
Remember me
In aging societies, end-of-life care and the provision of emergency medical services (EMS) for elderly individuals are urgent matters. A do-not-attempt-to-resuscitate (DNAR) order is defined in Japan as mandating that no resuscitation be carried out when the individual with the DNAR experiences cardiopulmonary arrest (CPA). A DNAR is meant to enable individuals who have chronic and irreversible underlying disease (e.g., end-stage cancer) to spend the end of their lives in a dignified manner in accord with their desire, in advance of CPA. In Japan, the Ministry of Health, Labour and Welfare first published the policy for end-of-life care, that is, the Guideline Regarding the End-of-Life Care Decision-Making Process,1 in 2007. This guideline emphasizes that the decision-making process needs to be based on a discussion between the patient and health-care workers (HCWs) involved in the patient’s case. This process, referred to as advance care planning (ACP), has been shown to improve the quality of end-of-life care.2
In 2014, the Ministry of Health, Labour and Welfare issued a revised version of the guidelines,3 and the Japanese Society of Intensive Care Medicine, the Japanese Association for Acute Medicine, and the Japanese Circulation Society then jointly published their Guidelines for End-of-Life Care in Acute and Intensive Care Medicine.4 As a result, the awareness and understanding of DNAR orders and end-of-life care is improving among health-care staff in hospitals. However, a clear social consensus regarding patients’ right to refuse medical treatment remains to be established in Japan. Moreover, no guidelines have been published on the implementation of DNAR orders in cases of out-of-hospital cardiac arrest (OHCA). In fact, it is not uncommon for a family member or staff to call an ambulance when they witness an individual experiencing cardiac arrest at home or in a nursing home, even though the individual had completed a DNAR in advance.
The Japanese Society for Emergency Medicine recommends that when the local EMS has been called for an individual with a DNAR who is experiencing an OHCA, the individual’s home-care physician should be contacted directly for confirmation that resuscitation should not be performed.5 However, that recommendation is not legally binding, thus the decision to attempt resuscitation is left to the judgment of the EMS team. Currently, even if the individual has a DNAR order, if an ambulance has been called, the EMS team is generally obligated to attempt resuscitation. As a result, in not a small number of cases, paramedics called to the scene struggle to deal with the confusion and conflicting demands related to what treatment procedures they should provide and to what extent they should respect the individual’s DNAR order.
We undertook the present study to investigate the current status of EMS use among OHCA patients with a DNAR order obtained in advance of their cardiac arrest and examine the factors that influence this EMS use.
Methods Study design and settingThis study was undertaken in Sagamihara, Japan, a city in the northern part of Kanagawa Prefecture, with a population of approximately 720,000. Our hospital is the only tertiary emergency facility in this city. This was a prospective study examining all of the OHCA cases in which a Sagamihara Municipal Fire Department EMS team was called between May 30, 2019 and February 15, 2020. In principle, each OHCA case is transported to our hospital according to the regulations of medical control in this area. However, if the patient has any underlying diseases and worsening of the underlying disease could be the cause of CPA, the patients are transported to their attending hospital. In cases in which the patient has a home-care physician or a DNAR order, the EMS team can also transport the patient to another hospital other than our hospital. These decisions of transported facility are made according to the direct instructions from emergency physicians of our facility (on-line medical control). There are no specific rules regarding the actions of the EMS team to be taken in the field for DNAR patients in our region. In such cases, paramedics have directly received instructions through on-line medical control, and they may perform chest compressions and assist ventilation using a bag valve mask during patient transport depending on the situation.
Data collectionWith the cooperation of the Sagamihara Fire Department, we collected the following data from the fact-finding survey completed for each OHCA patient.
Emergency medical services patient-related dataThe following information was obtained: the patient’s age, the site of the medical event’s occurrence, the EMS caller, underlying disease, in-home medical care intervention, the DNAR order instructions and content, the home-care physician contacted, outpatient outcomes, and the outcome 1 month later (Utstein Style): cerebral performance category and overall performance category.
Confirmation of DNAR orders was obtained by EMS team listening to family members or other bystanders on-site.
Prehospital factorsThe following prehospital information was obtained: time of transport, EMS caller-related data, the transporting EMS team, witnesses of the CPA, whether bystanders undertook cardiopulmonary resuscitation (CPR), EMS team-initiated CPR, CPR discontinuation, the EMS medical procedures implemented, the hospital to which the patient was transported (hereafter “transported hospital”), and the reason(s) for the selection of that hospital.
