
Remember me




A model-based economic evaluation was performed on the cost effectiveness of the following three strategies: (1) vaccination with RZV, (2) vaccination with ZVL, and (3) no vaccination, from a societal perspective. The target population consisted of older adults aged ≥ 50 years in mainland China. The ZVL strategy included one dose, and the RZV strategy included two doses administered at months 0 and 2. Because the efficacy of both vaccines varied by vaccination age [21], we conducted analyses separately for four age cohorts, 50–59, 60–69, 70–79, and ≥ 80 years. A lifetime horizon (model terminated after everyone died or reached age 120 years) was set, since the risk of developing HZ persists throughout one’s lifetime, and there is a lifelong risk of recurrence of HZ even after recovery.
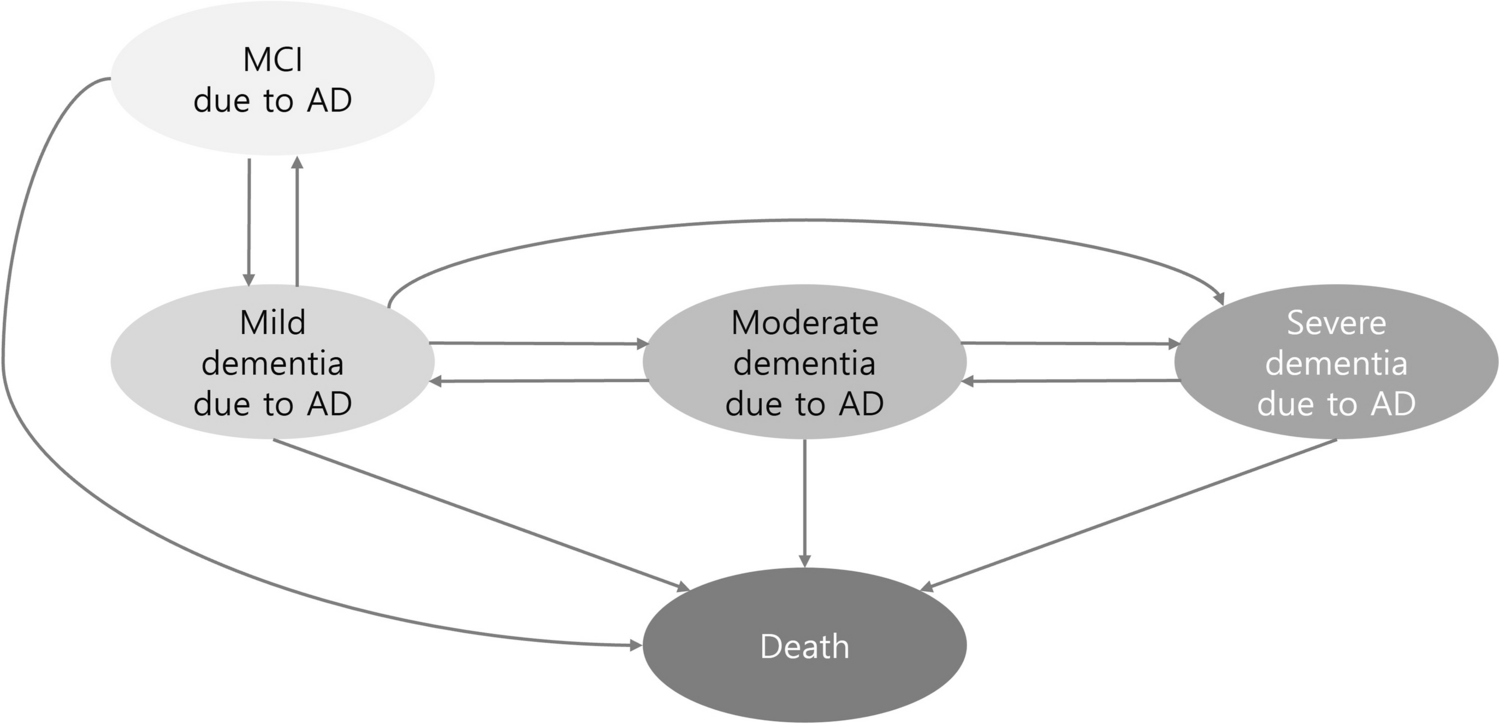
2.2 Model, Inputs and AssumptionsA validated Markov model connected with decision tree [20] was developed to quantify the cost effectiveness of RZV, ZVL, and no vaccination (Fig. 1). The Markov model consisted of eight Markov states (health, HZ with PHN, HZ with auricular, HZ with ocular, HZ with neurological, HZ without complication, HZ resolved, and death) and three decision tree nodes (initial HZ, alive, and HZ recurrent). All simulated populations were entered into the model at the healthy state and transited to other states in a 1-year cycle. Healthy individuals could develop HZ with or without complications (PHN, ocular, auricular, or neurologic diseases) or die. Patients surviving HZ would transit to the state of resolved HZ, where they might relapse into recurrent HZ or die.
