
Remember me




Thygeson‘s superficial punctate keratitis (TSPK) is a bilateral recurrent corneal epithelial keratopathy that affects the central cornea primarily. It is characterized by focal discrete round to oval crenated epithelial lesions that stain with fluorescein and rose bengal. Phillips Thygeson, in 1950, first published a case report on a transient, bilateral disorder, having coarse corneal epithelial lesions in absence of underlying stromal involvement.[1] In a series of more than 50 cases of superficial punctate keratitis during the study period 1956–1961, 29 cases had detailed, documented clinical and laboratory analysis.[2] The role of any microbiological agent or virus as an aetiologic factor could not be established. Idoxyuridine was found to be ineffective, and steroids though not curative but were found to transiently supress the symptoms.
Braley and Alexander reported their observation in nine patients followed over a period of 4–8 years.[3] They also reported the entity to be bilateral, involving epithelium and subepithelium, usually centrally located and predominantly in the superior half of the cornea. These opacities were irregular, whitish or grayish, vertically oval in shape and center of the opacity staining irregularly with fluorescein. They also described the remissions and exacerbated pattern of the entity. During exacerbations, numerous lesions were observed, and during remissions, one to two lesions were still noticed. Virus could be isolated only in one patient after repeated corneal scrapings; however, no inclusion bodies could be demonstrated. Gock et al. reported a case of 36-year-old woman who complained of blurred vision, ocular discomfort, watering, and photophobia without congestion continuing for the past 6 months.[4] Slit-lamp examination in both the eyes showed numerous discrete punctate epithelial lesions with crenated edges taking-up fluorescein stain. Underlying stroma and surrounding conjunctiva were also not involved. All these clinical features were in concordance with the features of TSPK.
In a case report by Lemp et al., virus could be successfully isolated from the cornea of a patient with superficial punctate keratitis.[5] This virus, after a series of tests, was identified as Varicella zoster. Forstot et al. reported a case series of three patients with TSPK who benefitted both symptomatically as well as visually from therapeutic soft contact lenses.[6] Duszak et al. reported TSPK in a 33-year-old African-American man and discussed in detail about the clinical picture, differential diagnosis, and management strategy.[7]
TPSK is often an under diagnosed entity and confused with infectious keratopathy. The purpose of this study is to report the clinical presentations and outcomes of TSPK in a case series of 13 patients, and provide a review of literature.
Case SeriesDuring the last 6 years, we examined 13 patients (Male: 3, Female: 10) in a tertiary eye care center in eastern India. The mean age of presentation was 34.3 ± 17.6 (range: 9–64) years [Table 1]. More than two-third patients (11/13) were ≤ 45 years. All except one had bilateral presentation [Fig. 1].
 Table 1:
Table 1: Demographic and Clinical Profile of Patients with Thygeson’s Superficial Punctate Keratitis
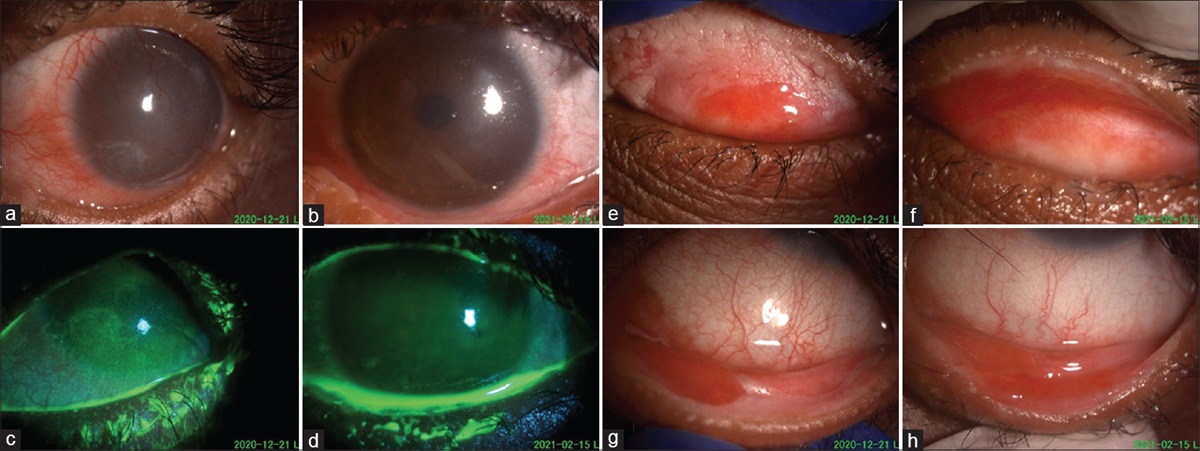
 Figure 1:
Figure 1: Slit-lamp photograph showing: (a and b) multiple epithelial lesions in a patient with bilateral involvement, (c) multiple epithelial lesions, (d) fluorescein-stained epithelial lesions involving central cornea, (e) fluorescein-stained positive lesions seen under cobalt blue filter light, (f) anterior segment ocular coherence tomography showing hyperreflectivity of the epithelial lesion with back shadowing into the corresponding corneal stroma
