
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Remember me
Since 2020, there have been outbreaks of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection worldwide. SARS-CoV-2 infection is severe in patients with lung cancer.1-4 Steroids, antiviral drugs, anti-interleukin-6 drugs, etc. are currently used for treating SARS-CoV-2. However, there has been no silver bullet breakthrough as yet. The effectiveness of treatment that prevents aggravation, such as antibody cocktail therapy5 and new antiviral drugs,6 has been reported. The usefulness of the messenger RNA (mRNA) vaccine has already been reported7, 8 and BNT162b2 and mRNA-1273 are typical SARS-CoV-2 mRNA vaccines currently is used worldwide. Vaccination is recommended for patients with cancer by the Center for Disease Control and Prevention and National Comprehensive Cancer Network.9, 10 However, few data are available to establish vaccine safety and efficacy in patients with advanced cancer. The SARS-CoV-2 vaccine has a high incidence of side effects such as fever even in healthy individuals, but there are few serious adverse events. In the BNT162b2 phase 3 trial, only approximately 4% of enrolled patients had a malignancy of any type, and these patients were not analyzed separately to assess vaccine efficacy.7 In the mRNA-1273 trial, patients with cancer were not enrolled.8 There are reports that the antibody titer after vaccination does not change between patients with cancer and healthy people,11-13 while others have reported that antibody titers after mRNA vaccination are low in patients with solid cancer receiving anticancer drug treatment.14, 15 The SARS-CoV-2 vaccine has a high incidence of side effects such as fever even in healthy individuals. However, there are few serious adverse events.7, 8 The side effects of the vaccine in patients with chronic inflammatory diseases who are receiving immunosuppressive treatment are the same as those of healthy individuals.16 Although some reports have been published on the safety of SARS-CoV-2 mRNA vaccines in patients with cancer and it has been reported that there is no problem with safety,17 there are also case reports of cytokine release syndrome.18
Therefore, this study aimed to evaluate the safety of the vaccine in patients with lung cancer receiving anticancer drug therapy.
METHODS Ethics statementsAll participants provided written informed consent. This study was approved by the relevant institutional review board (National Hospital Organization Iwakuni Clinical Center Institutional Review Board, Iwakuni, Yamaguchi, Japan) (no. 0262) and was conducted in compliance with the Declaration of Helsinki and Ethical Guidelines for Medical and Health Research Involving Human Subjects. The study protocol was registered on the website of the University Hospital Medical Information Network, Japan (protocol ID: UMIN000043918).
Study design and participantsThis multicenter prospective observational study, the OLCSG2102 study, included patients with advanced lung cancer who were receiving anticancer therapies such as chemotherapy, immune checkpoint inhibitors (ICIs), and molecular targeted therapy. Patients who met the following eligibility criteria were enrolled at seven hospitals in Japan. They included those aged 20 years or older, diagnosed with unresectable cancer or recurrent lung cancer, receiving anticancer drug therapy, and scheduled for SARS-CoV-2 vaccination. Patients with a history of coronavirus disease (COVID-19), patients with a history of SARS-CoV-2 vaccination, patients who were considered inappropriate for SARS-CoV-2 vaccination, or patients with an estimated prognosis of <2 months were excluded.
OutcomesThe coprimary outcomes were to assess the frequency of fever and other side reactions 7 days after the second dose of SARS-CoV-2 vaccination based on a patient-reported survey,
secondary outcomes of the frequency of fever and other side reactions 7 days after the first dose of SARS-CoV-2 vaccination based on the patient-reported survey, incidence of grade 3 or worse immune-related adverse events after SARS-CoV-2 vaccination in patients receiving ICIs, incidence of COVID-19 after vaccination, overall survival after vaccination, and progression-free survival of anticancer drug therapy. Body temperature of the axilla was measured in degrees Celsius.