Fig. 1
All model inputs were extracted from the published literature or public databases, ethical approval was not required. A literature search of Medline, Embase, and Web of Science was performed from January 2000 to May 2024. Data reported for Chinese people were preferred, otherwise, data from Asian populations were used. The inputs for demographics and epidemiology are listed in eTable 1 in the electronic supplementary material (ESM), and inputs for vaccine efficacy, utility, and costs are listed in Table 1. Efficacy of vaccine were fitted with “nls” function in R, version 4.2.2, 2022 [22], and the economic evaluation model was developed in Microsoft Excel 365 with Visual Basic for Application.
Table 1 Model inputs for vaccine efficacy, utility, and costs2.2.1 DemographicsThe data regarding age- and sex- specific population size and all-cause mortality were obtained from the national population census in 2020 [23]. The target population (adults in China aged ≥ 50 years) comprised 486.58 million in total, including 222.57 million aged 50–59 years, 147.39 million aged 60–69 years, 80.83 million aged 70–79 years, and 35.80 million aged over 80 years [23].
2.2.2 EpidemiologyThe age- and sex-specific HZ incidence was derived from a regional integrated health care database [24]. The incidence of recurrent HZ was obtained from the electronic healthcare record database of the regional community-based health information system in China [25]. The duration of HZ was assumed to be 30 days as reported in the Shingles Prevention Study (SPS) of the ZVL vaccine [11]. The age- and sex-specific proportions of PHN incidence among HZ cases were extracted from a health insurance register claims database in Taiwan, China [26]. The mean duration of PHN for HZ cases aged 50–69 years (8.3 months) and ≥ 70 years (10.9 months) was retrieved from the SPS [11]. The incidence of other complications was estimated from the health management system on epidemiologic features of HZ in China [27]. The mortality rate of HZ in Japan was applied in this study because of the absence of related data in China [28]. The mortality rate of recurrent HZ was assumed to be the same as that of initial HZ.
2.2.3 VaccineThe vaccine coverage against HZ (1.70%) was estimated from a survey in nine cities across China [15], and we assumed that the coverage of RZV and ZVL was the same. The RZV required two doses, and a model-based study in China indicated that 80% of RZV-vaccinated individuals would receive the second dose [29].
The efficacy of RZV was obtained from the Zoster Efficacy Study in Adults 50 Years of Age or Older (ZOE-50) trial [13], the Zoster Efficacy Study in Adults 70 Years of Age or Older (ZOE-70) trial [14], and a long-term follow-up (LTFU) study [30]. The long-term efficacy of RZV against HZ incidence was fitted using four functions: linear, logarithmic, exponential, and 1-minus-exponential functions. All these functions could be monotone decreasing, consistent with the process of waning efficacy. The best fitted functions were selected according to visual assessment, goodness of fit (adjusted R2), and dermatologist opinion (eFigure 1 and eTable 2 in the ESM). For vaccination at age 50–69 years, the linear function was best fitted with R2 = 0.59. The selected function was \(y= 0.9965-0.0153 \times \text\) for vaccination at age 50–69 years. For vaccination at age 70 years, the best fitted function was logarithmic and exponential. However, these two functions simulated a particularly slow waning rate of efficacy. Therefore, the linear function was used according to dermatologist opinion, and the final functions was \(y= 0.9651-0.0226 \times \text\) for vaccination at age ≥ 70 years. The efficacy of RZV against PHN in HZ cases was not considered in our study, because the efficacy against PHN was lower than the efficacy against HZ incidence [13, 14], meaning RZV had no additional efficacy against PHN incidence among HZ cases who were vaccinated. In clinical practice, it was possible that patients might receive one dose. Therefore, the efficacy of one-dose RZV was considered in our study. However, few participants received only one-dose RZV and the mean follow-up period was < 3 months in the ZOE studies [13, 14]. A post-hoc analysis [31] using these limited clinical data evaluated the initial efficacy of one-dose RZV, and the initial efficacy of one dose was 0.9077 in patients aged 60–69 years and 0.7063 in patients aged ≥ 70 years [31]. Due to lack of long-term efficacy data for one-dose RZV, we conservatively assumed that the efficacy waning rate (slope) for one dose was twice as much as for two doses, yielding efficacy functions for a single RZV dose.
