This study assessed the intention of Muslim pregnant women to fast during Ramadan. The use of the theory of planned behavior along with analytical tools including latent class analysis allowed for a better understanding of the complexity of the factors driving this intention, which appears to be guided by several factors including perceptions of physical ability, opinions of mothers, and husbands with perceptions of the impact on a woman’s health and Islam’s guidance.
One key finding that this study draws attention to is the fact that women who intend to fast all days of Ramadan are not a homogenous group. This group is divided into two distinct subgroups that differ in key variables such as the belief in the extent to which Islam encourages fasting. This appeared to be a strong and key variable for class 2 but a strong factor for class 1. This has implications for communication efforts targeting women in this group. Efforts should be made by clinicians and public health professionals to provide tailored communication messages for pregnant women intending to fast for the whole month of Ramadan that address the drivers behind their decisions starting with how women perceive Islam’s encouragement of their practice.
In this study, almost 58% of the participants had the intention to fast all days of Ramadan. This percentage is higher than what has been observed in other studies conducted in several Asian nations (Pakistan, Singapore, and Indonesia) where the rates of fasting ranged from 14 to 43% [6, 9, 24]. This difference may be partially explained by the conceptual difference between the intention to fast, measured in this study, and the actual fasting behavior, measured in other studies. The analytical model used in this study indicated that women’s belief in their physical ability to fast was very important in predicting the intention of the pregnant to fast during Ramadan. Findings concerning physical ability and fasting are in agreement with a study that was done in Iraq, another Arab country, where almost half of the participants, mentioned that being unable to fast was the most important reason behind not fasting [7]. Along the same lines, the perceived difficulty of fasting during pregnancy after feeling sick and weak was a major reason to skip or stop fasting among pregnant women [9, 25].
The belief of pregnant women that Islam encourages fasting during pregnancy was another influential predictor of the intention to fast. This belief has been explored by other studies where the proportion of women believing that fasting is encouraged by Islam ranged from 38 to 96% [3, 25, 26].
The opinion of the mothers of pregnant women was very important in the decision-making, where the majority of participants who intended to fast believed that their mothers would encourage fasting, and the majority of those not planning to fast mentioned that their mothers would discourage fasting. This is in line with other studies, not related to fasting, that addressed the impact mothers have on their pregnant daughters’ health-related decisions. For example, in a study done in Ghana that assessed the behavior of pregnant teenagers for health-seeking information, mothers were the most important source of information for their pregnant daughters [27]. This might be particularly relevant to the Lebanese cultural context, which emphasizes strong intergenerational family relationships. It may be that the mother is the closest natural and trustworthy “expert” the pregnant woman can access. Perhaps slightly less important, but still an important factor was the husband’s opinion concerning fasting. In this study, 45% of the women intending to fast perceived the opinions of their husbands to be important in guiding their decisions. A study done in Pakistan observed that family members’ opinions on encouraging fasting were particularly trusted by the pregnant participants [3]. Moreover, in Singapore, Joosoph et al. found that the majority of family members and husbands supported the pregnant women and encouraged them to fast [24].
Interestingly, Muslim sheiks were not observed to be contributing to the intention of pregnant women to fast. This is in contrast with a study done in the US state of Michigan, a multicultural setting, where Muslim sheiks influenced pregnant women’s decisions to fast more than family members [5]. The difference might be explained by a sociocultural effect where the difference in cultural context plays a role. Muslims in Muslim minority countries, such as the USA, usually have a sense of community revolving around scheduled gatherings in Mosques, where they can discuss Islamic teachings with religious figures. This would lead to women placing a particular value on sheiks in that setting. Lebanon, on the other hand, is a country with a significant Muslim population where the role of religious figures in this particular issue does not seem to be as prominent.
Health care professionals and, predominantly, the obstetrician or the midwife represent reliable and frequently encountered sources of information to which pregnant women address their health needs and concerns [28]. In this study, however, it was interesting that the obstetrician was not contributing to the intention of pregnant women to fast either directly or indirectly. Communication gaps between health professionals and pregnant women concerning fasting were observed in prior studies, which indicated varying rates of counseling about the issue [5, 25, 29]. In a study done in Pakistan, the majority of participants did not even consult any health professional to assess the safety of fasting during Ramadan [3]. On the other hand, the majority of pregnant women in a study done in Iran consulted their midwife or obstetrician about fasting during Ramadan [4]. Somewhere in between, approximately half of the fasting women in a study done in Germany consulted their obstetricians to discuss fasting status. Several reasons may contribute to the communication gaps described above [25]. Those variations might be related to the fear of pregnant women from discussing this religious issue with their caregivers, and their perceptions that they should be making this decision independently of their providers, as they fear the judgment of their behavior from their providers [3, 4].
Moreover, variation in the rates of consulting obstetricians indicates that primary care providers, pharmacists, and nurses should be proactive in providing pregnant Muslim women with sound advice on fasting as well as encourage them to seek professional help from their obstetricians when fasting during Ramadan is being considered.