Data collectionThe side reaction rating scale for the vaccine was based on the BNT162b2 report.7 Data on local and systematic reactions and use of medication were collected from patients who had been surveyed for 7 days after each vaccination. Pain at the injection site was assessed according to the following scale: mild, does not interfere with activity; moderate, interferes with activity; severe, prevents daily activity; and grade 4, emergency department visit or hospitalization. Redness and swelling were measured according to the following scale: mild, 2.0–5.0 cm in diameter; moderate, >5.0–10.0 cm in diameter; severe, >10.0 cm in diameter; and grade 4, necrosis or exfoliative dermatitis (for redness) and necrosis (for swelling). The scales of systematic events were as follows: fatigue, headache, chills, muscle pain, joint pain (mild, does not interfere with activity; moderate, some interference with activity; or severe, prevents daily activity), vomiting (mild, 1–2 times in 24 h; moderate, >2 times in 24 h; or severe, requires intravenous hydration), and diarrhea (mild, 2–3 loose stools in 24 h; moderate, 4–5 loose stools in 24 h; or severe, ≥6 loose stools in 24 h). Grade 4 for all events indicated an emergency department visit or hospitalization. Vaccine adverse reactions were reported daily by the patients on a predistributed questionnaire. Patients measured and recorded body temperature daily for 8 days from the day before vaccination to the seventh day after vaccination.
Statistical analysesData from the BNT162b2 clinical trial showed that the frequency of fever >38°C after the second vaccination was 11% in the setting of patients aged 56 years or older.7 We assumed that a 10% increase in the frequency of fever >38°C in patients who were undergoing treatment for lung cancer would be acceptable. Accordingly, we estimated that the required number of patients for the early safety assessment would be 104, with a one-sided significance level of 0.05 and a power of 80%. An interim analysis was conducted when 120 cases were collected considering that 5% of cases would drop out of the survey.
Differences were assessed using analysis of variance or chi-square test. Adjusted odds ratios were calculated using multivariate logistic regression analyses with the following covariates: sex, age, smoking history, the presence of respiratory complications, and type of treatment. All statistical analyses were performed using a standard software package (STATA version 17; StataCorp). The significance threshold was set at p < 0.05 for the two-sided unpaired tests.
RESULTSWe report the results of the interim analysis of early adverse events owing to vaccination. Between April 8, 2021 and August 31, 2021, >400 patients undergoing lung cancer treatment were enrolled to assess vaccination safety and immune-related adverse events. At the time of obtaining the patient-reported survey from 120 patients to assess post-vaccination safety, the initial adverse events of vaccination were analyzed. All patients received two doses of the vaccination.
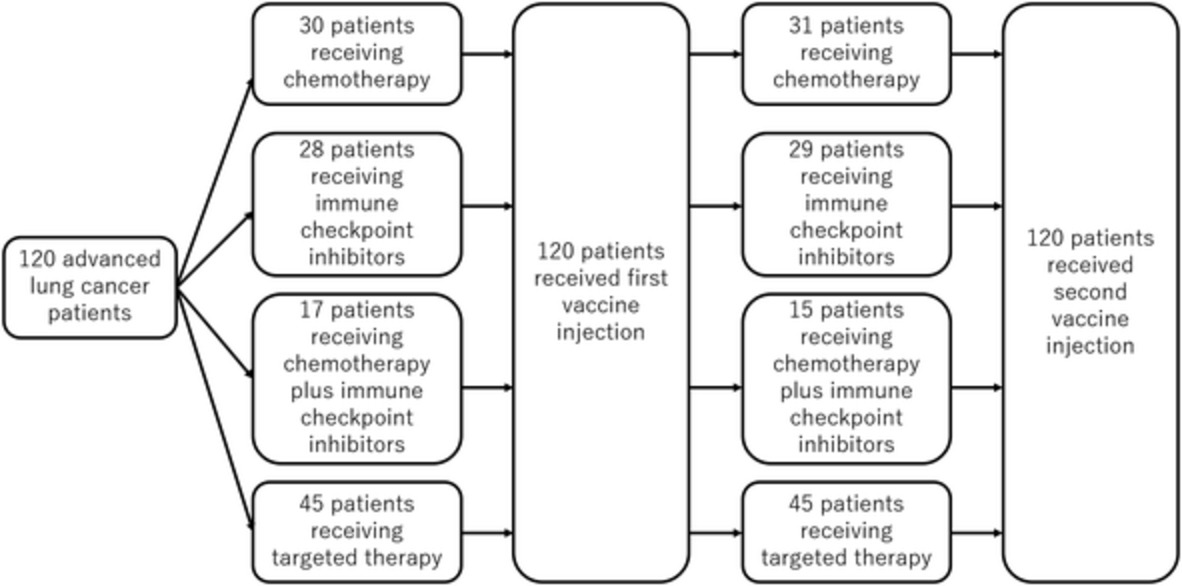
