccination decision. Many participants decided to avoid watching the news about COVID-19, particularly when faced with contradictory information. A 42-year-old female nurse noted:
“Whenever I open my phone, I found a lot of information about COVID-19. This information comes from everyone not only from doctors or the Ministry of Health, but it comes from everybody. This makes me more worried about myself and my family.”
A 27-year-old physician noted, “From all this mess, I decided to ignore it all. I don’t read any health information about Corona from any source. Sometimes I do not believe what was said by the Ministry of Health.”
Misinformation about the vaccine, particularly passive information, has the potential to affect participants’ vaccination decisions. For instance, a female participant mentioned that she was keen to take the vaccine, and she changed her mind after listening to a story about people who were injected with the COVID-19 vaccine and developed serious side effects.
All participants expressed a desire to follow the hospitals’ rules and restrictions during the pandemic. However, they felt that the guidelines for HCWs' vaccination were confusing. Participants explained that the provided health information about the vaccination was poor, and the decisions contradicted their hospital’s policy for the availability of COVID-19 PCR testing. A 48-year-old female nurse noted:
“It is not understandable when you provide me with a free vaccine and at the same time you ask me to pay 1000 pounds for the test.”
In this theme, participants listed a range of misinformation they had encountered regarding COVID-19, resulting in confusion, distress, and mistrust. Participants agreed that providing them with trustworthy health information resources by the Suez Canal University Hospitals will promote their attitude toward COVID-19 vaccination acceptance.
Vaccine acceptance and hesitancyThis study showed a high level of vaccine hesitance among HCWs, particularly nurses. Of the 23 HCWs interviewed in this study, only 2 participants had their first dose of the vaccine, five had a mixed view with concerns about COVID-19 vaccine safety, and the remaining participants were unwilling to accept the COVID-19 vaccine.
The safety of the COVID-19 vaccine was a major concern for all participants. They questioned how quickly the vaccine had been produced and whether the side effects had enough time to be fully tested. These worries had been exacerbated by engagement with social media stories. A 29-year-old nurse preferred to wait for at least 6 months to test the effect of the vaccine on others before taking it. She noted:
“I’m not convinced yet that it is a good idea to take the vaccine. And if I take it, I will wait at least six months to see if there are any side effects happened to those who took it.”
Some concerns about the future effects of the vaccine on comorbid and immunocompromised patients were mentioned by many participants. A 31-year-old female nurse with a thyroid health problem noted:
“For me, I may think of taking the vaccine. But not now I want to be sure that there will be no future side effects that could happen to me.”
Participants, mostly physicians, agreed that the manufacturing of the COVID-19 vaccine is a fundamental method to control the pandemic. Therefore, they agreed to take any vaccine provided in the Suez Canal University Hospitals. The idea that the acceptability of the COVID-19 vaccine among physicians will impact the overall acceptability in the general population was agreed upon by all participants. Few participants showed confidence in any vaccine provided. They believed that when providing a vaccine in the market, people should have some confidence that it was a good vaccine and that it was quite safe.
A 26-year-old participant noted, “I believe they would never put the unsafe vaccine in the market, you know it is a great responsibility, and if you think it is not effective, it will not cause any harm.”
Vaccine hesitancy could be attributed to three prominent factors: safety concerns, negative stories, and personal knowledge. Vaccine acceptance was higher among physicians than among nurses. Vaccine safety and potential comorbidity side effects were the main concerns about vaccine acceptance among all participants.
留言 (0)