
Remember me



It is estimated that there are 570 000 new diagnoses of esophageal cancer (EC) and 510 000 deaths per year, representing the sixth most common cause of cancer-related deaths worldwide.1, 2 In China, it is also a leading cause of death, and the majority of cases are diagnosed at advanced stages and not eligible for surgery.3, 4 At present, a definitive CRT has been given priority as the standard treatment for inoperable EC, and good response could increase patient survival.5, 6 However, owing to individual differences and tumor heterogeneity, not all patients could benefit from the CRT approach.7, 8 The treatment effect depends heavily on the response to CRT, and it is crucial to predict the response as early as possible to avoid side effects for timely adjustment of treatment strategies.
The main traditional imaging methods for evaluating the treatment response of EC patients administered CRT include esophagography and computed tomography (CT), which analyze pathological changes of the esophagus only for morphology, lagging behind biometric changes.9, 10 Although fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) could reflect metabolic changes and is helpful in evaluating the treatment response to CRT in EC patients, radiation exposure and high cost are fatal disadvantages, especially for long-term follow-up.
Magnetic resonance imaging (MRI) has been widely used in tumor detection and treatment evaluation thanks to excellent soft tissue resolution and nonionizing radiation. Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) is an advanced MRI; beside the advantages of traditional MRI, it measures the properties of tumor microvascular structure and permeability, and evaluates the functional tissue information with quantitative parameters.11 In DCE-MRI examination, quantitative parameters such as ktrans (volume transfer constant in min−1), kep (rate constant in min−1), and ve (volume fraction of the extravascular extracellular space, which is dimensionless) could be obtained from pharmacokinetic models.12, 13 Current studies have reported the potential role of DCE-MRI parameters in assessing the treatment response in different tumors6, 13-16 as well as its value in predicting tumor-related biomarkers.17, 18
Regarding the prediction of tumor-related biomarkers, based on the advantages of DEC-MRI in determining vascular permeability, hypoxia-inducible factor-1-alpha (HIF-1α) was chosen as a research indicator in this study. As a core transcription factor under hypoxia in the microenvironment, HIF-1α is involved in mediating biological behaviors such as apoptosis, proliferation, and migration.19, 20 Current reports have further suggested that hypoxic cells could not only increase the resistance of tumor cells to CRT, but also render the tumor more invasive and prone to metastasis.21, 22 In addition, higher HIF-1α expression is associated with lower treatment response and reduced survival.23, 24 Therefore, the prediction of HIF-1α expression would also contribute to early efficacy assessment in EC patients. At present, data reported about tumor hypoxia are typically dependent on the pathological method, which is an invasive and undesirable approach for some patients. Hence, it would be beneficial for the patients to predict HIF-1α expression by DCE-MRI in a noninvasive manner.
