
Remember me
Conventional cardiopulmonary resuscitation (CPR) for cardiac arrest during pregnancy and postpartum has been reported to have a high survival rate.1 In emergency management in the obstetrics clinical setting, rescue is difficult due to the absence of an emergency physician and interhospital transfer. Herein, we report a rescue case in which cardiac arrest (CA) was caused by a nonhemorrhagic event after cesarean section and the patient was transferred immediately for extracorporeal cardiopulmonary resuscitation (ECPR) to an institution with limited obstetrics care. The success of resuscitation suggests that ECPR could be effective for postpartum CA that does not necessitate hemostatic intervention.
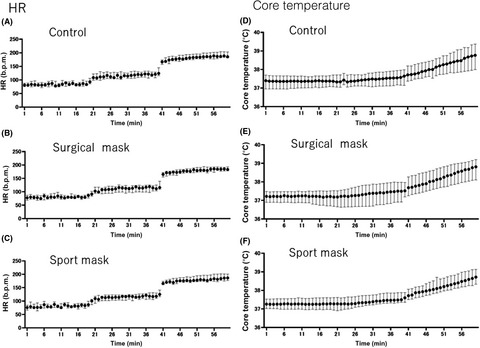
CASE PRESENTATIONA 39-year-old woman at 38 weeks of gestation received elective cesarean section at an obstetrics clinic. Her medical history included hypertension and no remarkable complications during pregnancy. Electrocardiography revealed no abnormality, such as QT elongation. Under spinal anesthesia with bupivacaine, the patient underwent surgery, and perioperative blood loss volume was approximately 300 ml. After delivery, gradual onset of bradycardia, loss of spontaneous respiration, and impalpable carotid pulsation were observed. Thus, CPR was immediately initiated. The initial electrocardiogram revealed ventricular fibrillation. Subsequently, tracheal intubation was carried out. The patient did not recover despite direct cardioversion and adrenaline administration. For further management and treatment, she was transferred to our institute while CPR was continued. The time from the onset of the CA to the departure from the clinic was 28 min. When the patient arrived at our institute, she did not recover despite continued CPR. Therefore, venoarterial extracorporeal membrane oxygenation (ECMO) through the right femoral vein and left femoral artery was started. The time from collapse to ECMO induction was 63 min (Fig. 1). Eighty minutes after ECMO induction, return of spontaneous circulation was achieved. Although coronary angiography and computed tomography were carried out, we could not detect the cause of the CA. Because of postoperative bleeding, targeted temperature management for normothermia was administered by ECMO. In spite of the disseminated intravascular coagulation on admission, early replacement of the coagulation factors with blood products prevented hemorrhagic events (Fig. 2). Levels of serum cardiac enzymes, such as creatinine kinase, were normal. The patient’s circulation improved over time, and ECMO was terminated on day 3 of hospitalization. Tracheal tube extubation was carried out on day 6. Although the head computed tomography scan on day 8 revealed a slightly hypoxic encephalopathy, the patient’s consciousness disturbance recovered gradually. She was transferred to a rehabilitation hospital 14 days after admission. Her cerebral performance category score2 was 3 at transfer. After 3 months of rehabilitation following discharge, cerebral function improved so that she could perform independent activities of daily life (cerebral performance category score: 2). While the patient was hospitalized, we tentatively diagnosed amniotic fluid embolism (AFE) as the cause of CA. However, zinc coproporphyrin I and sialyl-Tn antigen, the serum markers of AFE, were not found; therefore, anesthesia might have caused CA.

