
Remember me
Diseases caused by the biliary system are rare in children with acute abdomen. In children, acute cholecystitis often has an underlying disorder1 that is different from that in adults. Gallbladder torsion (GT), caused by a congenital gallbladder abnormality, has been reported in children with acute abdomen and is a life-threatening condition requiring emergency surgery.2 However, the effectiveness of emergency laparoscopic cholecystectomy (LC) for pediatric GT has not yet been reported. Here, we report a successful surgical case of a 3-year-old boy who underwent emergency LC for GT.
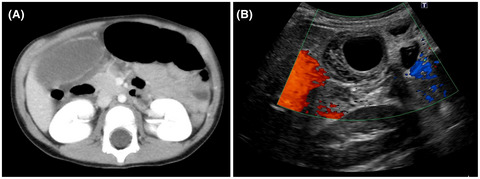
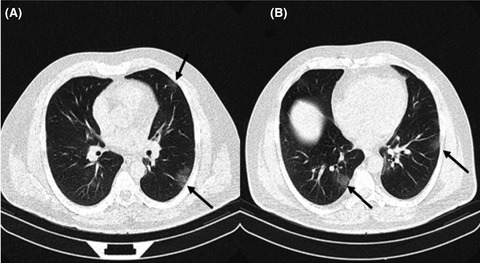
CASE REPORTA 3-year-old previously healthy boy was referred to an emergency medical center because of sudden abdominal pain and vomiting. Although he was diagnosed with acute gastroenteritis and prescribed medication, he continued to vomit several times, and his general condition worsened. Therefore, he was referred to our hospital the day after the onset of abdominal pain. Physical examination showed a flat and soft abdominal wall with mild rebound tenderness in the right hypochondrium and no palpable abdominal mass. Laboratory examinations showed a slightly elevated white blood cell (WBC) count of 16,500/μL, while C-reactive protein (0.25 mg/dL) and serum levels of liver enzymes were all within the normal ranges. Abdominal ultrasonography (AUS) revealed gallbladder wall thickness without gallstones. Additionally, a small amount of fluid was observed around the gallbladder and in the pelvic cavity. Because GT was not considered a differential diagnosis at the time of admission, he was admitted to the Department of Pediatrics, and treatment with antibiotics was started with a diagnosis of acute cholecystitis. Simultaneously, examinations for underlying disorders related to cholecystitis were planned; vasculitis, such as immunoglobulin A vasculitis or hemolytic anemia, were ruled out as a result. On day 1 of admission, the WBC count decreased to 12,500 /μl, and his abdominal pain slightly improved. Abdominal enhanced computed tomography (CT) showed swelling of the gallbladder with ascites, as did the AUS images from the day of admission (Fig. 1A). On day 2 of admission, due to the re-elevated WBC count of 16,000/μl, C-reactive protein level of 3.26 mg/dL, and persistent abdominal pain, a repeat AUS was carried out. An increase in the gallbladder wall thickness to 12 mm and a lack of intramural blood flow was noted (Fig. 1B), which led to a diagnosis of GT. The patient was referred to our department, and an emergency LC was carried out using the VISERA ELITE system (Olympus). A 12-mm trocar was inserted at the umbilical portion of a flexible laparoscope (LTF-S190-10; Olympus), followed by placement of three 5-mm ports, and the rest of the operation was carried out according to the standard procedure used in adult patients. The gallbladder was blackish, with severe edema, and surrounded by bloody ascites. After resection of the adhesion between the gallbladder and the greater omentum, the gallbladder was observed to be twisted 270° counterclockwise at the level of the cystic duct and mesentery (Fig. 2A). The gallbladder was easily untwisted clockwise to its natural position, which was classified as type I according to the Gross classification3 (Fig. 2B). After resecting a small amount of mesentery between the cystic duct and the liver bed, the cystic duct with the cystic artery was doubly ligated using Endoloop polydioxanone suture II and resected. The operation time was 104 min, and intraoperative blood loss was minimal. Microscopically, the resected specimen showed gangrenous cholecystitis without gallstones. Notably, the gallbladder bile culture was negative. The postoperative course was uneventful without any complications, and the patient was discharged on postoperative day 6.

Preoperative findings in a 3-year-old child with gallbladder torsion who underwent laparoscopic cholecystectomy. A, Day 1 of admission: abdominal enhanced computed tomography shows swelling of the gallbladder with ascites. Contrast effects on the gallbladder wall are observed. B, Day 2 of admission: abdominal ultrasonography reveals exacerbation of gallbladder wall thickness, 12 mm in size, and lack of intramural blood flow.