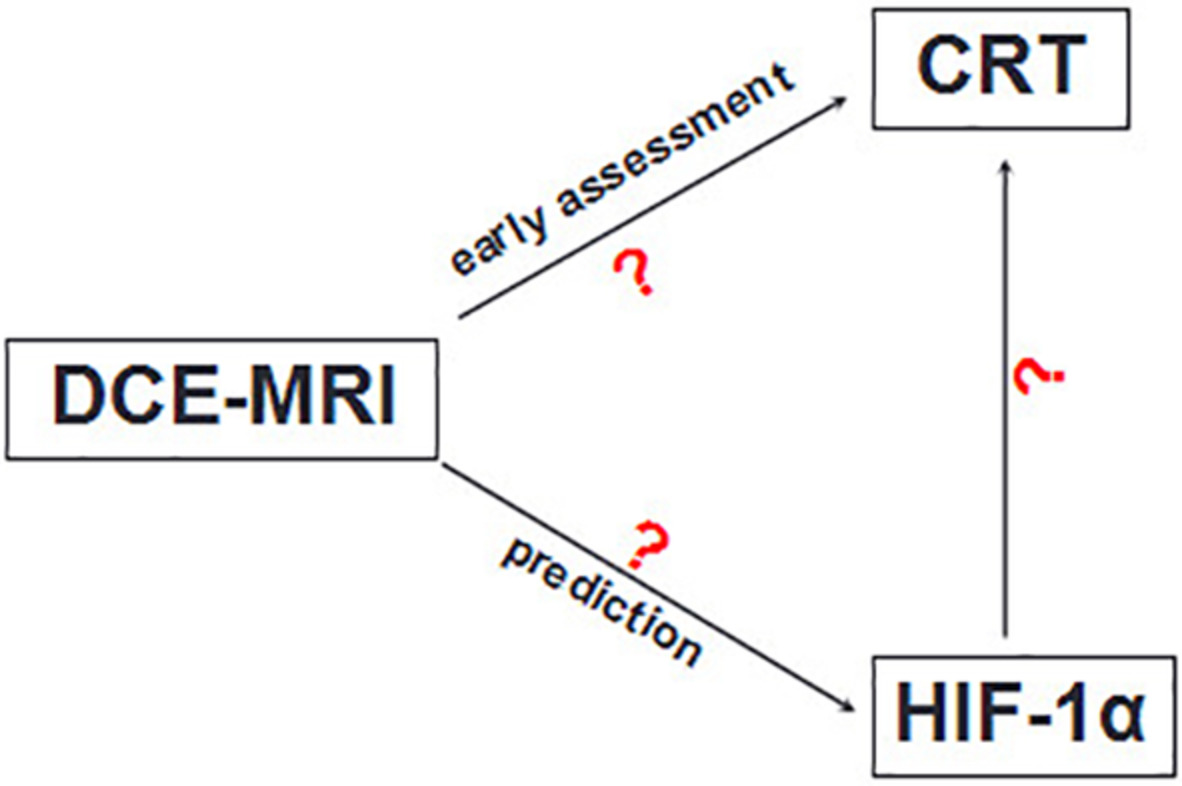
Based on the above analysis, this study aimed at detecting the role of DCE-MRI in detecting early treatment response in EC patients administered CRT. In addition, the possible associations of DCE-MRI parameters with HIF-1α expression were assessed, to offer a novel and noninvasive approach for prediction. Moreover, the relationships among DCE-MRI parameters, therapeutic response, and HIF-1α expression were explored.
2 MATERIALS AND METHODS 2.1 Ethics statementThe Institutional Review Board (IRB) of our hospital approved this study, and written informed consent was obtained from each participant. All experiments were performed in accordance with the ethical standards of the World Medical Association (Declaration of Helsinki).
2.2 PatientsInclusion criteria were (a) EC confirmed by endoscopic biopsy; (b) scheduled definitive concurrent CRT, without preoperative tumor-related treatment; (c) no contraindications for DCE-MRI; and (d) good quality of images, suggesting that motion artifacts were low enough to allow data analysis. Exclusion criteria were (a) previous tumor-related treatment, (b) contraindications for MRI, (c) unsuitability for CRT (n = 2), and (d) poor quality of images (n = 3). Eligible patients were enrolled from February 2018 to October 2020.
2.3 MRI examinationAll patients underwent 3.0 T DCE-MRI examination (Ingenia 3.0 T; Philips Medical Systems, Best, the Netherlands) at two time-points: pre-CRT (1 week before CRT) and 3w-CRT (3 weeks after CRT). Examination was performed in the supine position. The MRI scanning sequences included conventional T1-weighted imaging (T1WI), small field of view (FOV) and high-resolution (HR) T2-weighted imaging (T2WI), diffusion weighted imaging (DWI), and DCE imaging. Small FOV and HR T2WI scanning parameters were repetition time (TR), 2000 ms; echo time (TE), 90 ms; slice thickness, 4 mm; matrix, 232 × 232; FOV, 140 mm × 140 mm; and navigator use for respiratory triggering. DWI adopted echo-planar imaging to scan cross sections with the following parameters: TR, 250 ms; TE, 64 ms; slice thickness, 4 mm; matrix, 64 × 64; b values of 0 and 800 s/mm2, respectively). The apparent diffusion coefficients (ADC) diagram was reconstructed finally. DCE scanning comprised two parts. Before contrast injection, transverse volume sequences were obtained at two flip angles (α = 5° and 15°, respectively) to calculate T1 mapping. Then, DCE images were obtained with an axial dynamic T1-weighted 3D-fast field echo (TFE) with the following parameters: TR, 4 ms; TE, 2 ms; slice thickness, 4 mm; matrix, 172 × 172; FOV, 240 mm × 240 mm. A bolus dose of MRI contrast (Magnevist, Bayer) was injected at 0.1 mmol/kg of body weight at a rate of 2.5 ml/s with an automatic syringe pump, followed by saline flush.
