The COVID-19 pandemic, caused by the coronavirus SARS-CoV-2, has posed significant challenges to global public health. Beyond the commonly recognized symptoms of fever, cough, and respiratory distress, emerging evidence highlights the virus's distinctive impact on sensory perceptions, particularly taste and smell [1].
A notable and clinically relevant manifestation of COVID-19 is the alteration or loss of taste and smell, medically known as ageusia and anosmia, respectively [2, 3]. Similar to some respiratory viruses, SARS-CoV-2 exhibits a unique affinity for the epithelium of taste buds, which plays a crucial role in taste perception. This characteristic has spurred a growing body of research and clinical observations regarding the prevalence, duration, and implications of taste disturbances in COVID-19 patients [4].
Reports from France, Italy, Germany, China, South Korea, and the UK indicate that a significant number of confirmed COVID-19 patients have experienced ageusia (loss of taste), and a potential mechanism for SARS-CoV-2-induced ageusia has been suggested [5]. Furthermore, increasing evidence suggests that some patients experience ageusia in the absence of other symptoms [6]. In various populations, 2–4% of individuals are affected by lifelong taste disorders (ranging from dysgeusia to ageusia), with influenza and the common cold being two of the most frequent etiological factors [7].
Post-infection taste disorders typically occur following an upper respiratory tract infection (URTI) caused by different viral infections. Females are more frequently affected, and post-URTI complications are commonly reported between the ages of 40 and 80 [8]. Understanding the mechanisms behind altered taste sensation in COVID-19 is crucial for several reasons. Firstly, ageusia and dysgeusia often serve as early indicators of SARS-CoV-2 infection, aiding in the timely identification and isolation of cases. Additionally, the persistence of these sensory disruptions post-recovery raises important questions about the virus's long-term effects on neural and sensory pathways [9].