Most common symptom at presentation was watering (n = 8), followed by redness (n = 7) and photophobia (n = 7). Four patients complained of foreign body sensation. Four patients had burning sensation. Only one patient had complaints of pain at presentation. Most of the patients (92.3%) had more than one symptom. Combination of redness and watering (38.4%) was the most common symptom in our cohort. All patients had visual acuity of 0.2 logMAR or better at presentation. There was no seasonal trend observed in our patients. However, presentation in rainy season made clinical diagnosis more biased towards adenoviral or microsporidial etiology.
Seven patients were diagnosed as adenoviral and/or microsporidial keratoconjunctivitis at the first presentation. However, in follow-up visits, diagnosis was modified based on the chronicity and ruling-out other infective causes such as microsporidia and adenovirus. Based on clinical suspicion of Herpes simplex virus (HSV)/adenoviral, polymerase chain reaction (PCR) was carried out for three patients (Case# 5, 6, 7) for HSV and one patient (Case# 12) for adenoviral. Of these, one patient each was positive for HSV (Case# 7) and microsporidia (Case #8) respectively, as detected by PCR.
In our series, all patients received artificial tears at the first visit. While four patients could be managed with only artificial tears, others required multiple medications. These medication included topical steroid (loteprednol etabonate 0.5%, n = 3; fluorometholone 0.1%, n = 3), cyclosporine 0.1% (n = 4), and tacrolimus 0.03% (Talimus, tacroment) (n = 5). Some patients were subjected to combinations from the above-mentioned medications. The duration of treatment ranged from 1 to 42 months. Cyclosporine (n = 1), tacrolimus (n = 2), and steroid (n = 5) was started at the initial visit. The frequency of follow-up ranged from 2 to 36 clinical visits. The maximum visit (36) was seen in the youngest patient of our series, in a 9-year old girl, where microbiological sample sent for HSV-PCR was found to be positive. She resolved in a span of 3.5 years with lubricants, antivirals, cyclosporine, soft steroids, and finally maintained on tacrolimus for a few months without any further recurrence. The number of recurrences in our series ranged from 0 to 8 within a span of 0–3.5 years. Two out of 13 patients did not have even a single recurrence within the study period.
Literature SearchThe literature was searched using Pubmed and articles obtained from the bibliographies of these publications. We included references that we considered has a major contribution to the understanding and treatment of TSPK. The search words used were Thygeson‘s superficial punctate keratitis, cyclosporine, and tacrolimus.
Review of Literature Clinical featuresTSPK is a chronic insidious disease with episodes of exacerbations and remissions. The clinical course may last for as short as 2 months to as long as 41 years.[8] It is a bilateral, asymmetric condition where one eye may be affected during a certain episode. Many a times patients do not seek medical attention due to trivial symptoms. Others present with an insidious course in the form of annoying visual disturbance and irritation. This entity has been reported to affect any age group ranging from 2.5 to 70 years (average of 29 years).[9] These are similar to our series of patients with bilateral asymmetric presentation in the third to fourth decade of life. We noted a predilection for female gender (10/13) in our study.
