
Remember me


Cervical cancer is the fourth most common malignancy among women, in the light of a report using the GLOBOCAN 2018 database, there were 569,847 new cases of cervical cancer among 311,365 deaths globally in 2018.1 Persistent human papillomavirus (HPV) infection, especially high-risk HPV (HR-HPV), is a major cause of precancerous lesions and cervical cancer.2 It has been estimated that more than 50–80% of sexually active women will be infected with one or more types of genital HPV in their lifetime.3 The emergence and application of HPV preventive vaccines have been recognized as a major advancement and the most effective intervention for the control of cervical lesions.4
Presently, 9-valent vaccine covering HPV6/11/16/18/31/33/45/52/58 has been used in China. VIVIANE, FUTURE III, and other studies have confirmed the preventive effect of HPV vaccine on cervical cancer,5-7 and the number of deaths among vaccinated women might be reduced by >4 million over the next decade.8 However, the 9-valent vaccines do not encompass all HR-HPVs, which might cause cervical lesions, and the distribution of HPV genotypes varies between regions and countries, leading to geographical-based changes in the incidence and mortality of cervical cancer.9, 10 Previous VIVIANE studies (bivalent vaccine) and FUTURE III studies (tetravalent vaccine) have not found the protective effect of the vaccine on cervical intraepithelial neoplasia (CIN) 2+ lesions.5, 7 A recent meta-analysis showed that in the post-vaccine era, the infection rate of some non-vaccine coverage types also increased significantly.11 In addition, the female vaccination coverage must be at least 50% to have a protective effect on unvaccinated population.12 Therefore, the existing multivalent HPV vaccines cannot completely prevent cervical cancer. The majority of studies have focused on cervical cancer screening and vaccine effectiveness, whereas few studies analyzed the infection rate and prevalence of non-9-valent vaccine covered HPV subtypes, as well as the clinical characteristics and risk factors of non-9-valent vaccine covered HPV- infected patients.
In this retrospective study, we studied the non-9-valent vaccine covered HPV subtypes in cervical lesions, analyzed their distribution and the clinical characteristics of these HPV-infected patients. We also identified the most non-9-valent vaccine covered carcinogenic HPV types and the risk factors of CIN patients.
2 MATERIAL AND METHODS 2.1 Patient samplesThe clinical data of 7400 patients treated at the Department of Gynecology of Shanghai General Hospital from January 2017 to February 2021 were analyzed in this retrospective study. All cases provided cervical histopathological results and pre-treatment HPV typing results. According to the inclusion or exclusion criteria, 2670 patients with non-9-valent vaccines covered HPV subtype infections were selected for analysis. The patients were divided into normal group (2179 cases), CIN1 group (338 cases), and ≥CIN2 (including CIN2 and CIN3 and carcinoma in situ) group (153 cases). The HPV typing data, histopathological data, and age were collected from each group.
The inclusion criteria were as follows: (1) cervical HPV and cytology sampling qualified; (2) colposcopy was performed in the gynecological clinic of our hospital; (3) HPV classification, ThinPrep cytologic test (TCT), Pathological results of colposcopy biopsy, and baseline data were obtained. Exclusion criteria were as follows: (1) previous hysterectomy or conization; (2) women infected with any type of the 9-valent vaccine covered HPV; (3) other malignant tumors.
2.2 HPV detection and typing methodsThe PCR-reverse dot-hybridization technology was used for HPV detection using a PCR-RDB HPV genotyping assay (Yaneng Bioscience Co., Ltd., China),13 it can detect a total of 23 HPV types, including 17 HR-HPV subtypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82), 6 LR-HPV subtypes (6, 11, 42, 43, 81, and 83). Among these subtypes, 14 types were non-9-valent vaccine covered HPV subtypes (35, 39, 51, 53, 56, 59, 66, 68, 73, 82, 42, 43, 81, 83). Follow the kit instructions for experimental operation and data analysis.
2.3 TCT detectionCytological classification of the samples was performed by two experienced pathologists based on the Bethesda System Standard 2001 in a double-blinded manner.
2.4 Colposcopy and pathological examinationThe diagnosis of cervical diseases in all patients was based on cervical histopathology. The cervical tissue is obtained from colposcopy biopsy or surgical submission specimens. The histopathological results of the highest level of the cervix were viewed as the final diagnosis of the disease. The specimens were processed using the standard histopathological methods and evaluated by at least two pathologists. All colposcopy operations were performed by qualified colposcopy specialists at our Center. The pathology results were classified as normal, CIN1, CIN2, CIN3, and carcinoma in situ.