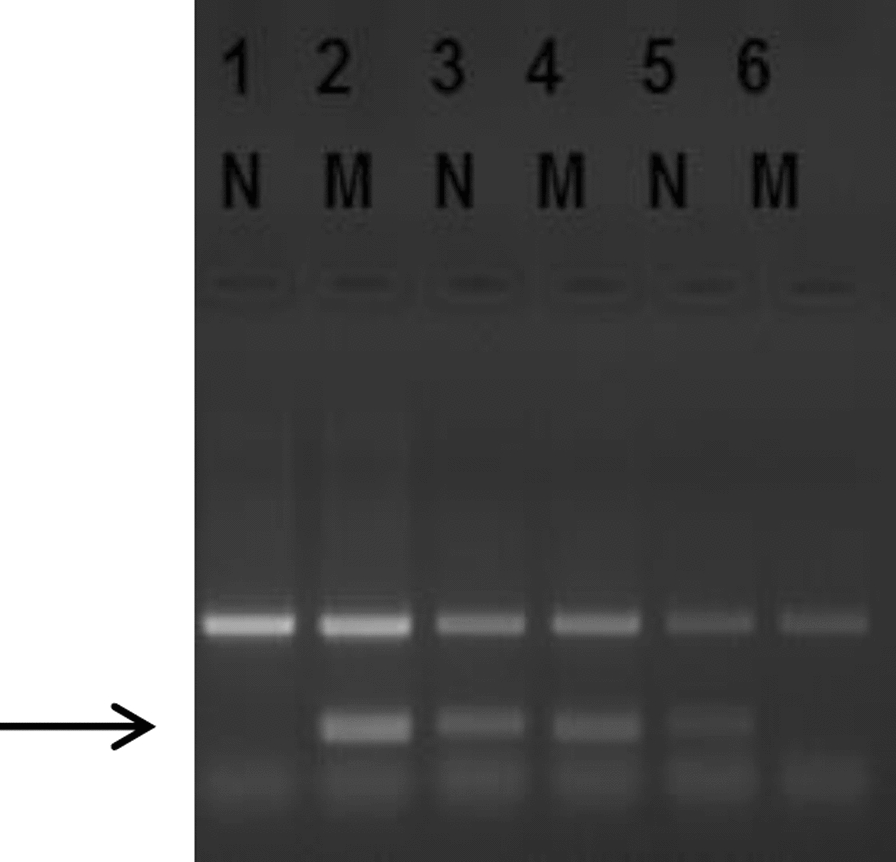
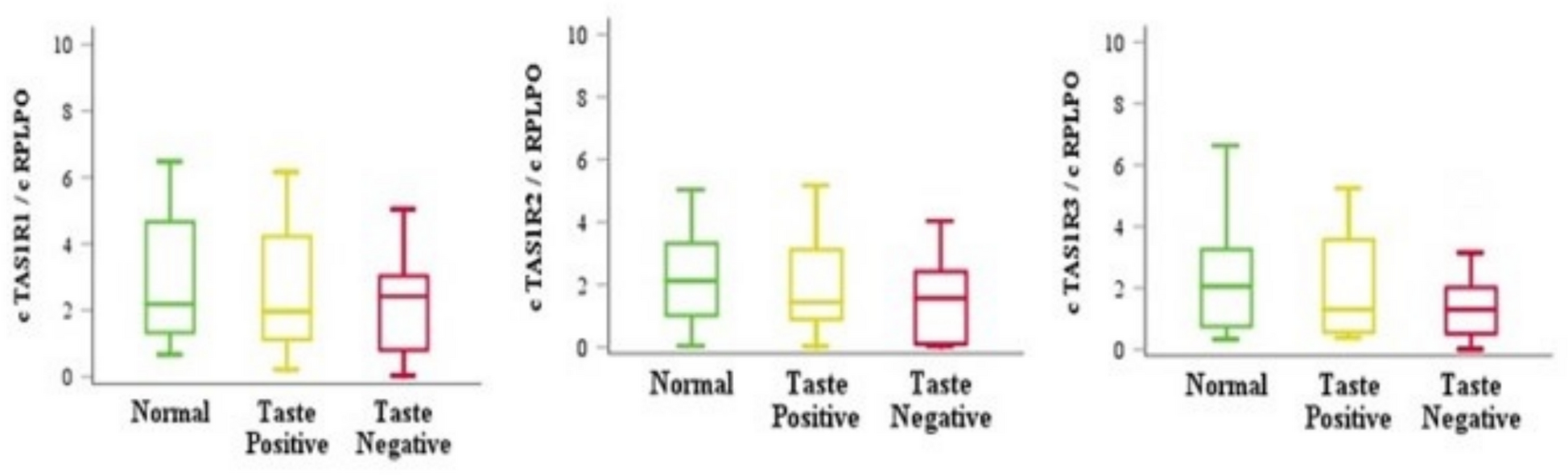
The TAS1R sweet taste receptors belong to a group of G protein-coupled receptors that have been reported to be disrupted in COVID-19 patients [10, 11]. These receptors function in detecting tastes such as umami and sweet by forming different heterodimeric complexes: TAS1R1/TAS1R3 for umami and TAS1R2/TAS1R3 for sweet. Type II receptors also function as monomers and contribute to bitter taste perception. When taste substances bind to these receptors, a secondary signaling pathway is activated, leading to increased intracellular calcium in taste receptor cells (TRCs), which then communicate with the gustatory cortex via the nervous system [12].
Some studies indicate a relationship between taste gene expression and COVID-19 infection. For example, Qendresa et al. [13] revealed that taste gene expression is decreased in response to COVID-19 infection, especially with the Delta variant. Barham et al. [14] also indicate a relationship between Bitter Taste Receptor Phenotype and outcomes of COVID-19 infection. In another study, Jain et al. [15] revealed that viral load has a significant relationship with COVID-19 infection. Patients with olfactory and taste dysfunction had higher viral load. These studies indicate that genetics and gene functions have an important role in olfactory and taste dysfunction.
This study is the first evaluation in the Iranian community to investigate the expression of TAS1R1, TAS1R2, and TAS1R3 genes on the sense of taste in COVID-19 patients. It examines the clinical implications, potential mechanisms, and avenues for future research. Unraveling the complexities of these sensory disturbances is essential for improving diagnostic strategies, patient care, and our broader understanding of the virus's pathophysiology.




Comments (0)