2.4 MR image analysisThe dynamic data were processed with the Omni-Kinetics post-processing software (GE Healthcare), which could fit T1-weighted DCE MRI data to the Tofts linear model, and quantitative kinetic parameters (ktrans, kep and ve) were calculated. Two radiologists with 8 and 11 years of experience in digestive radiology were blinded to the treatment results and independently performed data analysis. In this study, we artificially divided esophageal lesions into upper, middle, and lower segments, and three regions of interest (ROIs) were manually outlined randomly in each segment (Figure 1). Areas of necrotic tissue, hemorrhage, calcification, and blood vessels were avoided while setting the ROIs. Finally, the averages of the three segments (totally nine ROIs) for various parameters were obtained in every patient. On T2WI, the thickened esophageal wall had a relatively higher signal intensity compared with normal esophageal tissue. The small FOV and HR T2WI could make the signal intensity contrast more obvious; in addition, DWI/ADC could further help determine the exact boundaries of the esophageal lesions for delineating ROIs in CE-T1WI (Figure 2).

Diagrammatic representation of region of interest (ROI) delineation. The esophageal lesion was artificially divided into upper, middle, and lower segments, each containing three random ROIs

Multifunctional sequences for determining the exact boundary of an esophageal lesion for ROI delineation. A middle thoracic esophageal tumor at the pre-chemotherapy (CRT) and 3w-CRT time-points with multifunctional sequences images. The small field of view (FOV) and HR T2WI increase the signal intensity of the thickened esophageal wall more obviously. In addition, DWI/ADC could further help in determining the exact boundary of the esophageal lesion for ROI delineation on CE-T1WI
2.5 Treatment protocol and therapeutic response evaluationA total of 39 EC patients underwent CRT. According to the patient's specific condition, the prescribed radiotherapy dose was 60–66 Gy (1.8–2.2 Gy/fraction, 5 fractions/week; totally 30–33 fractions). Chemotherapy was performed concurrently with radiation therapy with paclitaxel liposome at 90 mg/m2 plus nedaplatin at 40 mg/m2 for 4 weeks, and no more than 6 weeks. A month after CRT, based on combined esophageal barium swallow, chest enhancement CT and the Response Evaluation Criteria in Solid Tumors (RECIST) guideline version 1.1,25 patients were divided into the sensitive (SG) and resistant (RG) groups; in parallel, HIF-1α(+) and HIF-1α(−) groups were determined by immunohistochemistry (IHC).
2.6 Immunohistochemical analysis of HIF-1αHIF-1α was assessed in paraffin-embedded tissue samples sectioned at 5 μm. Briefly, all sections were deparaffinized, and antigen retrieval was performed under high pressure for 2 min. Nonspecific binding was blocked with serum for 15 min at 37°C. The sections were stained with primary monoclonal rabbit anti-human HIF-1α antibody (Abcam, Cambridge, UK) in a humidified chamber for 60 min at 37°C. The specimens were next stained with goat anti-rabbit secondary antibodies, in a humidified container for 30 min at 37°C. HIF-1α expression was visualized with 3, 3-diaminobenzidine (DAB) followed by counterstaining with hematoxylin. HIF-1α expression was determined by assessing the percentage of tumor cells with cytoplasmic staining, and staining intensity was evaluated with the following classification system: 0, no staining; I, staining in less than 10% of tumor cells; II, staining in 10%–50% of cells; III, staining in over 50% of cells. 0 and I were considered a negative (−) pattern, whereas II and III were positive (+) patterns.26
2.7 Statistical analysisAll statistical analyses were performed with the SPSS 23.0 statistical software (SPSS Inc., Chicago, IL). Categorical data were compared by the Fisher's exact test and Kruskal–Wallis test. The Shapiro–Wilk test was performed to determine whether quantitative parameters had a normal distribution. Normally distributed data were compared by the Student's t test; the Mann–Whitney U test was adopted for non-normally distributed data. Paired comparisons were performed by the Wilcoxon test. The diagnostic performances of these parameters in predicting treatment response or HIF-1α expression were tested by receiver operating characteristic (ROC) curve analysis. The maximal Youden index (Youden index = sensitivity + specificity – 1) was calculated to obtain a reasonable threshold. p < .05 was considered statistically significant.