The efficacy of ZVL was modeled from the SPS [11], the Short-Term Persistence Substudy (STPS) [32], and the Long-Term Persistence Substudy (LTPS) [12]. As trials showed ZVL had additional efficacy against PHN in HZ cases, this was considered in our study. The long-term efficacy of ZVL against HZ incidence and PHN incidence were fitted separately using the same four function mentioned above. The selected functions were \(y=1- }^-0.9656)}\) for efficacy against HZ, and \(y= 0.7577-0.046 \times \text\) for efficacy against PHN. The vaccine’s efficacy against PHN incidence included two aspects: first, by reducing HZ incidence, the vaccine indirectly lowered PHN incidence (since fewer HZ cases lead to fewer PHN cases); second, it directly reduced PHN incidence among vaccinated individuals who developed HZ. The efficacy for PHN incidence reported in clinical trials included both indirect and direct effects on HZ incidence. In order to estimate the direct efficacy for PHN incidence among HZ cases, we used the validated equation [33] \(x=\frac}_}-}_}}}_}}\), where \(x\) is the efficacy for PHN incidence among HZ cases, \(}_}\) is the overall efficacy for PHN incidence reported in the trial, and \(}_}\) is the efficacy for HZ as estimated by the fitted functions above. To include the effect of age, we adjusted the vaccine efficacy on initial efficacy using age-specific risk ratios of the clinical trials [11, 34]. Lastly, it was assumed that vaccine efficacy of RZV and ZVL did not decrease below zero.
2.2.4 UtilityThe age- and sex-specific utility scores in the healthy state were obtained from the National Household Health Survey in older Chinese people [35]. The utility values of uncomplicated HZ, PHN, and ocular complications were extracted from studies on estimation of the health-related quality of life impacts of HZ and PHN [36,37,38]. The utility values of auricular complication were estimated from the average utility values for older patients with otitis media in Taiwan, China [39]. The utility values of neurologic complications were obtained from that of meningitis in a cost-effectiveness study in China [40]. It was assumed that utility values for ocular, auricular, neurologic complication states remained constant across age groups due to lack of age-specific evidence in established literature.
Moreover, a disutility due to grade 3 adverse events at injection site was included. In clinical trials of HZ vaccines, grade 3 adverse events were defined as events that prevented normal everyday activities. The risk difference of patients with grade 3 adverse events between the vaccine arm and placebo arm was 13.7% [13] for RZV and 1.4% [11] for ZVL. The disutility of a grade 3 adverse event was assumed at 0.193 ± 0.009 [41] (a shift from no problem with usual activities to severe problems with usual activities on the EQ-5D-3L instrument) and the median duration at 2 days [11].
2.2.5 CostThe vaccine cost per dose of ZVL (US$227.48) and RZV (US$195.46) in our study was the average bid-winning price across China [42]. Vaccination service cost per dose (US$3.88) was the average cost in all provinces across China [42]. The age-specific hospitalization rates of HZ were estimated from the health information systems of medical institutions [43]. The average number of outpatient visits and outpatient and inpatient costs with uncomplicated HZ were derived from a study on the disease burden of HZ [25]. Direct and indirect costs of PHN were estimated from physician reviews and patient reports from eight hospitals in China [44]. Direct and indirect costs of ocular and auricular complications were estimated from the China Health Statistical Yearbook [45], Chinese economic evaluation of eye diseases [46], and a questionnaire on hearing loss [47]. Direct and indirect costs of neurologic complications were estimated using the economic burden of patients with meningitis [48] and ischemic stroke [49] in China. Direct nonmedical costs and indirect costs per HZ case were derived from a retrospective cohort study on the HZ economic burden [50]. The costs that did not correspond to 2023 prices were inflated to 2023 using the consumer price index. All cost inputs were reported as 2023 US dollars, with Chinese yuan converted to US dollars using the 2023 exchange rate: US$1 = ¥7.05 [51]. According to the Guidelines for Evaluation of Chinese Pharmacoeconomics, costs and effectiveness were discounted at an annual rate of 5% [52].