Patient characteristics of the initial 120 patients are presented in Table 1. The patients comprised 73 men (61%) and 47 women (39%). The median age was 73.5 years (range, 64–86 years), and 41% of patients were 75 years or older. There were 74 (62%) smokers. All patients had advanced lung cancer, and the histological subtypes were mostly adenocarcinoma (n = 94). The treatments received for lung cancer at the time of the first vaccine injection were chemotherapy in 30 patients, ICIs in 28 patients, combination of chemotherapy and ICIs in 17 patients, and targeted therapies such as tyrosine kinase inhibitors in 45 patients. Two patients changed their treatment regimens between the first and second injections. Both patients were treated with a combination of chemotherapy and ICIs, and one patient's treatment was changed to chemotherapy alone and the other to ICI alone. In this study, 115 of the 120 patients received the BNT162b2 vaccine (Table 1).
TABLE 1. Patient characteristics Characteristic No. % Total 120 100 Age (years) Median (range) 73.5 (64–86) Sex Male/female 73/47 61/39 ECOG-PS 0/1/2 43/75/2 36/63/2 Smoking status Never smoked/smokers 46/74 38/62 Histology Ad/Sq/NOS/SCLC 94/15/3/8 78/13/3/7 Vaccine BNT162b2/mRNA-1273/unknown 115/1/4 96/1/3 Treatment (first vaccine injection) Chemotherapy 30 25 ICI 28 23 Chemotherapy plus ICI 17 14 Targeted therapy 45 38 Treatment (second vaccine injection) Chemotherapy 31 26 ICI 29 24 Chemotherapy plus ICI 15 13 Targeted therapy 45 38 Abbreviations: Ad, adenocarcinoma; ECOG-PS, Eastern Cooperative Oncology Group Performance Status; ICI, immune checkpoint inhibitor; mRNA, messenger RNA; no., number; NOS, not otherwise specified; SCLC, small cell lung cancer; Sq, squamous cell carcinoma.Systemic reactions to the first and second injections are shown in Figure S1 and Figure 1, respectively. The frequency of fever >38°C after the first injection was 2.5%, and the frequency of fever >38°C after the second injection, the primary outcome, was 15.4% (95% confidence interval [CI]: 9.4%–23.2%). The frequency of fever for each treatment regimen is shown in Table 2. Fever after the second injection tended to be slightly more frequent with chemotherapy regimens and less frequent with targeted therapy. The most frequent systemic reactions after the second injection were myalgia (54.2%) and fatigue (49.2%), and there was no difference according to treatment regimens. The local reactions after the first and second inoculations are shown in Figure S2 and Figure 2, respectively. After the second injection, 46.7% of patients had pain at the injection site. However, there was no difference between the treatments. In total, no serious adverse events were observed in this study, and there were no cases in which the treatment schedule was postponed owing to adverse events of the vaccine.

Systemic reactions reported after the second vaccine injection by treatment regimen. ICI, immune checkpoint inhibitor; Chemo, chemotherapy
TABLE 2. Frequency of fever after the second vaccine injection according to treatment regimen Treatment regimen Frequency 95% CI Chemotherapy (N = 30a) 23.3% 9.9%–42.3% ICI (N = 29) 13.8% 3.9%–31.7% Chemotherapy plus ICI (N = 15) 26.7% 7.8%–55.1% Targeted therapy (N = 43*) 7.0% 1.5%–19.1% Abbreviations: CI, confidence interval; ICI, immune checkpoint inhibitor.