During the episode of remission, patients present with complaints of ocular irritation, foreign body sensation, mild pain, photophobia, watering, mild congestion, and visual disturbance. Intensity of symptoms seems to be directly related to the severity of corneal involvement. Visual acuity may vary during the course of the disease. Usually vision is mildly affected especially during the active phase. However, long-term visual recovery is normal to near normal. In our series, 12 out of 13 patients had visual acuity of 20/20–20/30 at presentation. Braley and Alexander have mentioned that some of these patients were nervous, impatient, and appeared psychoneurotic.[3]
PathophysiologyThe pathophysiology of TSPK remains unclear. As mentioned in the literature, viral and immunogenic components have been found to be associated with the pathogenesis.[35]
Risk factorsThere are a few reports of recurrence of this entity after laser refractive surgery,[10111213] whereas other studies have suggested that both PRK and LASEK do not cause recurrence. Various viral infections have been associated with the disease like adenovirus, HSV,) and Varicella zoster virus.[35] Based on clinical suspicion, we performed PCR for HSV or adenovirus in four patients. All tests were negative except for one case where PCR was positive for HSV-1 DNA. Braley and Alexander could successfully isolate Varicella zoster virus from a case of TSPK.[3] Lemp et al. have mentioned about the nature of this disease, recurrence over years, mononuclear response with or without scarring, and suggested an unknown viral aetiology.[5] Darell et al. have reported a significant association of TSPK with HLA-DR3 and HLA-DW3.[14] The association of this antigen possibly alters the immune response leading to the prolonged episodes of exacerbations and remissions. We did not find any systemic association in our series.
DiagnosisTSPK presents bilaterally as numerous, strictly epithelial oval-shaped small white or grey dots [Fig. 1]. The underlying stroma and surrounding conjunctiva remain unaffected. The opacities appear more in the center and usually spare the peripheral cornea. The cyclic development of these lesions has been described in detail by Braley and Alexander.[3] At the initial stage, these lesions appear as minute, fuzzy looking flecks which does not disappear even on blinking. Gradually these flecks grow in size and transform into vertically oval slightly raised lesions with irregular edges. The center of lesions may fall off which then stains positively with fluorescein. This stage may persists for minutes to hours, but may soon get knocked off by blinking movements of the eyelids. After this stage, the lesion starts shrinking and eventually disappears. This whole cycle may take 12 h to weeks or more.[3] During the active phase, there may be presence of 20 lesions on an average which present predominantly in the central cornea as a conglomerate of coarse, oval-shaped, slightly raised granular lesions. This alters the smooth surface and is responsible for decreased vision, watering, photophobia, and foreign body sensation.[6] The lesions stain minimally with fluorescein and may or may not stain with rose bengal dye. The corneal sensation may be normal or slightly decreased but never completely absent as in Herpes simplex keratitis. During the inactive phase, these lesions flatten and appear as grayish, stellate-shaped, subepithelial opacities, and stain negatively with fluorescein. Some of these opacities may persist even in the absence of active disease.[14]
The lesions are transient and vary in distribution over the corneal surface. There may be foamy meibomian secretions near the canthus due to increased blinking and watering especially during exacerbations. Minute filaments may be present in few cases. Usually these are not true filaments and transiently present during the active phase.[15] The natural course follows exacerbations and remissions for several years till spontaneous resolution without developing any serious complications.
Confocal and Anterior Segment Optical Coherence Tomography (AS-OCT)Watson et al. first described the use of confocal microscopy in patients presenting with TSPK.[16] The wing cells of the epithelium showed disorganization along with irregularly appearing basal cells. The Bowman‘s membrane shows increased reflectivity with diffuse haziness. There is also increased frequency of appearance of microdot and refractile bodies in Bowman‘s membrane and anterior stroma. The subepithelial plexus gets distorted and wavy. Keratocytes of anterior stroma show reflective keratocytes with average five to six microdots per image. The posterior stroma and endothelium remain uninvolved. These reflective keratocytes may be responsible for the subepithelial scarring and hence decrease vision. All these findings in confocal microscopy may also indicate that TSPK is not limited only to the epithelium but may involve the anterior stroma of cornea as well. These changes were also found to be more obvious with the duration of the disease and were equally present even in the unaffected areas of the cornea. Fintelmann et al. have reported three cases of TSPK where AS-OCT showed increased reflectivity in the stroma just beneath the intraepithelial lesion.[17] This scarring may be a consequence of chronic inflammation and associated with the prolong duration of the disease.