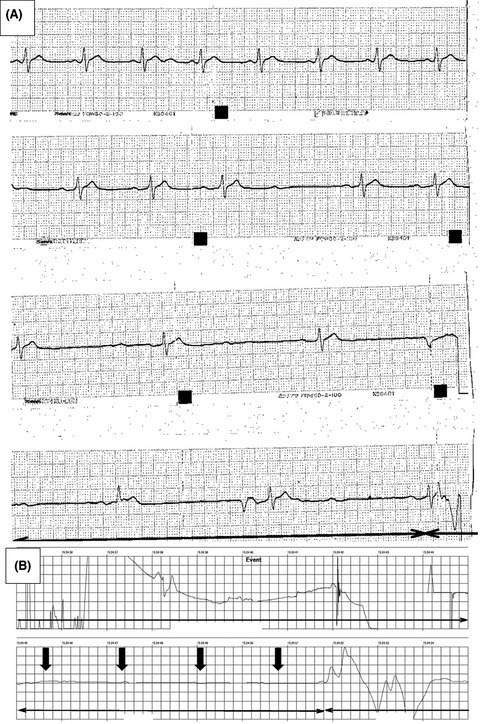
Time course of the case of a 39-year-old woman who had a cardiac arrest (CA) after cesarean section (CS). ECMO, extracorporeal membrane oxygenation; EMS, emergency medical service; VF, ventricular fibrillation.

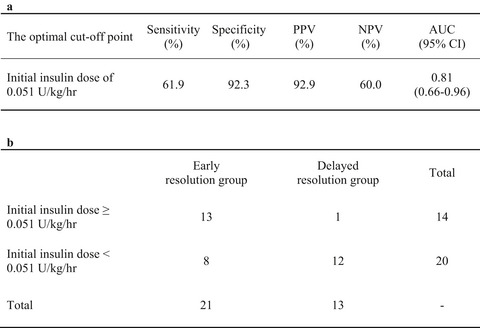
Time course of the laboratory data of a 39-year-old woman who had a cardiac arrest after cesarean section. Transfusions, including packed red blood cells (RBC; 2 U), fresh frozen plasma (FFP; 6 U), platelet products (PLT; 20 U), and fibrinogen (Fib) products (3 g), were carried out depending on the laboratory data. APTT, activated partial thromboplastin time; FDP, fibrin/fibrinogen degradation products; Hb, hemoglobin; PT-INR, prothrombin time – international normalized ratio.
Although a definitive diagnosis could not be established, clinical AFE, according to the Japanese criteria,3 could not be ruled out because the pathological evaluation of the uterus was not possible.
DISCUSSIONThe causes of CA after delivery are classified into hemorrhagic and nonhemorrhagic events. The Maternal Death Exploratory Committee in Japan and the Japan Association of Obstetricians and Gynecologists reported that the current mortality rates of pregnant and parturient women in Japan were as follows: postpartum hemorrhage, 23%; cerebrovascular disease, 16%; AFE, 13%; cardiovascular disease, 8%; pulmonary disease, 8%; and infection, 7%.4 Furthermore, in cases of nonhemorrhagic events, such as AFE and cardiovascular or cerebrovascular disease, the duration from the event to the onset of CA was less than 30 min. In contrast, in maternal deaths associated with hemorrhagic events, the duration from onset to CA ranged mostly from 1 to 3 h, and none of the patients had a CA within 30 min from the onset of the hemorrhagic event.4
Half of all pregnant women deliver at primary obstetric institutions, such as private clinics, in Japan. This means that 1 million deliveries per year are equally shared by general hospitals and private clinics. As most obstetric clinics in Japan have only a small number of beds and limited staff, they might have difficulty saving lives in critical emergencies. Prompt transfer to a facility with a medical team with technical skills in resuscitation is important. Regarding CA due to hemorrhagic events, clinical staff should have prior experience in transporting patients to highly specialized obstetric facilities.
However, for CA caused by nonhemorrhagic events, such as the present case, ECPR is a good indication as a definitive therapy. As Sharma et al.5 reported that ECMO induction for peripartum CA should be considered if no simultaneously occurring severe and uncontrollable active hemorrhage, such as uterine or gastric hemorrhage, are found, our case is a good indication for ECPR. However, patients with nonhemorrhagic CA requires more urgent interhospital transport than those with hemorrhagic CA. Although obstetric care was limited in our institute, a dispatched emergency technician suggested the indication for ECPR to the obstetrician in the clinic and informed the obstetrician that this was a nonhemorrhagic event due to the small amount of operative blood loss and absence of a bleeding tendency after delivery. As prompt resuscitation was undertaken in the clinic and the patient had a refractory ventricular fibrillation, we judged an indication for ECPR. In addition, we predicted that acute obstetric intervention was unnecessary because the CA was unlikely caused by the postpartum hemorrhage. The patient was transferred to our institute promptly and immediate ECPR was performed. Narita et al.6 emphasized that the collaboration of emergency physicians and obstetricians in the medical transfer system would contribute to a favorable outcome in severe peripartum emergencies. Our case clearly demonstrates this.