3 RESULTS 3.1 DCE-MRI-derived parameters for early evaluation of patient response to CRT in EC 3.1.1 Clinical characteristics in the SG and RG groupsDemographic data of all patients are presented in Table 1. Totally 39 patients (22 males and 17 females; mean age, 66.77 years; age range, 46–82 years) were enrolled in the current study. According to RECIST guideline version 1.1, the CR and PR groups were defined as the SG, and the SD and PD groups as the RG. There were 18 males and 16 females (mean age, 66.65 ± 7.32 years) in the SG, and 4 males and 1 female (mean age, 67.6 ± 5.13 years) in the RG. No statistically significant differences were detected between the SG and RG in mean age (p = .782), gender (p = .363), pathological type (p = .701), clinical T-stage (p = .819), and N-stage (p = .397), whereas tumor location showed a significant difference (p = .016) between the SG and RG.
TABLE 1. Demographic data in the SG and RG SG (n = 34) RG (n = 5) p-value Mean age 66.65 ± 7.32 67.6 ± 5.13 .782 Gender (n%) .363 Male 18 (52.9) 4 (80) Female 16 (47.1) 1 (20) Pathological type (n%) .701 SCC 33 (97.06) 5 (100) Adenocarcinoma 1 (2.94) 0 (0) Location (n%) .016* Cervical and upper 3 (8.8) 0 (0) Cervical 2 (5.9) 0 (0) Upper 11 (32.4) 1 (20) Middle and upper 8 (23.5) 0 (0) Middle 9 (26.5) 1 (20) Lower and middle 1 (2.9) 1 (20) Lower 0 (0) 2 (40) Clinical T-stage (n%) .819 II 2 (5.9) 0 (0) III 6 (17.6) 1 (20) IV 26 (76.5) 4 (80) Clinical N-stage (n%) .397 N0 1 (2.9) 0 (0) N1 15 (44.1) 0 (0) N2 6 (17.6) 4 (80) N3 12 (35.3) 1 (20) Abbreviations: SCC, squamous cell carcinoma; SG, sensitive group; RG, resistant group. * p < .05. 3.1.2 Parameters in SG and RG at the pre-CRT and 3w-CRT time-pointsAs shown in Table 2, pre-ktrans and pre-kep were decreased significantly in the SG after 3w-CRT (p < .01), whereas only pre-kep was significantly reduced in the RG (p = .037). Pre-ktrans was also decreased in the RG at 3w-CRT, although it showed no statistically significant difference (p = .225). Although ve was increased in the RG and decreased in the SG after 3w-CRT, no statistical significance was detected (p = .319 and .48, respectively).
TABLE 2. Comparisons of parameters in SG and RG at the pre-CRT and 3w-CRT time-points SG (n = 34) RG (n = 5) Pre-CRT 3w-CRT p Pre-CRT 3w-CRT p ktrans 0.47 ± 0.09 0.27 ± 0.09 <.01** 0.27 ± 0.04 0.23 ± 0.08 .225 kep 3.02 ± 0.91 2.17 ± 0.74 <.01** 2.78 ± 1.06 1.72 ± 0.95 .037* ve 1.86 ± 0.92 1.72 ± 0.84 .48 1.46 ± 0.56 1.75 ± 0.78 .319 Abbreviations: 3w-CRT, after 3 weeks of CRT; kep, reverse trans-vascular transfer rate constant in min−1; ktrans, volume transfer constant in min−1; Pre-CRT, 1 week before CRT; RG, resistant group; SG, sensitive group; ve, extravascular extracellular volume fraction. * p < .05, ** p < .01. 3.1.3 Changes in parameters between the SG and RG at the pre-CRT and 3w-CRT time-pointsAs shown in Table 3, pre-ktrans was higher in the SG compared with the RG (p < .01), and absolute Δktrans was reduced more substantially in the SG compared with the RG. No statistically significant differences were detected between the SG and RG in post-ktrans (p = .473), pre-kep (p = .579), post-kep (p = .226), Δkep (p = .685), pre-ve (p = .475), post-ve (p = .914), and Δve (p = .38). According to ROC analysis, Δktrans was the best parameter for early distinction of SG from RG; at a threshold of 0.4416, its sensitivity was 97.1%, with a specificity of 80.0% (AUC = 0.929; Figure 3).