Differential DiagnosisThe differential diagnosis of TSPK would include various aetiologies causing superficial punctate keratopathy (SPK). The process of evaluation of punctate keratopathy include general examination of the eye and adnexa, especially the periocular skin and lid margins, using special stains such as topical 2% fluorescein and 1% rose bengal on the ocular surface and interpreting the morphologic appearance, size, and location of the lesions. It may be subdivided as fine or coarse lesions based on their sizes. They can be epithelial or subepithelial keratopathy based on the location. The epithelial lesions may be classified further into punctate epithelial erosions (PEE), punctate epithelial keratopathy, and epithelial microcysts.[18]
PEE are fine faintly depressed lesions that stain positive with fluorescein and rose bengal. The location of the lesions are pointers to specific disorders. Diffuse involvement of the ocular surface is seen in viral conjunctivitis, drug toxicity or trauma. A superior localization is noted in superior limbic keratoconjunctivitis, trachoma, foreign body or trichiasis. Interpalpebral location is a characteristic of dry eyes, exposure, and neurotrophic keratopathy. Inferior lesions are noted in blepharoconjunctivitis, lagophthalmos, and trichiasis.[19]
Superficial punctate epithelial keratitisSuperficial punctate epithelial keratitis (SPEK) are small grayish white opacities that are visible even without staining and take-up rose bengal stains better than fluorescein. They may be fine or coarse with or without a surrounding inflammatory infiltrate. Fine SPEK are noted in sicca syndrome, exposure keratopathy, staphylococcal, chlamydial, and viral infections (molluscum and adenoviral). Coarse SPEK are seen in herpetic viral infections and Thygeson‘s SPK.[20]
Filamentary keratopathyFilamentary keratopathy is a form of SPEK that is commonly seen in dry eyes, trauma or foreign body, superior limbic keratoconjunctivitis. Filaments typically have a mucus core surrounded by epithelium of variable length and attached to the corneal surface at one end.
Combined epithelial and subepithelial punctate keratitisCorneal epithelial keratopathy and underlying subepithelial infiltrates may coexist. The lesions may wax and wane for variable time periods. The lesions may be unilateral or bilateral, and typically the subepithelial infiltrates appear 10–15 days after manifestation of epithelial keratitis. While the lesions respond to topical corticosteroids, the entity may relapse on withdrawal of steroids. Combined lesions are commonly seen after adenoviral keratoconjunctivitis, inclusion conjunctivitis, rosacea, trachoma, HSV, and varicella infections.[20] Specific disease entities with punctate keratitis include:
Adenoviral keratoconjunctivitisThe presence of multifocal subepithelial infiltrates is pathognomic of adenoviral keratoconjunctivitis, which may be noticed in 50% of cases especially with infection with serotype 8. There may be coexisting periocular lymphadenopathy, pharyngitis, and fever.[1821]
Microsporidia keratoconjunctivitisMicrosporidia is characterized by coarse multifocal raised lesions with conjunctival congestion. It is usually unilateral. There are typical raised “stuck on lesion” on the corneal epithelium resembling a superficial keratopathy. The organism is readily identifiable with a potassium hydroxide with calcofluor white wet mount that shows oval well-defined spores. The condition is usually self-resolving and may require topical lubricants only.[2223] In our patients, most common differential diagnosis was microsporidial keratoconjunctivitis. In five cases, cornea scraping was done. Direct smear examination was negative in all cases. In one patient, PCR was positive.