Local reactions reported after the second vaccine injection by treatment regimen. ICI, immune checkpoint inhibitor; Chemo, chemotherapy
Patients receiving anticancer therapy, except targeted therapy, had the date of vaccine injection determined by their physician. There was little association between the period between anticancer drug administration and vaccination and adverse events, especially fever (Table S1). In addition, medications such as steroids and antipyretics, as well as adverse events such as fever had negligible effect on the results (Table S2). Univariate and multivariate analyses were performed to investigate the effects of fever. The frequency of fever was significantly higher in men than in women (adjusted odds ratio: 8.87; 95% CI: 1.25–62.8; p = 0.029). There was no difference in the frequency of fever between patients older and younger than 75 years (adjusted odds ratio: 1.73; 95% CI: 0.55–4.47; p = 0.350) (Table S3). Patients treated with cytotoxic anticancer drugs tended to have a high fever, and patients who received targeted therapy tended to have a lower frequency of fever, although the difference was not significant (Table 2, A.3).
DISCUSSIONIn the present study, the frequency of fever >38°C after the second injection, the primary outcome, was 15.4%. Compared with the findings in previous reports,7 the present findings suggested a higher risk in patients with lung cancer who are, or will be, receiving anticancer medicine than in healthy individuals. However, regarding other adverse events, many patients had muscle pain, although the degree was mild; in addition, other adverse events were similar to those reported in the BNT162b2 phase 3 trial,7 and the frequency of antipyretic use was also low (Figures 1 and S1). As a local reaction, pain was observed in many patients, but redness and swelling were less, and local pain tended to be less than the data reported in the BNT162b2 phase 3 trial (Figures 2 and S2).7 Although the frequency of fever after vaccination tends to be high, it is considered that the SARS-CoV-2 mRNA vaccine could be safely administered to patients with lung cancer.
Previous studies have reported that the side effects of the vaccine are low in patients undergoing cancer treatment.13 However, we obtained different results in our study. This may be because of differences in the methods of data collection or between races.
In our study, men tended to have fever more frequently than did women. A study by Menni et al. evaluated the safety and efficacy of the BNT162b2 and ChAdOx1 COVID-19 vaccines in the UK and reported that women tended to have more adverse events than did men.19 The higher frequency of fever in men may be related to the fact that men had a higher frequency of a smoking history than,women, and smokers tend to have more fever than non-smokers. Furthermore, because of the higher smoking rate among men than among women, the proportion of patients receiving targeted therapy was low, and the proportion of those receiving chemotherapy was high. Although adverse events tended to be more frequent in the chemotherapy group than in the nonchemotherapy group, the number of cases remains small at this time, and more data need to be collected to determine whether chemotherapy treatment will truly increase adverse events related to the vaccine. Patients who received chemotherapy tended to have more fever than those without chemotherapy, and none of them developed febrile neutropenia. The reason patients who received chemotherapy tended to have higher temperatures is unclear. Drug-induced fever from anticancer drugs may have affected patients who were receiving chemotherapy. Currently, we are further accumulating cases, and we plan to verify our findings after the number of cases increases.
Our study has several limitations. First, our study included patients who had been using corticosteroids or antipyretic analgesics for treating lung cancer and complications prior to vaccination (Table S2). In these patients, preused drugs may have helped reduce adverse events. In addition, some patients had symptoms owing to lung cancer before vaccination, such as fatigue or any pain (Figures S3 and S4), and it is possible that the adverse events of the vaccine were overestimated in such patients. Second, our study could not determine whether the antibody titer increased; thus, the effectiveness of the vaccine could not be evaluated. Finally, since the main purpose of this report was to evaluate the short-term safety of the COVID-19 vaccine in those receiving lung cancer treatment, we could not examine its long-term safety. Serious complications (stroke and myocardial infarction) and adverse events of immunotherapy have been the focus of recent attention20, 21 and will be examined in a number of cases during an observation period. At this time, our study is considered to be the result of ensuring the safety of vaccination in patients with lung cancer.
In conclusion, vaccine-related adverse events tend to increase in patients with lung cancer undergoing cytotoxic chemotherapy. However, serious adverse events in the short-term are comparable to those observed in healthy individuals. This cohort study provided data on the safety of using the mRNA vaccine for SARS-CoV-2 in patients with advanced lung cancer who are receiving anticancer therapies such as chemotherapy, ICIs, and targeted therapy.