Intraoperative findings in a 3-year-old child with gallbladder torsion who underwent laparoscopic cholecystectomy. A, The gallbladder is twisted 270° counterclockwise at the level of cystic duct and mesentery. B, The gallbladder is untwisted clockwise to the natural position. There is a small amount of mesentery between the cystic duct and liver bed, which is classified as type I according to the Gross classification.
DISCUSSIONIn the present case, we report a case of pediatric GT that was diagnosed preoperatively by AUS, for which successful emergency LC was carried out. Gallbladder torsion is a cause of pediatric acute abdomen that may result in death. Levard et al.2 reported that two of 11 pediatric patients with GT died due to delayed diagnosis. However, in children, the symptoms are nonspecific4; accurate preoperative diagnosis is sometimes difficult, and the condition is often diagnosed as appendicitis.2, 5 Computed tomography, AUS, and magnetic resonance cholangiopancreatography have been reported to be useful for preoperative diagnosis of GT.4, 6 In particular, the twisted cystic pedicle on CT or AUS could be informative for a diagnosis. Even when there are improvements in clinical symptoms or blood results, as in the present case, repetitive imaging tests are recommended. When AUS shows an exacerbation of obvious gallbladder wall thickening and no intraluminal blood flow, prompt surgical exploration should be considered.
A review report by da Costa et al.7 in 2021 stated that LC in children is the gold standard surgery, and even pediatric patients can undergo surgery as safely as adults as they get older. However, in a report that compared emergency LC and elective LC for pediatric cholecystitis due to sickle cell disease, elective LC was recommended because of the higher number of postoperative complications in emergency LC.1 In a review of published reports of 28 cases of surgery for GT using LC, including three pediatric cases, Matsubara et al.8 reported that LC is a good option in surgery for GT because the mobile mesentery adheres less to the gallbladder bed. To the best of our knowledge, only four cases of LC for GT have been reported in the English literature in pediatric cases.4-6, 9 (Table 1). Although sufficient conclusions have not yet been established, LC for GT might be a good procedure, even in emergency pediatric cases. Of note, the present case was the youngest reported patient (at 3 years old) to successfully undergo LC for pediatric GT. Even in a pediatric patient with limited abdominal working space, which is a potential weakness of this method, LC for GT could be carried out without any complications, as easily as in adult cases.
Table 1. Reported cases of laparoscopic cholecystectomy for gallbladder torsion (GT) in pediatric patients Author, year (ref. no.) Age (years) Gender Preoperative diagnosis Time from onset to surgery (days) Operation time (min) Treatment for cystic duct Complications Postoperative hospital stay (days) Kimura et al. 20076 11 M GT 1 65 NA None 4 Matsuda et al. 20099 7 F GT 2 NA NA None 3 Inoue et al. 20114 9 M GT 4 NA NA None 4 Farnsworth et al. 20135 6 M Appendicitis 1 NA NA None NA Present case 3 M GT 3 104 Endoloop polydioxanone suture II None 6 F, female; M, male; NA, not available.In the present case of GT, the mobile mesentery, which includes the cystic duct and artery, was shortened in the short-axis direction. Therefore, the cystic duct and artery were resected after ligation with Endoloop polydioxanone suture II without creating the “critical view of safety” (CVS), which is important for preventing intraoperative complications.10 In reports on GT, the CVS has not been sufficiently evaluated, and most previous reports have described that treatment is easy because few parts adhere to the gallbladder bed. One advantage of laparoscopic surgery is magnified observation, and if the twisted cystic pedicle is apparent only in the gallbladder neck, the surgery can be safely carried out using treatment with Endoloop polydioxanone suture II. Rather, it might not be necessary to create the CVS to prevent injury of the cystic duct. However, the safety of the procedure should be further assessed.
In conclusion, we report a successful case of a 3-year-old boy who underwent emergency LC for GT. In children with acute abdomen, it is important to undertake prompt diagnosis while keeping GT in mind. Laparoscopic cholecystectomy for GT could be a safe and effective surgical procedure, even in pediatric patients.
ACKNOWLEDGMENTSWe would like to thank Editage for English language editing.
DISCLOSUREApproval of the research protocol: All authors participated in revising the manuscript and approved the final manuscript.
Informed consent: Written informed consent was obtained from the patient’s family to publish this case report and accompanying images.
Registry and the registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of interest: None.
Comments (0)