Herpes simplex keratitisHerpes simplex keratitis may present as coarse punctate epithelial spots or epithelial vesicles early in their clinical course. As the epithelial cells are laden with replicating virus, the cells undergo a progressive swelling and lysis. This causes the lesions to progress to a dendritic ulceration. The devitalized cells on the margin stain with rose Bengal, whereas the basement membrane is stained by fluorescein. This typical clinical feature is noted very early (12-24 h) of the disease manifestation.[2425] The youngest patient in the series was positive for HSV in PCR. She did not have any other features of HSV infection.
Herpes zoster keratitisHerpes zoster keratitis may initially involve the cornea as a coarse punctate epithelial keratitis with small raised focal lesions. The epithelium is swollen and blotchy with occasional mucus deposits. Epithelial vesicles may coalesce to form pseudodendrite that are broad, plaque like without a central ulceration. There are anterior stromal infiltrates characterized by sub Bowman‘s patchy granular infiltrates. Herpes zoster lesions have characteristic conjunctivitis, lid vesicles, and skin rashes that are dermatomal in distribution.[26]
Keratoconjunctivitis medicamentosaFrequent instillation of topical medications for long period of time may lead to corneal toxicity. Drugs, solvents, or preservatives such as benzakonium chloride may be the cause of keratopathy. These include brimonidine, prostaglandin analogues such as bimatoprost, acyclovir, and atropine. There is a punctate corneal epithelial staining especially with rose bengal, epithelial defects, and subepithelial infiltrates.[2027]
Keratoconjunctivitis siccaKeratoconjunctivits sicca may present variably as diffuse or confluent punctate lesions of the ocular surface with epithelial erosions. While there may be filaments or mucus strands, there may be corneal scarring, thinning with corneal peripheral vascularization. There may be diffuse staining of the corneal surface with rose bengal and fluorescein. Schirmer tests are subnormal.[28] In our series, a clinical diagnosis of dry eye was assumed in three patients, where dry eye workup test was done and found to be within normal range.
Treatment CorticosteroidsTopical corticosteroids are considered the mainstream of treatment for TSPK because they have been shown to be very successful at managing both clinical signs and symptoms. Various forms of topical steroids with different concentrations have been used. Topical steroids have been used during the episodes of exacerbation.[9] The use of steroids is warranted in patients who are significantly disabled by pain, photophobia, or reduced vision. Since it needs prolonged therapy, ocular side effect of steroid should be kept in mind. It may prolong the natural course of the disease.
TacrolimusTopical tacrolimus has been used successfully in cases of TSPK. In a retrospective case series, 14 cases were treated with tacrolimus 0.03% twice daily for 2 weeks followed by once at bedtime application.[29] Most of the patients in this series had improved vision, symptoms, and signs as long as patients were continuing their treatment. The authors have concluded this as an effective treatment without noticeable side effect. It is not a curative treatment. In a recent publication, tacrolimus (0.02%) solution has been used twice daily for a mean time period of 10 weeks for the treatment of TSPK.[30] We also found tacrolimus (0.03%) to be beneficial particularly in one patient who had maximum recurrences (8 episodes) and was maintained on tacrolimus for few months without any recurrences.
CyclosporineTopical cylosporine has been used as an alternative to topical steroid. Topical cyclosporine 2% with olive oil has been used for prolonged period for the treatment of TSPK.[31] After the use of the medication, all the lesions resolved, and cornea was clear in follow-up period. In a prospective study, Reinhard[32] et al. had used cyclosporine in 52 eyes of 28 patients. They included both adult and children in their study. The duration of treatment was for 6 months with a reducing frequency gradually. In 71 and 40% patients of adult and children, respectively, had complete suppression of lesions during treatment. Definite healing was achieved in one-third of adult patients. Lower concentration of cyclosporine (0.5%) has also been used in the treatment.[33] In our series, we treated successfully with cyclosporine (0.1%) in four cases.
TriflurothymidineNesburn[34] et al. have used trifluridine 1% drops in four patients with TSPK. Five of the six treated eyes responded favorably to topical trifluridine therapy. Symptoms and later the signs of the disease disappeared but more slowly than observed following topical corticosteroid therapy. Mild irritation and transient limbal follicle formation were the only side effects observed. The authors concluded that trifluridine is an effective and safe alternative to corticosteroids in the treatment of this condition and can be used as a steroid sparing agent.