2.5 Statistical analysisThe clinical characteristics and multiple HPV infections of the patients were tested by chi-square test. For samples with multiple HPV infections, the infection of one HPV subtype contributed to the occurrence of the disease as a partial attribution. The prevalence rate of HPV genotypes and the attribution rate of cervical lesions are based on the literature,14 the “attributive factor” of a certain HPV subtype is calculated by the formula “the number of cases of a single HPV subtype infection in the disease/the number of cases of any HPV subtype single infection.” Thus, the attribution rate of a specific HPV subtype of the disease is as follows: (the number of single infections of HPV subtype + multiple infections of an HPV subtype × attribution factor)/the total number of cases of the disease. The correlation between HPV subtypes and cervical diseases was analyzed by binary logistic regression, and 95% is considered the confidence interval. A p < 0.05 indicate a statistical difference significantly. All statistical analyses were performed using software package of social science statistical software version 26 (SPSS, IBM Co., Armonk, NY, USA).
3 RESULTS 3.1 Analysis of clinical characteristics of patients infected with non-9-valent vaccine covered HPV subtypesAmong the three groups of patients infected with non-9-valent vaccine covered HPV subtypes, CIN1 group had the highest median age (48 years), and ≥CIN2 group had the highest number of pregnancies and parities, with an average of 2.99 and 1.52, respectively. The univariate analysis was used to compare the clinical variables. Compared to the normal group, age ≥50 years, pregnancy ≥5 times, parity ≥3 times, menopause, no condom use, cervical transformation zone type III, and HPV-negative were risk factors for CIN1 or ≥CIN2 (p < 0.05) (Table 1).
TABLE 1. Clinical characteristics of patients with non-9-valent vaccine covered HPV infection Variables Normal (n = 2179) CIN1 (n = 338) p Normal (n = 2179) ≥CIN2 (n = 153) p n (%) n (%) n (%) n (%) Age Median (years) 40 48 40 43 <50 1691 (78) 181 (54) <0.0001 1691 (78) 106 (69) 0.018 ≥50 488 (22) 157 (46) 488 (22) 47 (31) Pregnancy Mean (times) 2.48 2.65 2.48 2.99 <5 1990 (91) 298 (88) 0.06 1990 (91) 128 (84) 0.001 ≥5 189 (9) 40 (12) 189 (9) 25 (16) Parity Mean (times) 1.20 1.34 1.20 1.52 <3 2064 (95) 307 (91) 0.004 2064 (95) 138 (90) 0.018 ≥3 115 (5) 31 (9) 115 (5) 15 (10) Condom Yes 631 (29) 70 (21) 0.002 631 (29) 30 (20) 0.013 No 1548 (71) 268 (79) 1548 (71) 123 (80) Menopause Yes 383 (18) 138 (41) <0.0001 383 (18) 54 (35) <0.001 No 1796 (82) 200 (59) 1796 (82) 99 (65) Cervical transformation area Type I 254 (12) 18 (5) <0.0001 254 (12) 9 (6) <0.001 Type II 781 (36) 72 (21) 781 (35) 33 (22) Type III 1144 (52) 248 (74) 1144 (53) 111 (72) HPV Positive 1705 (78) 238 (70) 0.001 1705 (78) 100 (65) <0.001 Negative 474 (22) 100 (30) 474 (22) 53 (35) 3.2 Analysis of infection in single- and multi-non-9-valent vaccine covered HPV subtypesAmong 14 non-9-valent vaccine covered HPV subtypes, the infection rates of HPV53, 56, 51, and 68 were higher in this study: 17.6%, 13.2%, 12.6%, and 9.3%, respectively. At the same time, the infection rate of HPV81 was high (4.23%) in polymorphic infections. In CIN1 group, the infection rates of HPV53, 56 and 51 were higher: 14.3%, 14.2%, and 12.4%, respectively. However, among the patients with multi-type HPV infection, the infection rates of HPV35 and 81 were second only to HPV53, accounting for 4.14%. In patients with ≥CIN2, the infection rates of HPV56 (13.1%), 51 (11.8%) and 53 (10.5) were higher, and the subtypes with high monotype HPV infection rates were 51 (8.5%), 68 (5.2%), and 53 and 56 (4.6%). However, in polymorphic infections, the infection rate of HPV35 and 39 was higher than that of HPV53 (Table 2).
