
Remember me
Breast cancer is the most common type of cancer in women.1-3 According to the American Cancer Society, the onset of the malignancy occurs in the cellular lining of the ducts and lobules of the glandular tissue of the breast (i.e. in situ), which later metastasizes to the nearby lymph nodes.2-4 Recent epidemiological studies show that breast cancer accounts for almost 25% of all cancers.5 According to the World Health Organization, almost 685,000 women die of breast cancer annually worldwide.2
Typically, endocrine therapies including tamoxifen and aromatase inhibitors are employed as a mainstay treatment for patients with breast cancer.6, 7 Tamoxifen functions primarily by competing with 17-β estradiol at the receptor area while also promoting the role of 17-β estradiol in breast cancer development.8, 9 Recent studies show that tamoxifen specifically binds to the DNA after its metabolic activation and initiates carcinogenesis.9 It was also shown to have chemopreventive properties, and the ability to transiently reduce serum lipid levels in postmenopausal women.10, 11 Aromatase inhibitor agents (i.e. anastrozole, exemestane, letrozole) are reported to act primarily by binding irreversibly (type I steroidal drugs) and reversibly (type II steroidal drugs) to the aromatase enzyme that transforms androgens in estrogen.12 Although the efficacy of both of these endocrine therapies has been widely documented in the literature,13-18 recent evidence has raised concerns regarding their implementation especially given an alarming increase in the cardiovascular morbidity associated with these drugs.19-21 Studies have attributed the onset of this adverse effect to the hormonal suppression induced by the drugs that eventually promotes the onset of a range of cardiovascular myopathies such as venous thromboembolism, heart failure, arrhythmia, angina, myocardial infarction, and stroke.22, 23 However, despite surplus evidence little is known about the differences in the safety profiles of these drugs to prevent cardiovascular disease in patients with breast cancer.
To date, a few individual randomized controlled trials,24-28 and cohort studies,20, 29-36 have attempted to compare the incidence of cardiovascular adverse events outcomes between breast cancer patients receiving tamoxifen and aromatase inhibitors with inconclusive results. While some studies had reported a relative increase in the events of venous thromboembolism with the administration of tamoxifen as compared to direct aromatase inhibitors,24, 27, 28, 36 others had reported a higher incidence of venous thromboembolism in patients consuming aromatase inhibitors as compared to tamoxifen.20, 30, 37 Similarly, a lack of consensus exists regarding the comparative influence of aromatase inhibitors and tamoxifen on the outcomes of heart failure and myocardial infarction. While some studies had reported an increase in the overall incidence of myocardial infarction and heart failure in patients receiving aromatase inhibitors as compared to tamoxifen,20, 26, 27, 33, 34 others have reported the opposite effect.32, 38
To the best of our knowledge, only two systematic reviews have attempted to comparatively evaluate the cardiovascular adverse outcomes between breast cancer patients consuming aromatase inhibitors and tamoxifen.39, 40 Nevertheless, the findings of these reviews are limited as they failed to include a range of recently published high quality randomized controlled trials,28 and cohort trials.20, 31-34, 36, 37 In this present systematic review and meta-analysis, we will attempt to bridge the gap in the current state of evidence by evaluating the comparative cardiovascular outcomes in breast cancer patients consuming aromatase inhibitors and tamoxifen. The findings from this study may contribute to developing best practice guidelines for oncologists to lower the incidence of cardiovascular adverse outcomes in breast cancer patients.
2 METHODSWe followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines41 for conducting this systematic review and meta-analysis (Figure 1).

Illustrating the PRISMA flowchart
2.1 Data search strategy The literature search was performed across five scientific databases (Web of Science, MEDLINE, CENTRAL, EMBASE, and Scopus) from inception till July 2021 using a combination of the following MeSH keywords: “Breast cancer”, “tamoxifen”, “aromatase inhibitors”, ‘cardiovascular complications’, “venous thromboembolism”, “cardiac arrest”, ‘heart failure’, ‘angina’, ‘stroke’, ‘arrhythmia’, ‘myocardial infarction’, and “arrhythmia”. Bibliography section of the included studies was also manually screened to find additional relevant studies. The inclusion criteria were as follows: Studies comparing cardiovascular outcomes between breast cancer patients consuming tamoxifen and aromatase inhibitors. Studies evaluating the events of venous thromboembolism, heart failure, angina, myocardial infarction, arrhythmia, and stroke. Human studies. Randomized controlled trials controlled clinical trials, case-control studies, prospective trials, or retrospective cohort trials. Studies published in peer-reviewed scientific journals. Studies published in English.The studies were independently screened by two different reviewers. Cases of disagreement were resolved by discussion with a third independent reviewer.
