
Remember me




Correction: Rheumatol Ther (2025) 12:173–202 https://doi.org/10.1007/s40744-024-00736-4
In the sentence beginning ‘Median persistence (Kaplan–Meier) and effectiveness…’ of the Methods section in Abstract, the text ‘(Kaplan–Meier)’ should have read ‘(Kaplan–Meier, log rank test)’.
Few terms were missing in the Results section of the Abstract and it was incorrect as
‘Results: In patients prescribed UPA, 41.3% were ≥ 65 years old, 33.8% were prescribed as first-line advanced therapy, and 27.2% were prescribed monotherapy. Persistence on UPA was 26.6 months (95% confidence intervals: 24.4, 29.9) and longest in earlier lines of therapy. The DAS28CRP(3) remission rate was 73% at 3 months, with improvements observed across lines of therapy. UPA monotherapy and combination therapy had similar persistence (27.8 [23.5, 33.4] versus 30.4 months [22.1, 35.3], p = 0.84) and effectiveness. UPA showed longer persistence than other JAKis (28.8 [25.6, 32.4] versus 17.2 months [14.9, 19.8], p < 0.001) and TNFis (26.6 [24.9, 30.8] versus 13.3 months [11.5, 14.5], p < 0.001). DAS28CRP(3) remission rates were greater at 3 months for UPA than other JAKis (75.0% versus 61.5%) and TNFis (72.7% versus 59.5%). In unmatched subgroups, compared to cycling between TNFis, switching to UPA from other JAKis or TNFis resulted in longer persistence (JAKi-to-UPA: 25.3 [16.1, not reached]; TNFi-to-UPA: 27.8 [23.2, 35.4]; TNFi-to-TNFi: 9.6 [8.4, 10.7]) and greater DAS-28CRP(3) remission rates over 9 months.’ It should have read ‘Results: In patients prescribed UPA, 41.3% were ≥ 65 years old, 33.8% were prescribed as first-line advanced therapy, and 27.2% were prescribed monotherapy. Median persistence on UPA was 26.6 months (95% confidence intervals: 24.4, 29.9) and longest in earlier lines of therapy. The DAS28CRP(3) remission rate was 73% at 3 months, with improvements observed across lines of therapy. UPA monotherapy and combination therapy had similar median persistence (27.8 [23.5, 33.4] versus 30.4 months [22.1, 35.3], p = 0.84) and effectiveness. UPA showed longer median persistence than other JAKis (28.8 [25.6, 32.4] versus 17.2 months [14.9, 19.8], p < 0.001) and TNFis (26.6 [24.9, 30.8] versus 13.3 months [11.5, 14.5], p < 0.001). DAS28CRP(3) remission rates were greater at 3 months for UPA than other JAKis (75.0% versus 61.5%) and TNFis (72.7% versus 59.5%). In unmatched subgroups, compared to cycling between TNFis, switching to UPA from other JAKis or TNFis resulted in longer median persistence (months: JAKi-to-UPA: 25.3 [16.1, not reached]; TNFi-to-UPA: 27.8 [23.2, 35.4]; TNFi-to-TNFi: 9.6 [8.4, 10.7]) and greater DAS-28CRP(3) remission rates over 9 months.’
In the sentence “DAS-28CRP(3) measures were categorized as follows: clinical remission (< 2.6), LDA (≥ 2.6 to ≤ 3.2), minimal disease activity (MDA; > 3.2 to < 5.1), and HDA (≥ 5.1) [3]’, MDA was incorrectly defined as ‘minimal disease activity’ but it should have been ‘moderate disease activity’.
In Table 1 (note ‘d’), Figs. 3, 4, 5, 6, and 7 caption, and footnotes of several Supplementary Tables, MDA was incorrectly defined as minimal disease activity. MDA has now been labeled correctly as moderate disease activity throughout.
In Fig. 1, a few of the sample sizes (n) displayed on the Sankey diagram were incorrect in the original publication and have been corrected as follows. The revised figure is displayed below.