Cardiopulmonary resuscitation discontinuation was defined as cases in which CPR was interrupted or CPR was not carried out in a prehospital situation. These decisions were made in collaboration with the home-care physician, with instructions provided by the on-line medical control.
Study outcomes and statistical analysisThe primary outcome of this study was the rate of the use of EMS despite the presence of a DNAR order in advance. We divided the cases into two groups based on the presence or absence of a DNAR order in advance, and we examined the factors that affected the DNAR orders and EMS use. When the two groups were compared, the cases in which the presence or absence of a DNAR order was unknown were excluded. Significance was tested using a Mann–Whitney U-test for continuous variables and Fisher’s exact test for proportions. We undertook a logistic regression analysis as a multivariate analysis to identify factors associated with a DNAR order in advance. Probability (p)-values less than 0.05 were considered significant.
ResultsOf the 26,881 cases for which the EMS was called in Sagamihara City during the study period, there were 396 cases of OHCA. The characteristics of the patients are summarized in Table 1. The patients’ mean age was 75 ± 18 years. Patients aged 65 years or older accounted for 319 (80.6%) of the 396 cases, and 253 (63.9%) were 75 years or older (Fig. 1). Approximately 70% of the patients had an underlying disease. The overall survival-to-discharge rate was 6.6% (26 cases), and the rate of a good outcome (cerebral performance category 1 or 2) at 1 month after the OHCA was only 4.1% (16 cases).
Table 1. Study population characteristics (n = 396) n % Age, years; mean ± SD 75 ± 18 Patients aged ≥65 319 80.6 Patients aged ≥75 253 63.9 Place of CPA occurrence Home 260 65.7 Nursing home 73 18.4 Another hospital 4 1.0 Outdoors/outdoor facility 59 14.9 EMS caller Patient/family member 234 59.1 Facility staff member 78 19.7 Passer-by 27 6.8 Others 57 14.4 Underlying disease (multiple answers allowed) 284 71.7 Malignant tumor 62 15.7 Chronic heart disease 51 12.9 Cerebrovascular disorder 23 5.8 Chronic pulmonary disease 7 1.8 Severe dementia 9 2.3 Bedridden 46 11.6 Others 86 21.7 Witnessed CPA (+) 154 38.9 Bystander CPR (+) 200 50.5 Family member 84 21.2 Physician 3 0.8 Nurse 9 2.3 Facility staff member 46 11.6 Others 34 8.6 In-home medical care intervention (+) 17 4.3 Transported hospitals Tertiary emergency facility 293 74.0 Secondary emergency facility 84 21.2 Another hospital 18 4.5 Canceled transportation 1 0. 3 Outpatient death (+) 339 85.6 Return of spontaneous circulation (+) 56 14.1 Survival to discharge (+) 26 6.6 CPC 1 9 2.3 2 7 1.8 3 6 1.5 4 4 1.0 5 368 92.9 Unknown 2 0.5 OPC 1 8 2.0 2 8 2.0 3 6 1.5 4 4 1.0 5 368 92.9 Unknown 2 0.5 DNAR order in advance (+) 45 11.4 Verbal 27 60.0 (/45) Documentation 12 26.7 (/45) Other 6 13.3 (/45) Abbreviations: CPA, cardiopulmonary arrest; CPC, cerebral performance category; CPR, cardiopulmonary resuscitation; DNAR, do not attempt resuscitation; EMS, emergency medical services; OPC, overall performance category.
Number of out-of-hospital cardiac arrest (OHCA) cases with a do-not-attempt-resuscitation (DNAR) order in advance, by age group. The total numbers of OHCA cases and DNAR orders were 396 and 45, respectively. By age group, the patients in their 80s had the highest number of cases of both OHCA (137 cases, 34.6%) and a DNAR order (28 cases, 62.2%). The number of cases of OHCA was the second highest in the 70s (94 cases, 23.7%) and the third highest in the 90s (57 cases, 14.4%) but concerning the existence of a DNAR order, the 90s showed the second highest prevalence (9 cases, 20.0%). There were no cases with a DNAR order under the age of 50 years.
A total of 45 (11.4%) of the patients had a DNAR order in advance. By age group, the patients in their 80s had the highest prevalence of DNAR orders (62.2%), followed by patients in their 90s (20.0%; Fig. 1). Only 12 (26.7%) of the orders were confirmed by documentation. In the OHCA cases that occurred in home, the confirmation was mostly only verbal (76.9%), whereas the confirmation of the cases that occurred at nursing homes was mostly from documentation (57.9%; Fig. 2).