ACKNOWLEDGMENTSThe authors thank all the investigators at the participating institutions. All authors contributed to the coordination of this study at each hospital. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
CONFLICT OF INTERESTToshio Kubo received lecture fees from Chugai pharmaceutical. Shoichi Kuyama received lecture fees from Chugai pharmaceutical. Yoshinobu Maeda received honoraria from Kyowa Kirin Co. Ltd., Bristol-Myers Squibb Company, Chugai Pharma Co. Ltd., Pfizer Co. Ltd., Celgene Co. Ltd., Novartis Pharmaceutical Co. Ltd., and Takeda Pharmaceutical Co. Ltd., and research funding from Astellas Pharma Inc., Bristol-Myers Squibb Company, Takeda Pharma Co. Ltd., Kyowa Kirin Co. Ltd., Nippon Shinyaku Co. Ltd and Chugai Pharma Co. Ltd. Katsuyuki Kiura received honoraria from MSD K.K., research funding from Pfizer Japan Inc., SHIONOGI & Co. Ltd., Boehringer Ingelheim Co. Ltd., Nippon Kayaku Co. Ltd., Taiho Pharmaceutical Co., Ltd., Ono Pharmaceutical Co. Ltd., MSD K.K., Chugai Pharmaceutical Co. Ltd., Bristol-Myers Squibb K.K., Takeda Pharmaceutical Co. Ltd., and fees for consulting from Daiichi Sankyo Co. Ltd. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this study.
Filename Description tca14281-sup-0001-FigureS1.jpgJPEG image, 118.6 KBFigure S1. Systemic reactions reported after the first vaccine injection by treatment regimen
ICI, immune checkpoint inhibitor; Chemo, chemotherapy
tca14281-sup-0002-FigureS2.jpgJPEG image, 61.9 KBFigure S2. Local reactions reported after the first vaccine injection by treatment regimen
ICI, immune checkpoint inhibitor; Chemo, chemotherapy
tca14281-sup-0003-FigureS3.jpgJPEG image, 74.1 KBFigure S3. Changes in systemic reactions before and after the first vaccine injection
Pre, preoperatively; Post, postoperatively
tca14281-sup-0004-FigureS4.jpgJPEG image, 77.6 KBFigure S4. Changes in systemic reactions before and after the second vaccine injection
Pre, preoperatively; Post, postoperatively
tca14281-sup-0005-Tables.docxWord 2007 document , 20.4 KBTable S1. Duration of anticancer drugs administered before vaccine injection
Table S2. Frequency of medication use that affected the outcomes
Table S3. Odds ratio for fever of ≥38°C associated with the second vaccine injection
Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
REFERENCES
1Luo J, Rizvi H, Preeshagul IR, Egger JV, Hoyos D, Bandlamudi C, et al. COVID-19 in patients with lung cancer. Ann Oncol. 2020; 31: 1386– 96. https://doi.org/10.1016/j.annonc.2020.06.007 2Peravali M, Joshi I, Ahn J, Kim C. A systematic review and meta-analysis of clinical characteristics and outcomes in patients with lung cancer with coronavirus disease 2019. JTO Clin Res Rep. 2021; 2:100141. https://doi.org/10.1016/j.jtocrr.2020.100141 3Tagliamento M, Agostinetto E, Bruzzone M, Ceppi M, Saini KS, de Azambuja E, et al. Mortality in adult patients with solid or hematological malignancies and SARS-CoV-2 infection with a specific focus on lung and breast cancers: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2021; 163:103365. https://doi.org/10.1016/j.critrevonc.2021.103365 4Provencio M, Mazarico Gallego JM, Calles A, Antoñanzas M, Pangua C, Mielgo Rubio X, et al. Lung cancer patients with COVID-19 in Spain: GRAVID study. Lung Cancer. 2021; 157: 109– 15. https://doi.org/10.1016/j.lungcan.2021.05.014 5Baum A, Fulton BO, Wloga E, Copin R, Pascal KE, Russo V, et al. Antibody cocktail to SARS-CoV-2 spike protein prevents rapid mutational escape seen with individual antibodies. Science. 