Study design
A comparative cross-sectional study was conducted in the period from August 2022 to August 2023 in the Neonatal Intensive Care Units, Children’s Hospital, Ain Shams University, Cairo, Egypt.
Forty-two term and late-preterm neonates were enrolled with symptoms, signs, and laboratory findings of neonatal indirect hyperbilirubinemia, and neonates were divided into 2 groups by purposive sampling method according to the inclusion and exclusion criteria: group 1 involved 22 term and late-preterm infants (GA: 35–366/7 weeks) with indirect hyperbilirubinemia who required phototherapy or exchange transfusion due to hemolytic disease of the newborn.
Whereas 20 term and late-preterm infants were enrolled in group 2 with hyperbilirubinemia due to a non-hemolytic cause, infants of smoking mothers, those on invasive ventilation or respiratory complications, infants with direct hyperbilirubinemia, those with hypoxic ischemic encephalopathy, and infants with congenital malformations or cardiovascular disease were excluded from the study; also, infants whose parents refused to consent were excluded.
Informed consents were taken from parents of all participating neonates after description of the study and its aim. The patients had the right to withdraw from the study at any time without giving any reasons. This study was approved by the Ethical Committee of Ain Shams University (FWA 000017585, FMASU M S 162/2019).
Blood carboxyhemoglobin measurement
COHb level was measured at the same time as bilirubin measurement and expressed as a percentage of total Hb by blood gas analyzer (cobas b 221) that was supported by a CO-oximetry panel using a spectrophotometric method developed by Roche Company [6]. COHb levels were measured on admission and after 48 h with follow-up labs in both groups including complete blood count (CBC), reticulocytic count, total serum bilirubin on admission and after 48 h, blood group typing of the baby and the mother, direct Coombs test, and lactate dehydrogenase test.