2.2 Quality assessmentRisk of bias for the included randomized controlled studies was assessed using Cochrane's risk of bias assessment tool for randomized controlled trials.42 This tool evaluates the outcomes for selective reporting, confounding bias, measurement of outcomes, and incomplete data availability as threats that can instigate instigating. Risk of bias for the included cohort studies was performed using Newcastle Ottawa scale,43 a tool that evaluates the outcomes for selective reporting, confounding bias, measurement of outcomes, and incomplete data availability as threats that can instigate instigating. Methodological quality was apprized independently by two reviewers, and cases of disagreement were resolved by discussion with a third reviewer.
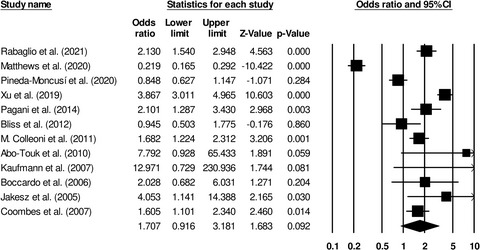
2.3 Data analysisA within-group meta-analysis was conducted using CMA, Comprehensive Meta-analysis version 2.0,44 based on the random-effects model.45 The odds ratio was computed to quantify the comparable risks between breast cancer patients receiving tamoxifen and aromatase inhibitors. Heterogeneity between the studies was assessed by I2 statistics, with I2 statistics between 0%–25% considered indicative of negligible heterogeneity, 25%–75% of moderate heterogeneity, and ≥75% of substantial heterogeneity.46 Publication bias was evaluated by Duval and Tweedy's trim and fill procedure47 that imputates of studies from either side of the plotted graph to identify any unbiased effect. The significance level for this study was determined at 5%.
3 RESULTSA search across five academic databases resulted in a total of 980 studies. Additional 13 studies were identified during the screening of the reference sections of the retrieved studies. A total of 20 studies met the inclusion criteria. Six of the included studies were randomized controlled trials,24-28, 48 13 were prospective cohort studies,20, 29-37, 49-51 and one was a retrospective cohort study.38 The data is summarized in Table 1.
TABLE 1. Demonstrates the details of the included studies Study Country Type of study Sample descriptive Age (M ± SD years) Stage of breast cancer Follow-up Venous thromboembolism Stroke Arrhythmia Angina Myocardial infarction Heart failure Franchi et al. (2021) Italy Prospective cohort studyTamoxifen: 7937
AI: 26,009
— — — —Tamoxifen: 163
AI: 182
— —Tamoxifen: 92
AI: 89
Tamoxifen: 243
AI: 266
Rabaglio et al. (2021) Switzerland Randomized controlled trialTamoxifen: 1541
AI: 1535
— — 3.8 yearsTamoxifen: 117
AI: 57
Tamoxifen: 24
AI: 22
— — —Tamoxifen: 26
AI: 26
A. A. Matthews et al. (2020) UK Prospective cohort studyTamoxifen: 4716
AI: 5289
Tamoxifen: 68
AI: 70
I to III 1 yearTamoxifen: 58
AI: 284
Tamoxifen: 190
AI: 1126
Tamoxifen: 222
AI: 1640
Tamoxifen: 87
AI: 710
Tamoxifen: 38
AI: 407
Tamoxifen: 233
AI: 1368
Khosrow-Khavar, Filion, et al. (2020) Canada Prospective cohort studyTamoxifen: 9783
AI: 8139
Tamoxifen: 66.2 ± 11.5
AI: 70.8 ± 11.2
— 1.3 years —Tamoxifen: 59
AI: 86
— —Tamoxifen: 34
AI: 61
Tamoxifen: 33
AI: 83
Pineda-Moncusí et al. (2020) UK Prospective cohort studyTamoxifen: 3082
AI: 18,455
Tamoxifen: 69
AI: 67
— —Tamoxifen: 49
AI: 345
Tamoxifen: 1
AI: 11
— — — — Choi et al. (2020) South Korea Prospective cohort studyTamoxifen: 7081
AI: 19,584
Tamoxifen: 63.8 ± 7.2
AI: 63.3 ± 6.6
— 5 years —Tamoxifen: 230
AI: 700
— — — — Khosrow-Khavar, Bouganim, et al. (2020) Canada Prospective cohort studyTamoxifen: 3874
AI: 1962
Tamoxifen: 67.7 ± 11.1
AI: 68.2 ± 10.7
— — —Tamoxifen: 22
AI: 19
— —Tamoxifen: 14
AI: 18
Tamoxifen: 14
AI: 13
Xu et al. (2019) USA Prospective cohort studyTamoxifen: 4062
AI: 3837
— 0 to IV 5.4 yearsTamoxifen: 309
AI: 80
— — — — — Abdel-Qadir et al. (2016) Canada Prospective cohort studyTamoxifen: 1941