Contact lensContact lens has been used for symptomatic relief and improves the compromised optical surface. Forstot[6] et al. have described the use of soft contact lens in three cases of TSPK. In all patients, visual acuity improved in addition to symptomatic relief. Two of three patients had used steroid for prolonged period before the usage of soft contact lens. The rapid resolution of epithelial lesions and symptomatic relief was noticed after patching or the use of contact lens.[35]
Photorefractive Keratectomy (PRK) with Phototherapeutic Keratectomy (PTK)There is a single case report mentioning about excellent visual recovery with no recurrence of corneal lesions in a young female of TSPK with low myopia after treatment with combined PRK with PTK procedure.[36] Recurrence of lesions beyond ablated area in a patient of TSPK after PRK has been reported.[13] On the contrary, recurrence of TSPK has also been reported after laser in situ keratomileusis.[12]
Artificial tearsConsidering the chronicity of the disease and the long-term side effects of steroid usage, artificial tears are prescribed for patients with TSPK either as combination therapy or monotherapy. Patients with mild symptoms may be managed with artificial tears.[37] Artificial tears are safe and can be primarily used for symptomatic relief.
ConclusionTSPK is a chronic bilateral disease with a course of remission and exacerbation. Though there is no significant affection of vision, patients are symptomatic. Proper history and clinical evaluation help to differentiate from other differential diagnoses. Prolonged treatment with topical medications is the mainstay of treatment. In our series, most patients were young and the common differential diagnoses were microsporidial and adenoviral keratoconjunctivtis. TSPK should be considered as a diagnosis of exclusion in cases of bilateral SPK of long duration.
Financial support and sponsorshipHyderabad Eye Research Foundation, Hyderabad.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interestThere are no conflicts of interest.
1. Thygeson P. Superficial punctate keratitis J Am Med Assoc. 1950;144:1544–9 2. Thygeson P. Clinical and laboratory observations on superficial punctate keratitis Am J Ophthalmol. 1966;61:1344–9 3. Braley AE, Alexander RC. Superficial punctate keratitis; isolation of a virus AMA Arch Ophthalmol. 1953;50:147–54 4. Gock G, Ong K, McClellan K. A classical case of Thygeson‘s superficial punctate keratitis Aust N Z J Ophthalmol. 1995;23:76–7 5. Lemp MA, Chambers RW Jr, Lundy J. Viral isolate in superficial punctate keratitis Arch Ophthalmol. 1974;91:8–10 6. Forstot SL, Binder PS. Treatment of Thygeson‘s superficial punctate keratopathy with soft contact lenses Am J Ophthalmol. 1979;88:186–9 7. Duszak RS. Diagnosis and management of Thygeson‘s superficial punctate keratitis Optometry. 2007;78:333–8 8. Tanzer DJ, Smith RE. Superficial punctate keratitis of thygeson: The longest course on record? Cornea. 1999;18:729–30 9. Tabbara KF, Ostler HB, Dawson C, Oh J. Thygeson's superficial punctate keratitis Ophthalmology. 1981;88:75–7 10. Jabbur NS, O‘Brien TP. Recurrence of keratitis after excimer laser keratectomy J Cataract Refract Surg. 2003;29:198–201 11. Seo KY, Lee JB, Jun RM, Kim EK. Recurrence of Thygeson‘s superficial punctate keratitis after photorefractive keratectomy Cornea. 2002;21:736–7 12. Netto MV, Chalita MR, Krueger RR. Thygeson‘s superficial punctate keratitis recurrence after laser in situ keratomileusis Am J Ophthalmol. 