The amount of blood withdrawn was about 1 cm collected in heparinized tube for COHb measurement, and other labs were withdrawn with routine labs from the patients. The patients were held by the primary caregiver if available or swaddled by the nurse to counteract the pain.
The infants were divided into two groups according to at least two hemolysis findings, namely Hb or Hct, under the 10th percentile for age-specific Hb or Hct [7], a significant decrease in Hb or Hct, reticulocytosis, increased LDH [8], and/or positive direct Coombs test.
For all newborns, phototherapy and exchange blood transfusion (EBT) were administered in agreement with the AAP (American Academy of Pediatrics) guidelines [9]. Infants with TSB 2–3 mg/dL less than the level of phototherapy were considered near the level of phototherapy and were admitted receiving phototherapy as treatment. In addition, attention was taken to infants whose level of TSB was close to the level of exchange transfusion (2–3 mg/dL) and were considered near the level of exchange transfusion, and close monitoring was offered [10].
Sample size
In purposive sampling using PASS II program for sample size calculation, at least 20 patients in each group achieve 100% power to detect difference of 1.1 of COHb between null hypothesis that both group means are 2.4 and alternative hypothesis that mean of group I (hemolysis) is 1.4 with SD of 0.7 and 0.2 and at significance level 0.05 using two-sided T-test.
Statistical analysis
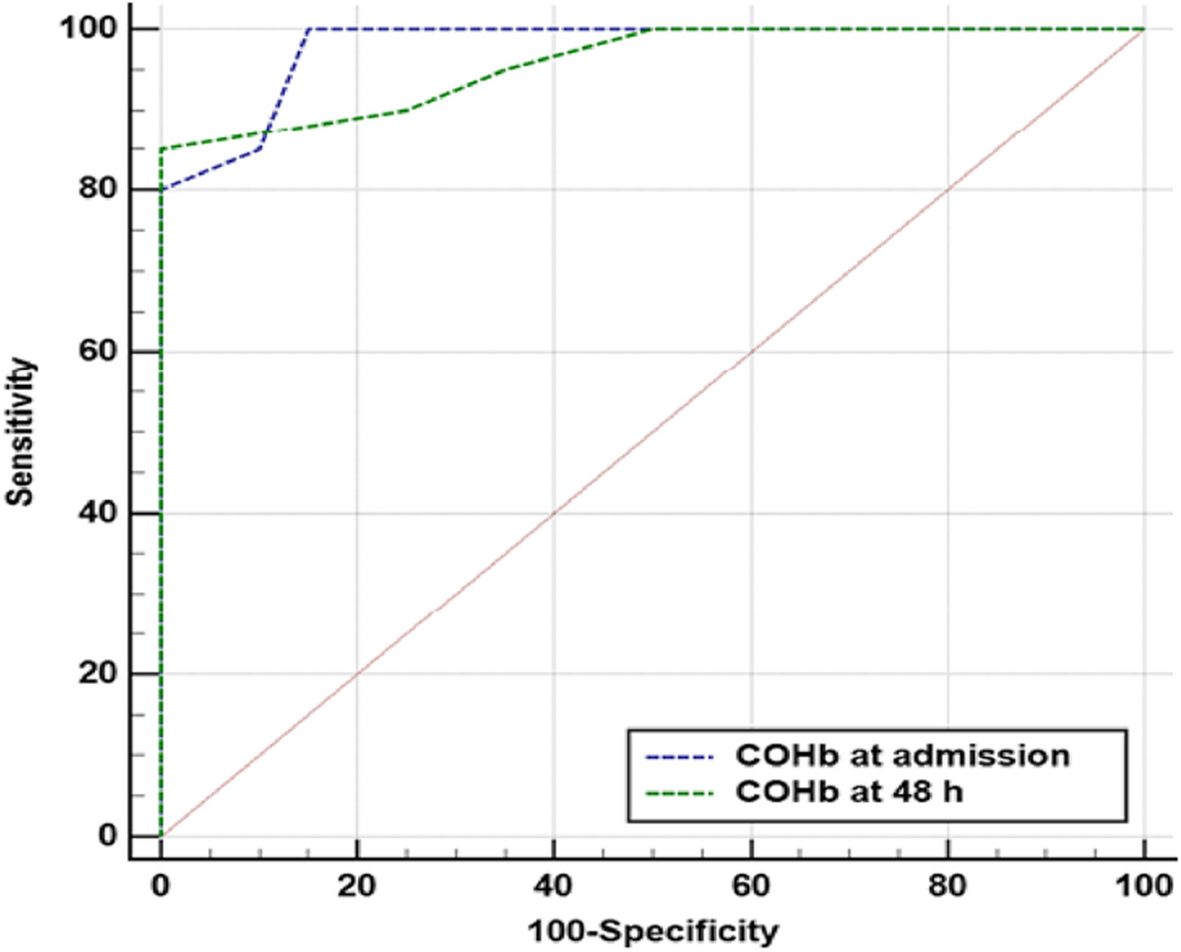
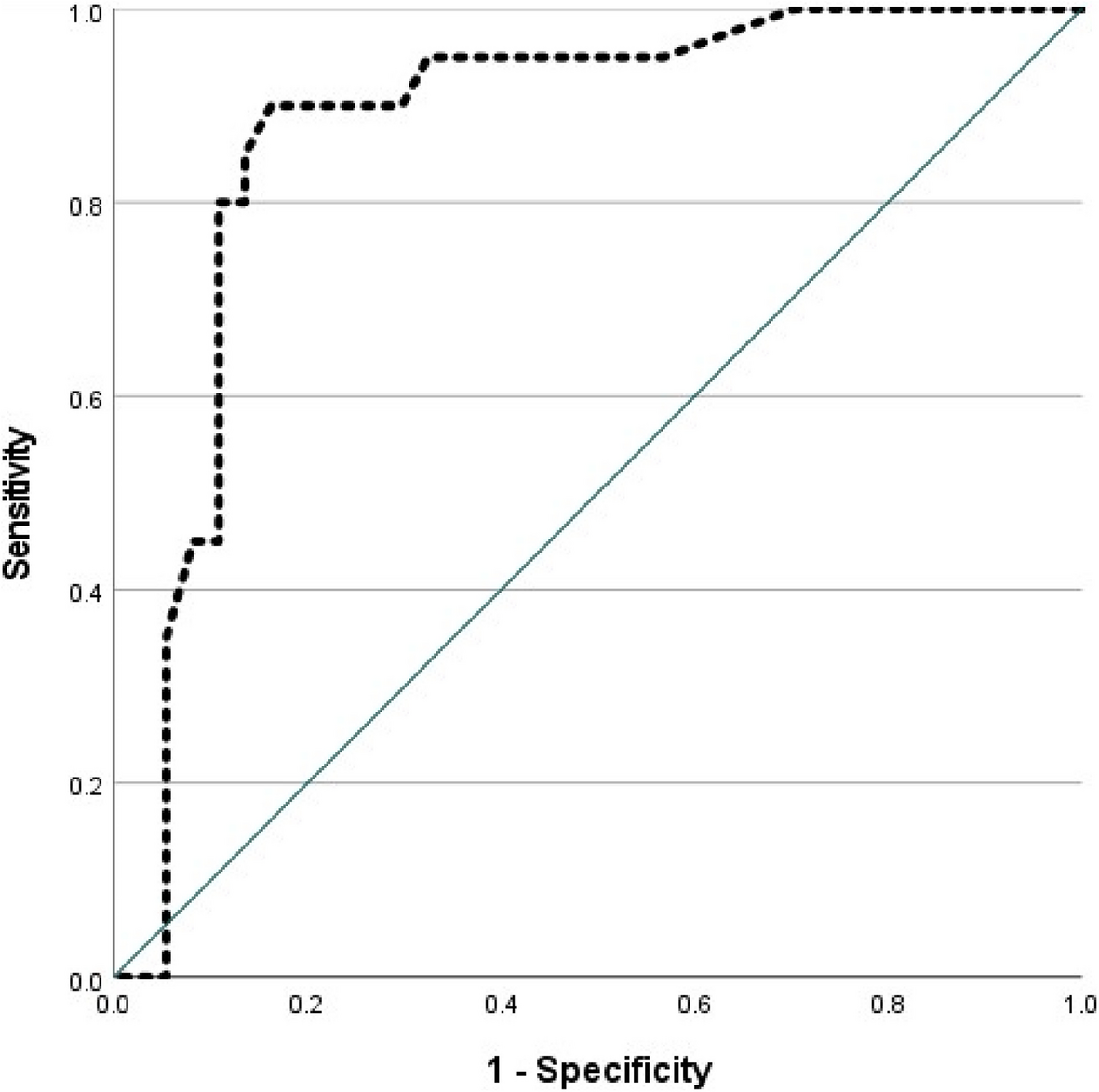
Data were analyzed using IBM© SPSS© Statistics version 26 (IBM© Corp., Armonk, NY, USA). Numerical variables were presented as mean and SD, and inter-group differences were compared using the unpaired t-test. P-values < 0.05 were considered statistically significant; categorical variables were presented as numbers and percentages, and differences were compared using the Pearson chi-squared test or Fisher’s exact test. Correlations between numerical variables were tested using the Pearson correlation. Receiver-operating characteristic (ROC) curve analysis was used to examine the diagnostic value of COHb.


Comments (0)