AI: 7409
Tamoxifen: 74
AI: 71
I to III 3.2 years — — — —Tamoxifen: 17
AI: 106
— Haque et al. (2016) USA Retrospective cohort studyTamoxifen: 4207
AI: 3807
— — 4.5 years —Tamoxifen: 204
AI: 53
—Tamoxifen: 279
AI: 71
Tamoxifen: 106
AI: 35
Tamoxifen: 248
AI: 69
Seruga et al. (2014) Canada Prospective cohort studyTamoxifen: 41
AI: 33
Tamoxifen: 69
AI: 69
— — — — —Tamoxifen: 7
AI: 5
Tamoxifen: 9
AI: 6
— Pagani et al. (2014) Belgium Prospective cohort studyTamoxifen: 2325
AI: 2318
— I to III —Tamoxifen: 50
AI: 24
Tamoxifen: 32
AI: 20
— — — — Bliss et al. (2012) Australia Prospective cohort studyTamoxifen: 2305
AI: 2294
— — 7.5 yearsTamoxifen: 19
AI: 20
— —Tamoxifen: 79
AI: 110
— — Colleoni et al. (2011) Italy Randomized controlled trialTamoxifen: 2459
AI: 2463
— — 3.7 yearsTamoxifen: 104
AI: 63
Tamoxifen: 45
AI: 38
— — —Tamoxifen: 25
AI: 30
Abo-Touk et al. (2010) Egypt Randomized controlled trialTamoxifen: 60
AI: 60
— I to III 3.4 yearsTamoxifen: 7
AI: 1
Tamoxifen: 1
AI: 2
— — — — JF et al. (2008) UK Prospective cohort studyTamoxifen: 3116
AI: 3125
— — 8.3 years —Tamoxifen: 34
AI: 20
— —Tamoxifen: 33
AI: 34
— Kaufmann et al. (2007) Germany Prospective cohort studyTamoxifen: 452
AI: 445
Tamoxifen: 60.5
AI: 60.9
I to III 4.83 yearsTamoxifen: 6
AI: 0
Tamoxifen: 1
AI: 3
— — — — Boccardo et al. (2006) Italy Randomized controlled trialTamoxifen: 225
AI: 223
— I to III 5.3 yearsTamoxifen: 10
AI: 5
— — — — — Jakesz et al. (2005) Austria Randomized controlled trialTamoxifen: 1606
AI: 1618
— I to III —Tamoxifen: 12
AI: 3
— — —Tamoxifen: 2
AI: 3
— Coombes et al. (2007) UK Randomized controlled trialTamoxifen: 2372
AI: 2352
— I to III 4.6 yearsTamoxifen: 72
AI: 45
— — —Tamoxifen: 19
AI: 31
— Abbreviations: AI, Aromatase inhibitors; M, Mean; SD, Standard deviation. 3.1 Participant informationTwenty included studies reported data on 174,142 female breast cancer patients. Of them, 63,185 patients received tamoxifen, and 110,957 patients received aromatase inhibitors.
The average age of the participants was as 67.4 ± 3.8 years; the average age of patients receiving tamoxifen was 67.2 ± 3.9 years and the average age of patients receiving aromatase inhibitors was 67.5 ± 3.6 years. Twelve studies did not report the age of the patients.24-28, 30, 32, 36, 38, 48, 49, 51
3.2 Quality assessment for randomized controlled trials studiesRisk of bias in the methodology of the randomized controlled trials was assessed using Cochrane's risk of bias assessment tool for randomized controlled trials (Table 1). The overall risk was found to be low in the included studies. Most of the bias in the included studies was detected in allocation of concealment, blinding of outcome assessment, and other biases. The overall risk of bias is summarized in Figure 2.

Demonstrates the risk of bias according to Cochrane's risk of bias assessment tool for randomized controlled trials
3.3 Quality assessment for cohort studiesRisk of bias in the methodology of the cohort studies was analysed with the Newcastle Ottawa scale (Tables 2 and 3). The overall risk was found to be low in all the included studies. The overall risk of bias is summarized in Figure 3.
TABLE 2. Demonstrates the risk of bias according to Cochrane's risk of bias assessment tool for randomized controlled trials (+: No bias, −: Bias present, ?: Unclear) Study Random sequence generation Allocation concealment Selective reporting Other bias Blinding of participants & personnel Blinding of outcome assessment Incomplete outcome data Rabaglio et al. (2021) + + + ? + + + Abo-Touk et al. (2010) + + + ? + + + Boccardo et al. (2006) + ? + − + ? + Jakesz et al. (2005) + + + + + + + Coombes et al. (2007) + + + ? + + + Coombes et al. (2007) + + + ? + + + TABLE 3. Risk of bias for i
Comments (0)