Do-not-attempt-resuscitation (DNAR) orders based on where the cardiopulmonary arrest occurred. (a) Overall: Of the 45 cases with DNAR orders, 27 cases (60.0%) were verbal only and 12 cases (26.7%) were a written document. (b) For cases that occurred at home, most of the DNAR orders were verbal (76.9%). (c) The DNAR orders in most of the cases that occurred at a nursing home were written instructions (57.9%).
There were only two cases in which the patient’s home-care physician rushed to the patient’s CPA site, and CPR was stopped in one case. In the remaining 43 (95.6%) cases, CPR was carried out by the EMS team despite the patient’s DNAR order being confirmed, with transport of the patient to a hospital. Of the 45 cases in total with a DNAR, 17 (37.8%) were transported to our tertiary emergency facility. Forty-one of the 45 patients underwent basic life support only, whereas four patients received some kind of advanced resuscitative treatment. Thus, it was assumed that, in these four cases, families changed their opinion despite DNAR advance directives during EMS treatment.
In the comparison based on the presence or absence of a DNAR order excluding 18 cases with “unknown” regarding a DNAR order, we observed significant between-group differences in patient age, the site of the CPA (nursing home), the EMS caller (facility staff member), underlying disease (severe dementia), in-home medical care intervention, EMS treatment, and transported hospitals (Table 2). The rate of CPR discontinuation was not significantly different between the cases with or without a DNAR order.
Table 2. Comparison of groups of Japanese patients with and without a do-not-attempt-resuscitation (DNAR) order in advance of out-of-hospital cardiopulmonary arrest (CPA)DNAR (+)
(n = 45)
DNAR (−)
(n = 333)
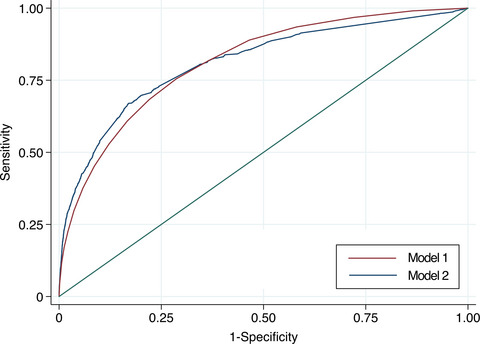
P-value Age, years; mean ± SD 84.8 ± 7.6 74.0 ± 18.5 <0.001* Place of CPA occurrence, % Home 26 (57.8) 232 (69.7) 0.125 Nursing home 19 (42.2) 53 (15.9) <0.001* Another hospital 0 (0.0) 4 (1.2) >0.999 Outdoors/outdoor facility 0 (0.0) 44 (13.2) 0.005* EMS caller, % Patient/family member 25 (55.6) 207 (62.2) 0.417 Facility staff member 19 (42.2) 58 (17.4) <0.001* Passer-by 0 (0.0) 18,5.4) 0.146 Others 1 (2.2) 50 (15.0) 0.018* Witnessed CPA (+), % 16 (35.6) 130 (39.0) 0.746 Bystander CPR (+), % 27 (60.0) 166 (49.8) 0.266 Underlying disease, % (multiple answers allowed) 31 (68.9) 195 (58.6) 0.022* Malignant tumor 11 (24.4) 49 (14.7) 0.125 Chronic heart disease 4 (8.9) 46 (13.8) 0.484 Cerebrovascular disorder 4 (8.9) 18 (5.4) 0.315 Chronic pulmonary disease 2 (4.4) 5 (1.5) 0.198 Severe dementia 4 (8.9) 5 (1.5) 0.014* Bedridden 9 (20.0) 37 (11.1) 0.092 Others 4 (8.9) 81 (24.3) 0.021* In-home medical care intervention (+), % 7 (15.6) 10 (3.0) 0.002* CPR discontinuation (+), % 5 (11.1) 30 (9.0) 0.589 EMS treatment, % (multiple answers allowed) Only basic life support 41 (91.1) 59 (17.7) <0.001* Airway management using equipment 2 (4.4) 222 (66.7) <0.001* Intravenous catheterization 2 (4.4) 186 (55.9) <0.001* Adrenaline administration 2 (4.4) 172 (51.7) <0.001* Others 4 (8.9) 30 (9.0) >0.999 Transported hospital, % Tertiary emergency facility 17 (37.8) 276 (82.9) <0.001* Secondary emergency facility 27 (60.0) 57 (17.1) <0.001* Canceled transportation 1 (2.2) 0 (0.0) 0.119 CPC, % 1 0 (0.0) 8 (2.4) 0.604 2 1 (2.2) 6 (1.8) 0.591 3 1 (2.2) 5 (1.5) 0.535 4 0 (0.0) 2 (0.6) >0.999 5 43 (95.6) 310 (93.1) 0.753 Unknown 0 (0.0) 2 (0.6) >0.999 OPC, % 1 0 (0.0) 7 (2.1) >0.999 2 1 (2.2) 7 (2.1) >0.999 3 1 (2.2) 5 (1.5) 0.535 4 0 (0.0) 2 (0.6) >0.999 5 43 (95.6) 310 (93.1) 0.753 Unknown 0 (0.0) 2 (0.6) >0.999 Note: Data are shown as n (%) unless otherwise indicated. Abbreviations: CPC, cerebral performance category; CPR, cardiopulmonary resuscitation; EMS, emergency medical services; OPC, overall performance category. *P < 0.05.The results of the multivariate logistic regression analysis indicated that only patient age was an independent variable affecting the presence of a DNAR order in advance for OHCA cases (odds ratio, 1.092; 95% confidence interval, 1.030–1.157; p = 0.003). The cut-off value based on the receiver operating characteristic curve for age for a confirmed DNAR order in advance was 78.5 years old (Fig. 3).