0–< 3 months: denominator for both combination therapy and monotherapy corrected to 2623 (was 2643)
3–9 months: stopped corrected to 123 (was 40)
3–9 months: no further follow-up corrected to 369 (was 123)
Incorrect version of Fig. 1

Correct version of Fig. 1
Fig. 1
Sankey diagram of treatment patterns for patients prescribed UPA as monotherapy or in combination with csDMARDs. Data include the treatment switching patterns of all patients prescribed UPA as monotherapy or in combination with csDMARDs through 21 months. Patients who stopped using UPA entirely are labeled as stopped. Patients with no data after a given timepoint, either because they were lost to follow-up or because the next timepoint was beyond the end of the study window, are labeled as no further follow-up. csDMARDs conventional synthetic disease-modifying antirheumatic drugs, UPA upadacitinib
In the results section, there were errors in the following sentences: ‘Throughout the study, only 28.0% of UPA-treated patients reported stopping treatment. However, some patients did not report visits and/or treatment use throughout 21 months and were classified as no further follow-up until treatment use or stop was recorded. For patients that were prescribed UPA as monotherapy at index, 31.4% continued to use monotherapy through 21 months, 7.1% added on MTX or other csDMARDs at any visit, 23.9% stopped treatment, and the remainder had no further follow-up data. For patients that were prescribed UPA as combination therapy at index, 30.5% continued to use combination therapy through 21 months, 9.4% switched to monotherapy at any visit, 10.2% stopped treatment, and the remainder had no further follow-up data.’
The sentences have been corrected to: ‘Up to 21 months, only 28.0% of UPA-treated patients reported stopping treatment. However, some patients did not report visits and/or treatment use throughout 21 months and were classified as no further follow-up until treatment use or stop was recorded. For patients that were prescribed UPA as monotherapy at index, 31.4% continued to use monotherapy through 21 months, 7.1% added on MTX or other csDMARDs at any visit, 24.1% stopped treatment while still on monotherapy, and the remainder had no further follow-up data. For patients that were prescribed UPA as combination therapy at index, 30.5% continued to use combination therapy through 21 months, 9.4% switched to monotherapy at any visit, 27.2% stopped treatment while still on combination treatment, and the remainder had no further follow-up data.’