2004;138:507–8 13. Fite SW, Chodosh J. Photorefractive keratectomy for myopia in the setting of Thygeson‘s superficial punctate keratitis Cornea. 2001;20:425–6 14. Darrell RW. Thygeson‘s superficial punctate keratitis: Natural history and association with HLA DR3 Trans Am Ophthalmol Soc. 1981;79:486–516 15. Thygeson P. Further observations on superficial punctate keratitis Arch Ophthalmol. 1961;66:158–67 16. Watson SL, Hollingsworth J, Tullo AB. Confocal microscopy of Thygeson‘s superficial punctate keratopathy Cornea. 2003;22:294–9 17. Fintelmann RE, Vastine DW, Bloomer MM, Margolis TP. Thygeson superficial punctate keratitis and scarring Cornea. 2012;31:1446–8 18. Roussel T, Grutzmacher R, Coster D. Patterns of superficial keratopathy Aust J Ophthalmol. 1984;12:301–16 19. Weisenthal RW, Afshari NA, Bouchard CS, Kolby KA, Rootman DS, Tu EY, et alCantor LB, Rapuano CJ, Cioffi GA Examination Techniques for the External Eye and Cornea Basic and Clinical Science Course. American Academy of Ophthalmology 2015-16, Section 8: External Disease and Cornea.:29–61 20. Pettit TH, Meyer KT. The differential diagnosis of superficial punctate keratitis Int Ophthalmol Clin. 1984;24:79–92 21. Jhanji V, Chan TC, Li EY, Agarwal K, Vajpayee RB. Adenoviral keratoconjunctivitis Surv Ophthalmol. 2015;60:435–43 22. Das S, Sharma S, Sahu SK, Nayak SS, Kar S. Diagnosis, clinical features and treatment outcome of microsporidial keratoconjunctivitis Br J Ophthalmol. 2012;96:793–5 23. Joseph J, Vemuganti GK, Sharma S. Microsporidia: Emerging ocular pathogens Indian J Med Microbiol. 2005;23:80–91 24. Kaye S, Choudhary A. Herpes simplex keratitis Prog Retin Eye Res. 2006;25:355–80 25. Dawson CR, Togni B. Herpes simplex eye infections: Clinical manifestations, pathogenesis and management Surv Ophthalmol. 1976;21:121–35 26. Liesegang T. Corneal complications from herpes zoster ophthalmicus Ophthalmology. 1985;92:316–24 27. Okoro CC, Amiebenomo OM, Aruotu N. Medicamentosa keratoconjunctivitis: A case report Afr Vision Eye Health. 2016;75:a20 28. Jones BR. Differential diagnosis of punctate keratitis Int Ophthalmol Clin. 1962;2:591–611 29. Marquezan MC, Nascimento H, Vieira LA, Serapião M, Ghanem RC, Belfort R Jr, et al Effect of topical tacrolimus in the treatment of Thygeson‘s superficial punctate keratitis Am J Ophthalmol. 2015;160:663–8 30. Shoughy SS, Tabbara KF. Topical tacrolimus in Thygeson superficial punctate keratitis Cornea. 2020;39:742–4 31. Del Castillo JM, Del Castillo JB, Garcia-Sanchez J. Effect of topical cyclosporin A on Thygeson‘s superficial punctate keratitis Doc Ophthalmol. 1996;1997(93):193–8 32. Reinhard T, Sundmacher R. Topical cyclosporin A in Thygeson‘s superficial punctate keratitis Graefes Arch Clin Exp Ophthalmol. 1999;237:109–12 33. Hasanreisoglu M, Avisar R. Long-term topical cyclosporin A therapy in Thygeson‘s superficial punctate keratitis: A case report Cases J. 2008;1:415 34. Nesburn AB, Lowe GH 3rd, Lepoff NJ, Maguen E. Effect of topical trifluridine on Thygeson‘s superficial punctate keratitis Ophthalmology. 1984;91:1188–92 35. Goldberg DB, Schanzlin DJ, Brown SI. Management of Thygeson‘s superficial punctate keratitis Am J Ophthalmol. 1980;89:22–4 36. Goldstein MH, Feistmann JA, Bhatti MT. PRK-pTK as a treatment for a patient with Thygeson‘s superficial punctate keratopathy CLAO J. 2002;28:172–3 37. Nagra PK, Rapuano CJ, Cohen EJ, Laibson PR. Thygeson‘s superficial punctate keratitis: Ten years‘ experience Ophthalmology. 2004;111:34–7
Comments (0)