Receiver operating characteristic (ROC) curve of age for confirmed do-not-attempt-resuscitation (DNAR) orders in advance of out-of-hospital cardiac arrest. The cut-off value for the ROC curve was calculated by the Youden index. The area under the ROC curve was 0.694 (95% confidence interval, 0.627–0.761), and the most appropriate cut-off was 78.5 years (sensitivity, 0.867; specificity, 0.495).
DiscussionOur analyses revealed that 11.4% of the patients in our city’s region in Japan who experienced an OHCA used EMS despite having a DNAR directive. Corresponding reported values are 7.5% in France,6 6.2% in the UK,7 and 9.9% in a county in the state of Washington, USA8; the percentage in this study is higher than those observed in other parts of the world. Our findings suggest that ACP is not yet generally acknowledged in Japan, and there are few written DNAR orders among the patients with chronic underlying diseases who experienced an OHCA. In this study, age was the only independent factor for DNAR advanced directives, with a cut-off value of 78.5 years. This also could suggest that ACP and DNAR advance directives should be given a little earlier to provide medical care that reflects the patient’s wishes because the mean age of CPA patients in this study was 75 years, which is 3.5 years younger than the cut-off value. Home-care physicians and nursing homes that provide long-term treatment for individuals with underlying disease play an extremely important role in end-of-life care and engaging their patients in ACP, as roughly 70% of patients are unable to make such decisions when they are at a terminal stage,9 and there are many EMS uses of DNARs in nursing homes.10
In his or her ACP, an individual should repeatedly discuss end-of-life medical treatments with all of the HCWs related to their end-of-life care, including the patient’s family members, and the individual should clearly express their wishes in written documents. In Japan, only 1.1% of nursing homes have a full-time physician on staff, and the number of full-time physicians per facility has been shown to be extremely low (0.2).11 In addition, the physicians’ main duties do not usually include dealing with acute changes in residents’ conditions or treating injuries or illnesses, and obtaining the physicians’ assistance on their days off can be difficult. There is an additional practical problem: home-care physicians do not have sufficient time to adequately engage in ACP discussions with patients within the limited time available for medical consultations.
In order to provide patient-oriented end-of-life care, it is necessary to establish a system for on-site EMS treatment when a DNAR can be confirmed, not only when ACP is discussed. Currently, even if a patient has a DNAR order in place, it would not be permissible for the EMS team to decide on its own to transport the patient without trying to resuscitate him or her or to discontinue resuscitation.12 However, as shown in this study, there are cases in which older adults at home or in a nursing home have a clearly written DNAR order that results in conflict and confusion for the EMS team. This issue received recognition nationally, and in 2017, the Japanese Society for Clinical Emergency Medicine issued its Recommendations Regarding the Performance of Cardiopulmonary Resuscitation in Emergencies that would Observe the Wishes of Ill or Injured Individuals in the Final Stage of Life.5 These recommendations proposed a protocol for not performing CPR in cases in which it can be confirmed that there is a written DNAR order or in which DNAR instructions can be confirmed with the patient’s primary care physician or an online medical control physician. However, due to the legal ambiguity that remains, the recommendations are yet to be widely adopted.