TABLE 3. Comparisons of parameters between the SG and RG at the pre-CRT and 3w-CRT time-points Parameters SG (n = 34) RG (n = 5) p Pre-ktrans 0.47 ± 0.09 0.27 ± 0.04 .01* Post-ktrans 0.27 ± 0.09 0.23 ± 0.08 .473 ∆K trans −0.2 ± 0.11 −0.03 ± 0.06 .002** Pre-Kep 3.02 ± 0.91 2.78 ± 1.06 .579 Post-Kep 2.17 ± 0.74 1.72 ± 0.95 .226 ∆Kep −0.87 ± 0.91 −1.05 ± 0.76 .685 Pre-Ve 1.86 ± 0.92 1.46 ± 0.56 .475 Post-Ve 1.72 ± 0.84 1.75 ± 0.78 .914 ∆Ve −0.11 ± 0.96 0.29 ± 0.56 .38 Abbreviations: Post-X, X acquired after 3 weeks of CRT; Pre-X, X acquired 1 week before CRT; RG, resistant group; SG, sensitive group; ∆X, changes in X. * p < .05, ** p < .01.
Receiver operating curve (ROC) curve for Δktrans. Δktrans was the best parameter in early distinction of SG from RG with 97.1% sensitivity, 80.0% specificity, and an AUC of 0.929
3.2 DCE-MRI-derived parameters for predicting HIF-1α(−) and HIF-1α(+) EC patients 3.2.1 Clinical characteristics of HIF-1α(−) and HIF-1α(+) EC patientsThe clinical data of the HIF-1α(−) and HIF-1α(+) groups in EC patients are presented in Table 4. Totally 24 patients (12 males and 12 females; mean age, 66.33 years; age range, 46–82 years) were enrolled in this study. According to IHC analysis, the patients were divided into the HIF-1α(−) and HIF-1α(+) groups, respectively. There were 5 males and 8 females (mean age, 64.0 ± 7.00 years) in the HIF-1α(−) group, and 7 males and 4 females (mean age, 69.09 ± 6.98 years) in the HIF-1α(+) group. No statistically significant differences were detected between the two groups in mean age (p = .11), gender (p = .219), pathological type (p = .358), location (p = .096), clinical T-stage (p = .649), and N-stage (p = .665).
TABLE 4. Clinical characteristics of HIF-1α(−) and HIF-1α(+) EC patients HIF-1α(−) HIF-1α(+) p-value Mean age 64 ± 7 69.09 ± 6.98 .11 Gender (n%) .219 Male 5 (38.5) 7 (63.6) Female 8 (61.5) 4 (36.4) Pathological type (n%) .358 SCC 12 (92.31) 11 (100) Adenocarcinoma 1 (7.69) 0 (0) Location (n%) .096 Cervical and upper 3 (23.1) 0 (0) Cervical 1 (7.7) 0 (0) Upper 3 (23.1) 3 (27.3) Middle and upper 2 (15.4) 3 (27.3) Middle 4 (30.8) 3 (27.3) Lower and middle 0 (0) 1 (9.1) Lower 0 (0) 1 (9.1) Clinical T-stage (n%) .649 III 2 (15.4) 1 (9.1) IV 11 (84.6) 10 (90.9) Clinical N-stage (n%) .665 N1 6 (46.2) 4 (36.4) N2 3 (23.1) 3 (27.3) N3 4 (30.8) 4 (36.4) Abbreviation: SCC, squamous cell carcinoma. 3.2.2 Comparisons of parameters in the HIF-1α(−) and HIF-1α(+) groups at pre-CRT and 3w-CRTAs shown in Table 5, both pre-ktrans and pre-kep were decreased significantly in the HIF-1α(−) group compared with the 3w-CRT (p < .01). Pre-ktrans was reduced significantly in the HIF-1α(+) group at 3w-CRT (p < .01). Although pre-kep was decreased in the HIF-1α(+) group at 3w-CRT, statistical significance was not reached (p = .066). Meanwhile, ve was increased in the HIF-1α(−) group and decreased in the HIF-1α(+) group at 3w-CRT, but with no significant differences (p = .432 and .508, respectively).
TABLE 5. Comparisons of parameters in the HIF-1α(−) and HIF-1α(+) groups at the pre-CRT and 3w-CRT time-points HIF-1α(−) (n = 13) HIF-1α(+) (n = 11) Parameters Pre-CRT 3w-CRT p Pre-CRT 3w-CRT p ktrans 0.48 ± 0.1 0.27 ± 0.1 <.01** 0.37 ± 0.07 0.23 ± 0.06 <.01
Comments (0)