2020; 369: 1014– 8. 6Singh AK, Singh A, Singh R, Misra A. Molnupiravir in COVID-19: a systematic review of literature. Diabetes Metab Syndr. 2021; 15:102329. 7Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020; 383: 2603– 15. https://doi.org/10.1056/nejmoa2034577 8Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med. 2021; 384: 403– 16. 9 Centers for Disease Control and Prevention, Updated Healthcare Infection Prevention and Control Recommendations in Response to COVID-19 Vaccination. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-after-vaccination.html. Accessed September 13, 2021. 10 COVID-19 resources available from the National Comprehensive Cancer Network. https://www.nccn.org/covid-19/default.aspx. Accessed September 13, 2021. 11Thakkar A, Gonzalez-Lugo JD, Goradia N, Gali R, Shapiro LC, Pradhan K, et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell. 2021; 39: 1081– 90. e2. https://doi.org/10.1016/j.ccell.2021.06.002 12Yazaki S, Yoshida T, Kojima Y, Yagishita S, Nakahama H, Okinaka K, et al. Difference in SARS-CoV-2 antibody status between patients with cancer and health care workers during the COVID-19 pandemic in Japan. JAMA Oncol. 2021; 7: 1141– 8. https://doi.org/10.1001/jamaoncol.2021.2159 13Goshen-Lago T, Waldhorn I, Holland R, Szwarcwort-Cohen M, Reiner-Benaim A, Shachor-Meyouhas Y, et al. Serologic status and toxic effects of the SARS-CoV-2 BNT162b2 vaccine in patients undergoing treatment for cancer. JAMA Oncologia. 2021; 7:e212675. https://doi.org/10.1001/jamaoncol.2021.2675 14Massarweh A, Eliakim-Raz N, Stemmer A, Levy-Barda A, Yust-Katz S, Zer A, et al. Evaluation of seropositivity following BNT162b2 messenger RNA vaccination for SARS-CoV-2 in patients undergoing treatment for cancer. JAMA Oncol. 2021; 7: 1133– 40. https://doi.org/10.1001/jamaoncol.2021.2155 15Monin L, Laing AG, Muñoz-Ruiz M, McKenzie DR, del Molino Del Barrio I, Alaguthurai T, et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: interim analysis of a prospective observational study. Lancet Oncol. 2021; 22: 765– 78. https://doi.org/10.1016/s1470-2045(21)00213-8 16Geisen UM, Berner DK, Tran F, Sümbül M, Vullriede L, Ciripoi M, et al. Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann Rheum Dis. 2021; 80: 1306– 11. https://doi.org/10.1136/annrheumdis-2021-220272 17Waissengrin B, Agbarya A, Safadi E, Padova H, Wolf I. Short-term safety of the BNT162b2 mRNA COVID-19 vaccine in patients with cancer treated with immune checkpoint inhibitors. Lancet Oncol. 2021; 22: 581– 3. https://doi.org/10.1016/s1470-2045(21)00155-8 18Au L, Fendler A, Shepherd STC, Rzeniewicz K, Cerrone M, Byrne F, et al. Cytokine release syndrome in a patient with colorectal cancer after vaccination with BNT162b2. Nat Med. 2021; 27: 1362– 6. https://doi.org/10.1038/s41591-021-01387-6 19Menni C, Klaser K, May A, Polidori L, Capdevila J, Louca P, et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID symptom study app in the UK: a prospective observational study. Lancet Infect Dis. 2021; 21: 939– 49. https://doi.org/10.1016/s1473-3099(21)00224-3 20Klein NP, Lewis N, Goddard K, Fireman B, Zerbo O, Hanson KE, et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA. 2021; 326: 1390– 9. https://doi.org/10.1001/jama.2021.15072 21Luo B, Li J, Hou X, Yang Q, Zhou Y, Ye J, et al. Indications for and contraindications of immune checkpoint inhibitors in cancer patients with COVID-19 vaccination. Future Oncol. 2021; 17: 3477– 84. https://doi.org/10.2217/fon-2021-0288
Comments (0)