Solid-organ transplant recipients have an increased risk of contracting diseases that are preventable through vaccination.1 Much emphasis has been placed on ensuring completion of pretransplantation immunization, because the immunosuppressive therapy that prevents graft rejection may decrease the immune response to vaccines.1 The current Covid-19 pandemic has presented unparalleled challenges; transplant recipients were recognized early on as being at particular risk.2,3 As the pandemic has evolved, concerns about the fates of solid-organ transplant recipients who become infected have increased.
After vaccines became available, it was hoped that solid-organ transplant recipients would have adequate immune responses to them. However, early prospective cohort studies showed that two doses of messenger RNA (mRNA)–based SARS-CoV-2 vaccines did not induce an immune response that was sufficient to protect most of these patients.
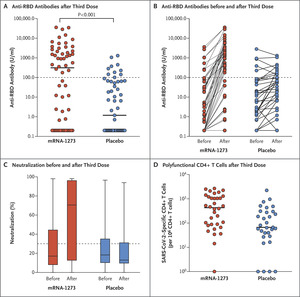
Case series and nonrandomized studies of a third dose of Covid-19 vaccines have suggested that an additional dose may produce an adequate or even robust response in most transplant recipients.4 However, randomized, controlled trials have been lacking. In a letter published today in the Journal, Hall et al.5 report on the immunogenicity and safety of a third dose of the mRNA-1273 vaccine (Moderna) given to organ transplant recipients 3 months after the first two doses. An anti–receptor binding domain (RBD) antibody level greater than 100 U per milliliter was the primary outcome, since it has been found to correlate with 50% in vitro virus neutralization. On the basis of this measure, a third dose was effective: 33 of 60 patients (55%) who received mRNA-1273 and 10 of 57 patients (18%) who received placebo had an anti-RBD antibody level above the threshold of 100 U per milliliter. In addition, the “mean fold change” in anti-RBD antibody level in the mRNA-1273 group was 75 times that in the placebo group (see Fig. S2 in the Supplementary Appendix of their letter, available at NEJM.org). Finally, there was modest evidence that a SARS-CoV-2–specific T-cell immune response occurred in the mRNA-1273 group. Together, these results provide convincing evidence of enhanced vaccine efficacy in transplant recipients, for whom great concern has been raised about a weak or even negligible immune response after the standard two doses of mRNA vaccine.
Adverse events, mainly local reactions, were mild but were more common with mRNA-1273 than with placebo. However, no hospitalizations were reported among the patients who received the booster dose of mRNA vaccine. In addition, no cases of organ rejection — something that is of great concern to transplant recipients — were reported after the booster dose. Overall, at this juncture, the benefit of third-dose vaccination, at least with the mRNA-1273 vaccine, appears to outweigh the risks.
The community of transplant recipients and professionals is eager for guidance and, possibly, for approval of a booster dose. But can one generalize from this small trial? There was some imbalance between the vaccine and placebo groups — for example, in the type of transplant, with fewer lung transplants and more abdominal organ transplants in the vaccine group than in the placebo group. Although antibody levels increased impressively after the third dose of mRNA-1273, trial follow-up was short-term. Continued monitoring of the participants in this trial and of those in prospective nonrandomized studies will be important. Although some may infer from these data that solid-organ transplant recipients should routinely receive a third vaccine dose, additional randomized trials will be key to learning how to better care for solid-organ transplant recipients during this pandemic.

Comments (0)