
Remember me
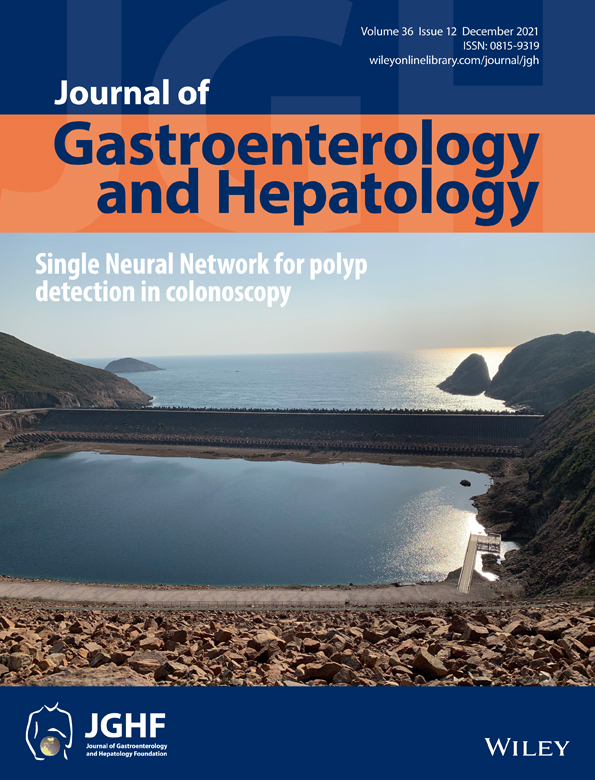
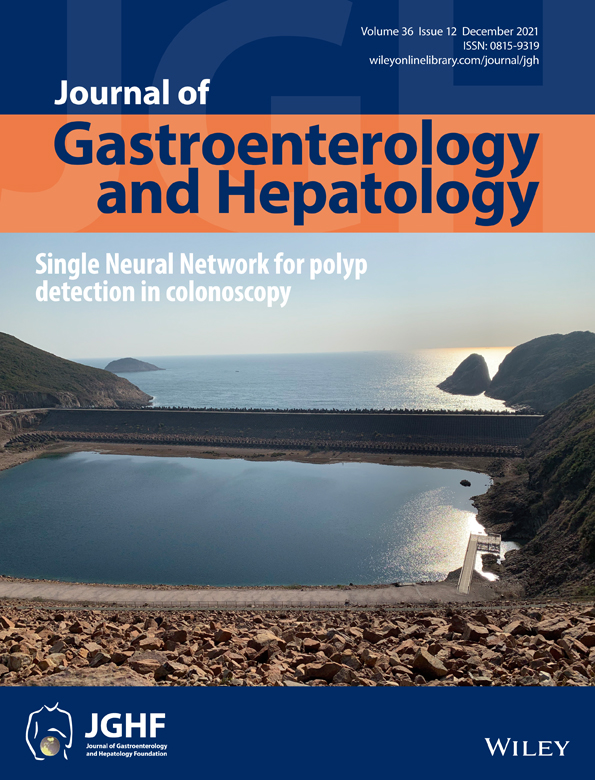
A 39-year-old man was admitted to the gastroenterology department with the chief complaint of fever and backache. Pancreatic duct stones and cholecystitis were confirmed by abdominal computed tomography (CT) and magnetic resonance imaging (MRCP) (Fig. 1). Pancreatic duct stones were successfully removed during endoscopic retrograde cholangiopancreatography (ERCP, Fig 2). However, an interesting scene happened when the contrast agent was injected into the pancreatic duct. A congenital traffic branch formed above the head of the pancreas connects the bile duct and pancreatic duct (Fig. 2). The contrast agent flows from the pancreatic duct into the bile duct and the guide wires can enter the bile duct from the pancreatic duct (Video S1).
 MRCP of the pancreatico-biliary tract, showing stones in the main PD adjacent to the ampula (blue arrow) with a traffic branch (red arrow) connecting the major papilla to the mid-CBD. Otherwise, the main CBD (black arrow) and PD (yellow arrow) were normal in calibre. [Color figure can be viewed at wileyonlinelibrary.com]
MRCP of the pancreatico-biliary tract, showing stones in the main PD adjacent to the ampula (blue arrow) with a traffic branch (red arrow) connecting the major papilla to the mid-CBD. Otherwise, the main CBD (black arrow) and PD (yellow arrow) were normal in calibre. [Color figure can be viewed at wileyonlinelibrary.com]
 ERCP images that demonstrated the main pancreatic ductal calculi (blue arrow, a) and the traffic branch that connect the major papilla to the mid-CBD (yellow arrows, a-d). The close loop communication between the PD and CBD was outlined by both contrast and guidewire canulation (c). [Color figure can be viewed at wileyonlinelibrary.com]
ERCP images that demonstrated the main pancreatic ductal calculi (blue arrow, a) and the traffic branch that connect the major papilla to the mid-CBD (yellow arrows, a-d). The close loop communication between the PD and CBD was outlined by both contrast and guidewire canulation (c). [Color figure can be viewed at wileyonlinelibrary.com]
Pancreaticobiliary maljunction (PBM) is a congenital malformation in which the confluence of the bile duct and the pancreatic duct was situated outside the duodenal wall. PBM was acknowledged as a risk factor for the development of biliary cancer. Pancreatic juice could reflux to the bile duct and gallbladder in PBM, which could induce histological changes in the biliary epithelial tissue, such as epithelial cell proliferation and intraepithelial neoplasia, eventually resulting in biliary malignant tumors. PBM was divided into two types based on whether there is bile duct dilation, PBM with biliary dilation (congenital biliary dilation) and PBM without biliary dilation. Based on the data from recent literature, the incidence of biliary cancer in adult patients with PBM with biliary dilation and PBM without biliary dilation was 22% and 42%, respectively. With respect to the location of biliary cancers, bile duct cancer and gallbladder cancer occurred in 32% and 63% of PBM patients with biliary dilation, respectively. Unlike PBM with biliary dilation, biliary cancers with PBM without biliary dilation occurred mainly in the gallbladder (88%) and rarely in the bile duct (7%). Cholecystectomy and resection of the extrahepatic bile duct is an established standard surgical treatment for the PBM with biliary dilation. However, no consensus has been reached on whether the extrahepatic bile duct was excised in PBM without biliary dilation. Prophylactic cholecystectomy has been performed in many medical centers because most biliary cancers associated with PBM without biliary dilation are gallbladder cancer. However, some surgeons suggest that both gallbladder and the extrahepatic bile duct should be excised in PBM without biliary dilatation because the incidence of bile duct cancer in PBM without biliary dilatation is higher compared with the general population.
In this case, the confluence of the bile duct and the pancreatic duct was located at the duodenal papilla, which is different from PBM. To the best of our knowledge, this congenital malformation type was reported for the first time.
Comments (0)