TABLE 2. Analysis of infection in single- and multi-type non-9-valent vaccine covered HPV subtypes HPV types Normal (n = 2179) CIN1 (n = 338) ≥CIN2 (n = 153) TotalPositive
n (%a)
Single type
n (%a)
Multiple infections
n (%a)
Positive
n (%a)
Single type
n (%a)
Multiple infections
n (%a)
Positive
n (%a)
Single type
n (%a)
Multiple infections
n (%a)
Positive
n (%a)
Single type
n (%a)
Multiple infections
n (%a)
HPV35 94 (4.3) 52 (2.4) 42 (1.9) 30 (8.9) 16 (4.7) 14 (4.1) 15 (9.8) 4 (2.6) 11 (7.2) 139 (5.2) 72 (2.7) 67 (2.5) HPV39 190 (8.7) 116 (5.3) 74 (3.4) 21 (6.2) 9 (2.7) 12 (3.6) 13 (8.5) 2 (1.3) 11 (7.2) 224 (8.4) 127 (4.8) 97 (3.6) HPV42 120 (5.5) 43 (2.0) 77 (3.5) 13 (3.9) 3 (0.9) 10 (3.0) 10 (6.5) 3 (2.0) 7 (4.6) 143 (5.4) 49 (1.8) 94 (3.5) HPV43 109 (5.0) 42 (1.9) 67 (3.1) 10 (3.0) 0 (0.0) 10 (3.0) 5 (3.3) 1 (0.7) 4 (2.6) 124 (4.6) 43 (1.6) 81 (3.0) HPV51 275 (12.6) 167 (7.7) 108 (5.0) 42 (12.4) 30 (8.9) 12 (3.6) 18 (11.8) 13 (8.5) 5 (3.3) 335 (12.6) 210 (7.9) 125 (4.7) HPV53 405 (18.6) 274 (12.6) 131 (6.0) 50 (14.8) 31 (9.2) 19 (5.6) 16 (10.5) 7 (4.6) 9 (5.9) 471 (17.6) 312 (11.7) 159 (6.0) HPV56 283 (13.0) 180 (8.3) 103 (4.7) 48 (14.2) 18 (5.3) 30 (8.9) 20 (13.1) 7 (4.6) 13 (8.5) 351 (13.2) 205 (7.7) 146 (5.5) HPV59 160 (7.3) 80 (3.7) 80 (3.7) 24 (7.1) 14 (4.1) 10 (3.0) 7 (4.6) 4 (2.6) 3 (2.0) 191 (7.2) 98 (3.7) 93 (3.5) HPV66 173 (7.9) 105 (4.8) 68 (3.1) 27 (8.0) 14 (4.1) 13 (3.9) 7 (4.6) 2 (1.3) 5 (3.3) 207 (7.8) 121 (4.5) 86 (3.2) HPV68 202 (9.3) 123 (5.6) 79 (3.6) 30 (8.9) 17 (5.0) 13 (3.9) 15 (9.8) 8 (5.2) 7 (4.6) 247 (9.3) 148 (5.5) 99 (3.7) HPV73 44 (2.0) 18 (0.8) 26 (1.2) 7 (2.1) 3 (0.9) 4 (1.2) 3 (2.0) 1 (0.7) 2 (1.3) 54 (2.0) 22 (0.8) 32 (1.2) HPV81 162 (7.4) 72 (3.3) 90 (4.1) 21 (6.2) 7 (2.1) 14 (4.1) 12 (7.8) 3 (2.0) 9 (5.9) 195 (7.3) 82 (3.1) 113 (4.2) HPV82 26 (1.2) 12 (0.6) 14 (0.6) 8 (2.4) 2 (0.6) 6 (1.8) 6 (3.9) 3 (2.0) 3 (2.0) 40 (1.5) 17 (0.6) 23 (0.9) HPV83 11 (0.5) 2 (0.1) 9 (0.4) 3 (0.9) 1 (0.3) 2 (0.6) 2 (1.3) 0 (0.0) 2 (1.3) 16 (0.6) 3 (0.1) 13 (0.5)Additionally, among all patients, the infection rates of HPV53, HPV51, HPV56, and HPV39 were 10.1%, 7.5%, 6.1%, and 4.4%, respectively. The higher infection rates of single HPV were 53, 51, 56, and 68. In the multi-type HPV infection, the infection rate of HPV42 was next to that of HPV51, that is, 3.04% (Table S1).