2.3 Statistical Analysis2.3.1 Base-Case AnalysisThe outcomes comprised (i) cost, (ii) life year (LY), (iii) quality-adjusted life year (QALY), (iv) the incremental cost-effectiveness ratio (ICER), (v) net monetary benefits (NMB) and net health benefits (NHB), and (vi) health impacts on total cases of HZ, complications of HZ, and HZ-related death. An ICER was calculated as the incremental costs per additional QALY gained. NMB and NHB were obtained for each strategy by applying the following calculation: \(\text(\uplambda ) =\text\times\uplambda -\text\), \(\text(\uplambda ) =\text-\text/\uplambda\), where \(\uplambda\) was the willingness-to-pay (WTP) threshold [53].
The primary decision rule of cost effectiveness was based on ICER. When the ICER was lower than the prespecified WTP threshold, threefold gross domestic product (GDP) per capita per QALY (US$38,042.49/QALY), the strategy was considered cost effective [52]. Specifically, we first calculated the ICER for RZV and ZVL compared with no vaccination. Then, we calculated the ICER for RZV compared with ZVL.
Since ICER requires pairwise comparisons, this study involved three strategies, which need C(3,2) = 3 pairwise comparisons. In contrast, net benefit (NMB and NHB) only required a single comparison and is more straightforward for analysis, providing complementary insights. For each strategy, we calculated the net benefits and ranked them from the highest to the lowest. The strategy with the highest net benefit was considered to be the most cost-effective strategy.
2.3.2 Sensitivity AnalysesTo assess the robustness of the base-case results, sensitivity analyses were performed. The sensitivity of the results to variable variation was defined as the impact of variable variation on cost-effectiveness outcomes (ICER).
One-way sensitivity analyses were performed for all model parameters. When the 95% confidence interval (CI) of a parameter was available, its lower and upper bounds were used as the range; if not available, the minimum and maximum values of parameters from different studies were used (Table 1). The results of one-way sensitivity were presented by tornado diagrams. We defined that the results were sensitive to a study variable variation when variable variation altered the cost-effective conclusions (shifting from cost effective to not cost effective, and vice versa) or made the greatest impact on the ICER.
In two-way sensitivity analysis, we examined the joint effect of price of RZV and ZVL, the adherence rate of the second dose of RZV and its price. The results of two-way sensitivity were presented by region graph, and each region was assigned to the most cost-effective strategy. The value of variables within their joint distributions that led to changes in the cost-effective conclusions would be reported.
In probabilistic sensitivity analyses (PSA), a Monte Carlo simulation with 10,000 iterations was generated by simultaneously sampling the key model parameters from the predefined distributions. The results from PSA were used to construct (i) a cost-effectiveness scatter plane, which showing the percentage of iterations that each strategy had an ICER not exceeding WTP; (ii) a cost-effectiveness acceptability curve, illustrating the probability of each strategy being cost effective over a range of WTP values; and (iii) the expected value of perfect information (EVPI) analyses, which quantified the value of acquiring perfect information about all aspects of the decision, that is, eliminating all uncertainty [54, 55].
2.3.3 Scenario and Subgroup AnalysesTo investigate the uncertainty of economic outcomes caused by different scenarios, scenario analysis with respect to the following three conditions was conducted: (i) different adherence to second dose of RZV; (ii) different efficacy waning rate (slope) for one-dose RZV (equal to two-dose RZV, threefold to two-dose RZV); and (iii) different time horizons (10, 20, 30, and 40 years). Lastly, sex subgroup analyses were performed to investigate the uncertainty caused by the subpopulation.
2.4 Validation of the ModelInternal and external validity were performed to evaluate the accuracy of model simulations. In internal validity, the inputs, outputs, equations, and programming codes in the model were inspected, and two different types of software (Microsoft Excel 365 and TreeAge Pro 2022) were used to construct the model. In external validity, the simulated lifetime risk of HZ among people with no vaccination in our model was compared with results reported in published literature.
Comments (0)