4.1 Limitations of the study
As with all studies, this research had both strengths and weaknesses. The study was conducted in Lebanon, a country with a diverse cultural background. The instrument was provided to participants in their native language improving the comprehension of questionnaire items and ultimately improving the quality of data. Theory informed a priori hypotheses that drove the analyses.
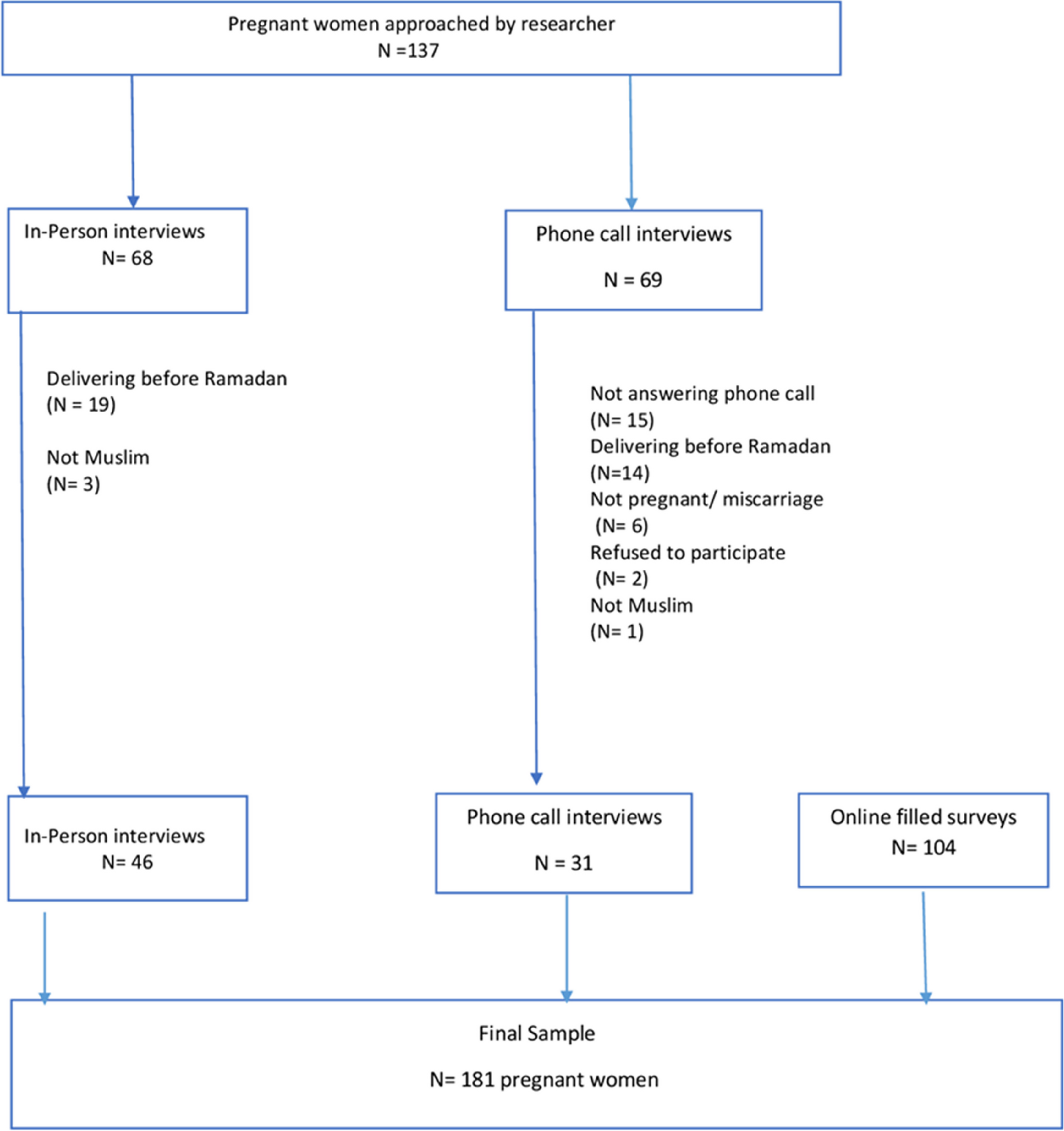
Limitations of this project merit discussion. The diversity in the convenience sampling procedure, including online recruitment of pregnant women, resulted in a higher average educational level of participants limiting the generalizability of the study. The study was done in Lebanon, a country with unique diversity. While this represents an addition to the literature, caution should be taken before generalizing to other settings in which Muslims represent an overwhelming majority or minority. The effect of some confounders on the intention to fast cannot be ruled out including the effect of fasting in a previous pregnancy, or if some pregnant women are also breastfeeding. Self-report measures are more likely to result in the overestimation of intention to fast during Ramadan, a socially desirable behavior, that may be seen as an indication of religious piety by some participants. Still, in an attempt to reduce this bias, the survey was self-administered in the online data collection phase, and no identifying information was collected from participants. Mode of administration bias should be considered when participants in the phases involving face-to-face and telephone interviews may be more likely to report fasting. Finally, this study focused on intentions to fast rather than actual fasting, which might change over time with women who initially chose to fast reverse their decision or vice versa.





Comments (0)