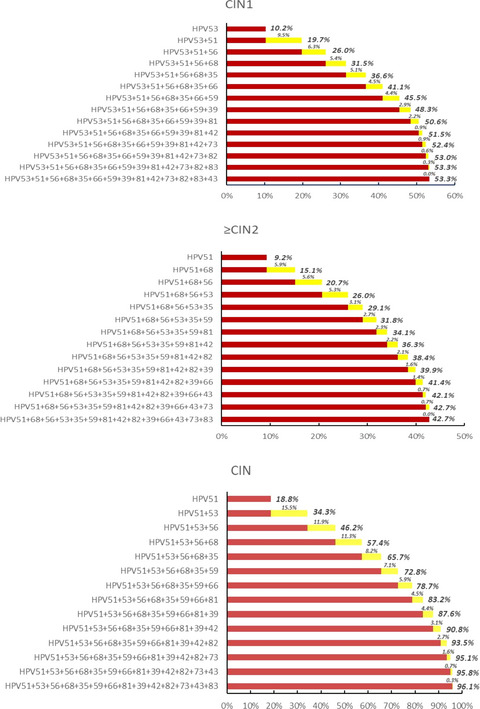
3.3 Cumulative attribution rate of 14 non-9-valent vaccine covered HPV subtypes in cervical lesionsIn our cohort, the current non-9-valent vaccine covered HPV subtypes could be attributed to 53.3% of CIN1 and 42.7% of ≥CIN2. The CIN1 grade is mainly attributed to the HPV53 (10.2%), followed by HPV51 (9.5%) and 56 (6.2%). The ≥CIN2 grade is mainly attributed to HPV51 (9.2%), followed by HPV68 (5.9%) and 56 (5.6%). Among all CINs, the attribution rates of HPV51, 53, and 56 were 18.8%, 34.3%, and 46.2%, respectively. Meanwhile, HPV51, 53, 56, and 68 accounted for the majority of cervical lesions in each group, and the cumulative attribution rates were 31.5% in CIN1 and 26.0% in ≥CIN2 (Figure 1).

Cumulative attribution rate of 14 non-9-valent vaccine covered HPV subtypes in cervical lesions
3.4 Distribution of multiple infection rates of non-9-valent vaccine covered HPV subtypesIn all patients infected with non-9-valent vaccine covered HPV subtypes, one, two, three, four subtypes, high-risk non-9-valent vaccine covered, and low-risk non-9-valent vaccine covered subtypes were detected with infection rates of 56.5%, 15.2%, 3.8%, 1.01%, 59.2%, and 43.9%, respectively. The rate of monotype infection was the highest in the normal group (59.0%) and lowest in ≥CIN2 group (37.9%). The infection rate of two subtypes of HPV increased with the aggravation of cervical lesions, and the infection rate of patients with ≥CIN2 was the highest (22.9%), while triple and quadruple infections were most common in the CIN1 group with infection rates of 5.0% and 1.2%, respectively. Furthermore, the infection rate of HPV subtypes covered by high-risk non-9-valent vaccine was higher than that covered by low-risk non-9-valent vaccine among all three groups of patients. Conversely, the infection rate of HPV subtypes covered by low-risk non-9-valent vaccine decreased gradually. Consecutively, two subtypes of HPV infections were found to be risk factors for ≥CIN2 compared to the normal and CIN1 groups (normal, p = 0.001; CIN1, p = 0.034). Compared to the normal group, the HPV infection covered by high-risk non-9-valent vaccine was a risk factor for ≥CIN2 (p = 0.027) (Table 3).
TABLE 3. Distribution of multiple infection rates of non-9-valent vaccine covered HPV subtypes HPV type Normal (n = 2179) CIN1 (n = 338) ≥CIN2 (n = 153) Total n (%) n (%) n (%) n (%) Single type 1286 (59.0) 165 (48.8) 58 (37.9)a 1509 (56.5) Two types 320 (14.7) 52 (15.4) 35 (22.9)b 407 (15.2) Three types 77 (3.5) 17 (5.0) 6 (3.9)c 100 (3.8) Four types 22 (1.0) 4 (1.2) 1 (0.7)d 27 (1.0) N9-HR-HPV 1274 (58.5) 210 (62.1) 97 (63.4)e 1581 (59.2) N9-LR-HPV 980 (45.0) 124 (36.7) 52 (34.0)f 1156 (43.3) Abbreviations: N9-HR-HPV, high-risk HPV covered by non-9-valent vaccines, including HPV35/39/51/53/56/59/66/68/73/82; N9-LR-HPV, low-risk HPV covered by non-9-valent vaccines, including HPV42/43/81/83. 3.5 Correlation between HPV subtype infection, clinical factors, and cervical lesionsThen, we analyzed the clinical risk factors of non-9-valent vaccines covered HPV-infected CIN patients through single-factor and multi-factor. Multivariate analysis showed that HPV35, HPV53, HPV81, HPV83, menopause, and cervical transformation area were independent risk factors for CIN compared to the normal group (OR > 1, p < 0.05). Cervical transformation zone was an also critical risk factor (OR = 4.1). In patients with TCT ≥ atypical squamous cells of unknown significance (ASC-US), HPV35, HPV42, HPV83, age, menopause, and cervical transformation zone were independent risk factors for CIN (Table 4
Comments (0)