According to a fact-finding survey by a Fire and Disaster Management Agency subcommittee in Japan published in 2018,13 as many as 54.4% of fire department headquarter offices had not determined how to respond to DNAR orders. Moreover, the survey revealed that even when municipal fire departments make their decisions independently, 60.5% follow the usual on-site protocol and perform CPR before transporting the patient to a medical center. In contrast, in the above-cited study,8 the on-site CPR was discontinued for 82% of OHCA patients with a confirmed DNAR in accord with the protocol. Legal arrangements regarding the handling of a DNAR directive could be required in order to respect the wishes of patients in Japan as well.
LimitationsThis study has some limitations to address. First, because the study sample consisted only of cases of EMS calls for OHCA, cases in which home-care physicians attended to OHCA patients in their homes with no EMS call being made were not included. It is thus possible that the EMS call was made because of a lack of involvement of this type of physician in the patient’s care. As a result, selection bias could have led to results indicating a lower prevalence of DNAR orders plus a higher prevalence of cases in which a home-care physician is not involved in the patient’s care than is actually true overall. Further investigations should be carried out to obtain a better understanding of the extent to which home-care physicians are proactively engaged in end-of-life care and attending to dying patients in their homes.
In addition, the data in this study were collected in a medical control region that has no specific rules regarding DNAR cases. Depending on the region, there could be rules governing both the medical procedures that EMS teams can carry out in DNAR cases and the facilities to which patients are to be transported.
ConclusionThe results of this study suggest that DNAR orders and ACP are under-utilized in Japan. Currently, an EMS team could be required to attempt resuscitation against a patient’s DNAR order obtained in advance, even when the EMS team can confirm that the patient has clearly authorized the DNAR order. Providing emergency treatment that meets patients’ wishes by clarifying the response to DNAR orders is important.
AcknowledgmentsThis study was supported by the Foundation for Ambulance Service Development for “Provision of subsidies to innovative investigation and research of ambulance services.”
DisclosuresApproval of the research protocol: This study protocol was approved by the Kitasato University School of Medicine and Hospital Ethics Committee (Approval No. B19-020). This study involved human participants and conformed with the principles of the Declaration of Helsinki and its amendments.
Informed consent: The need for informed consent from the patients or patients’ families was waived by the Ethics Committee because the study involved only a fact-finding survey with no interventions.
Registry and the registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of interest: None.
References
1 Ministry of Health, Labour and Welfare. Guidelines regarding the end-of-life care decision-making process (in Japanese). Available at: https://www.mhlw.go.jp/shingi/2007/05/dl/s0521-11a.pdf 2Detering KM, Hankock AD, Reade MC, et al. The impact of advance care planning on end of life care in elderly patients: Randomized controlled trial. Br. Med. J. 2010; 340: c1345. 3 Ministry of Health, Labour and Welfare. Guidelines regarding the decision-making process for medical care at the final stage of life (in Japanese); 2018. Available at: https://www.mhlw.go.jp/file/06-Seisakujouhou-10800000-Iseikyoku/0000197721.pdf 4 Japanese Society of Intensive Care Medicine, Japanese Association for Acute Medicine, Japanese Circulation Society. Guidelines for end-of-life care in acute care and intensive care medicine: Recommendations from three medical associations (in Japanese). Available at: http://www.jsicm.org/pdf/1guidelines1410.pdf 5 Japanese Society for Clinical Emergency Medicine. Recommendations regarding the performance of cardiopulmonary resuscitation in emergencies that would observe the wishes of ill or injured individuals in the final stage of life (in Japanese). Available at: http://plaza.umin.ac.jp/~GHDNet/sennyu/c221-JSEM.pdf 6Reuter PG, Agostinucci JM, Bertrand P, et al. Prevalence of advance directives and impact on advanced life support in out-of-hospital cardiac arrest victims. Resuscitation 2017; 116: 105– 8. 7Rajagopal S, Kaye CR, Lall R, et al. Characteristics of patients who are not resuscitated in out of hospital cardiac arrests and opportunities to improve community response to cardiac arrest. Resuscitation 2016; 109: 110– 5. 8Counts CR, Blackwood J, Winchell R, et al. Emergency medical services and do not attempt resuscitation directives among patients with out-of-hospital cardiac arrest. Resuscitation 2021; 158: 73– 8. 9Silveira MJ, Kim SYH, Langa KM. Advance directives and outcomes of surrogate decision making before death. N. Engl. J. Med. 2010; 362: 1211– 8. 10Kangasniemi H, Setälä P, Olkinuora A, et al.
Comments (0)