In the sentence ‘The proportion of patients in each DAS28CRP(3) category was significantly different between the UPA and other JAKi treatment groups at 3- and 9-months post-index (3 months: p < 0.001; 9 months: p = 0.027) with more patients treated with UPA in remission at these time points than patients treated other JAKis (UPA, 3 months: 75%, 9 months: 81.1%; other JAKis, 3 months: 61.5%, 9 months: 70.8%) (Fig. 5b)’, the term ‘with’ was missing. The corrected sentence should read ‘The proportion of patients in each DAS28CRP(3) category was significantly different between the UPA and other JAKi treatment groups at 3- and 9-months post-index (3 months: p < 0.001; 9 months: p = 0.027) with more patients treated with UPA in remission at these time points than patients treated with other JAKis (UPA, 3 months: 75%, 9 months: 81.1%; other JAKis, 3 months: 61.5%, 9 months: 70.8%) (Fig. 5b).’
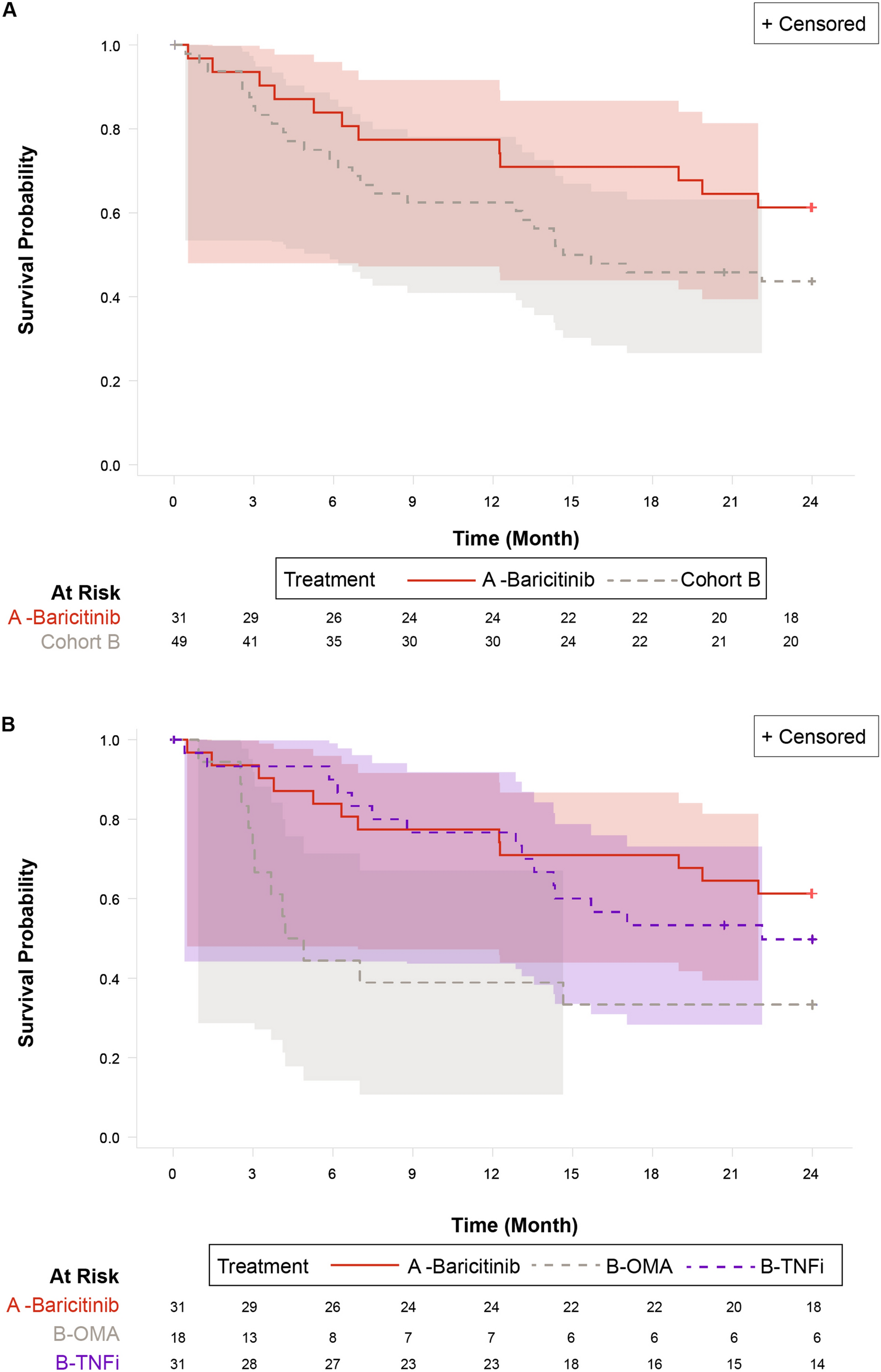
In the results section the term “longer” was missing from the sentence ‘Patients treated with UPA demonstrated significantly median time on treatment (26.6 months [95% CI 24.9, 30.8]) than patients treated with TNFis (13.3 months [11.5, 14.5]; p < 0.001) (Fig. 6a; Supplementary Table 18)’. It should have read ‘Patients treated with UPA demonstrated significantly longer median time on treatment (26.6 months [95% CI 24.9, 30.8]) than patients treated with TNFis (13.3 months [11.5, 14.5]; p < 0.001) (Fig. 6a; Supplementary Table 18).’
In the discussion section, there was an error in the following sentence that resulted in a misrepresentation of the referenced studies: “In previous OPAL studies, 17% of patients prescribed baricitinib and 16% of patients prescribed tofacitinib were in DAS28-ESR remission at index [38], with 23% of patients prescribed tofacitinib as monotherapy in remission at index [35].” The sentence has been amended to: “In previous OPAL studies, ~ 16% of bDMARD patients and ~ 17% of tofacitinib patients were in DAS28-ESR/CRP remission at index [38], with over 20% of patients prescribed tofacitinib as monotherapy in remission at index [35].”
Reference [2] was incorrect as ‘2. Ciciriello S, P Y, Tahir T, Smith T, O’Sullivan C, Leadbetter J et al. Upadacitinib vs TNFi and other JAKi treatment outcomes in Australian rheumatoid arthritis patients: descriptive comparison of persistence and effectiveness using the OPAL dataset - ACR meeting abstracts. Arthritis Rheumatol; p. 76. Available from: https://acrabstracts.org/abstract/upadacitinib-vs-tnfi-and-other-jaki-treatment-outcomes-in-australian-rheumatoid-arthritis-patients-descriptive-comparison-of-persistence-and-effectiveness-using-the-opal-dataset/.’ The corrected Reference [2] should read ‘2. Ciciriello S, Youssef P, Tahir T, Smith T, O’Sullivan C, Leadbetter J et al. Upadacitinib vs TNFi and other JAKi treatment outcomes in Australian rheumatoid arthritis patients: descriptive comparison of persistence and effectiveness using the OPAL dataset—ACR meeting abstracts. Arthritis Rheumatol; p.76. Available from: https://acrabstracts.org/abstract/upadacitinib-vs-tnfi-and-other-jaki-treatmentoutcomes-in-australian-rheumatoid-arthritis-patients-descriptive-comparison-of-persistence-and-effectiveness-using-the-opal-dataset/.’
The original article has been corrected.
Comments (0)