The Extracorporeal Life Support Organization guidelines have not clearly specified whether ECMO for peripartum CA is useful and safe. The reasons for this are that ECMO is considered a contraindication in patients with systemic bleeding,7 and 23% of peripartum CA cases were caused by obstetric hemorrhage.4 However, a meta-analysis of cases of ECMO for peripartum CA revealed favorable outcomes in terms of maternal and fetal survival rates, which were 77.2% and 69.1%, respectively.8 Kollengode et al.9 reported that the survival rate of patients with peripartum CA who had undergone ECPR was 54.8%. We speculate that the favorable outcomes were achieved because ECMO was mainly applied in nonhemorrhagic cases. As most peripartum women are young and healthy, ECPR could be considered if the cause of the CA seems reversible.10 Therefore, ECPR for peripartum CA caused by nonhemorrhagic events has potential favorable neurological outcomes. Because this case occurred under specific medical and social conditions in Japan, it is not clear whether the lessons learned in this case can be applied universally.
CONCLUSIONIn Japan, where half of deliveries are carried out at primary obstetric institutions, we successfully managed a case of peripartum CA that resulted from a nonhemorrhagic cause, and a favorable neurological outcome was achieved due to prompt interhospital transfer and aggressive treatment, such as ECPR, at an institution with limited obstetrics facilities.
ACKNOWLEDGMENTSThe authors would like to thank Dr. Naohiro Kanayama for the analysis of zinc coproporphyrin I and sialyl-Tn antigen and for his advice on the manuscript.
DISCLOSUREApproval of the research protocol: Approved by the ethics committee of Hyogo Emergency Medical Center.
Informed consent: The patient and her family provided written informed consent for the publication of this case report.
Registry and registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of interest: None.
REFERENCES
1Beckett VA, Knight M, Sharpe P. The CAPS study: incidence, management and outcomes of cardiac arrest in pregnancy in the UK: a prospective, descriptive study. BJOG 2017; 124: 1374– 81. 2Cummins RO, Chamberlain DA, Abramson NS, et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: the Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 1991; 84: 960– 75. 3Kanayama N, Tamura N. Amniotic fluid embolism: pathophysiology and new strategies for management. J. Obstet. Gynaecol. Res. 2014; 40: 1507– 17. 4Hasegawa J, Sekizawa A, Tanaka H, et al. Current status of pregnancy-related maternal mortality in Japan: a report from material death exploratory committee in Japan. BMJ. Open 2016; 21: 6. 5Sharma NS, Wille KM, Bellot SC, et al. Modern use of Extracorporeal life support in pregnancy and postpartum. ASAIO J. 2015; 61: 110– 4. 6Narita M, Nakao S, Matsuoka T, et al. Collaboration and teamwork between emergency and critical care centers and maternal-child medical care centers. Jpn. J. Abdom. Emerg. Med. 2018; 38: 489– 91. 7 Extracorporeal Life Support Organization. ELSO general guidelines for all ECLS cases, 2017. I-B. Available from: https://www.elso.org/Resources/Guidelines.aspx 8Zhang JJY, Ong JA, Syn NL, et al. Extracorporeal membrane oxygenation in pregnant and postpartum women: a systemic review and meta-regression analysis. J. Intensive Care Med. 2019; 36: 220– 8. 9Kollengode R, Chuen SE, Peter R, et al. Extracorporeal membrane oxygenation in pregnancy: an analysis of Extracorporeal Life Support Organization Registry. Crit. Care Med. 2020; 48: 696– 703. 10Carolyn MW, Kathleen AS, Tracy AM. Extracorporeal membrane oxygenation in pregnant and postpartum women: a ten-years case series. Am. J. Obstet. Gynecol. 2020; 2: 100108.
Comments (0)