
Remember me



This was a cross-sectional, quantitative study approved by the Indiana University (IU) School of Medicine Institutional Review Board (#22966).
Participants and proceduresA list of eligible patients was derived from an internal clinical registry and the eligibility of each participant was verified by confirming at least one parent was English speaking and their child had completed rGS at less than 1 year of age between July 1, 2022 and May 31, 2024, via examination of the electronic medical record (EMR). All data was recorded in Research Electronic Data Capture (REDCap) (Harris et al. 2009, 2019). Additional information collected and/or confirmed from the EMR included name, date of birth, parent phone number, sex at birth, number of postnatal visits with a genetics provider, rGS results, mortality status of the infant, and level 3 Botto classification of the infant’s CHD (e.g., LVOTO, conotruncal, septal) (Botto et al. 2007).
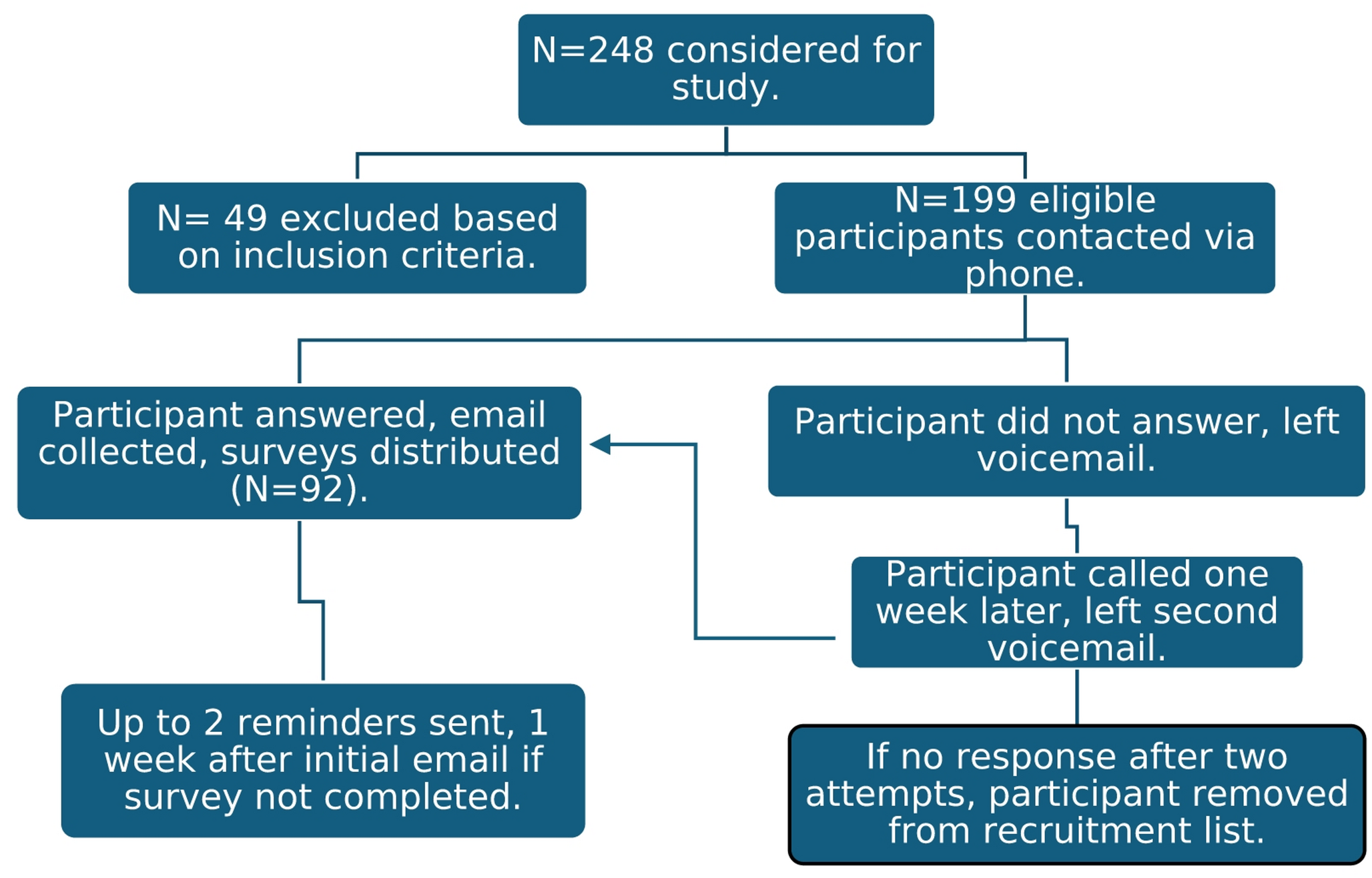
Due to institutional IRB requirements, eligible participants were first contacted by telephone to determine if they were interested in learning more about the study and willing to share their email address. Those who were able to be reached and agreed were sent an email with more information and a link to the survey. For those who could not be reached, a voicemail was left, and they were called again one week later if they did not respond to the initial voicemail. If after two attempts the participant could not be reached, they were removed from recruitment. Participants who were emailed a survey but did not complete it within 7 days were sent up to 2 automated REDCap email reminders, one week apart. This process, including number of participants ultimately sent a survey, is summarized in Fig. 1. All participants were initially contacted between July 9, 2024, and August 16, 2024. The study closed to participation on August 30, 2024, 2 weeks after the final reminder email was sent.
Fig. 1 Survey
SurveyThe survey included questions to obtain demographic (level of education, age, gender, race, and ethnicity) and family-based (relationship of the parent/guardian to the child, primary medical coordinator status, the number of additional children under the care of the parent, and family history of CHD) information. The remaining questions consisted of the adapted GEmS (McConkie-Rosell et al. 2019). Nine questions (1, 7, 9, 11, 12, 14, 17, 18, 28) were altered slightly to reflect that rGS had already taken place, for example by changing words/phrases like “will you feel” to “did you feel.” This measure consists of four subscales: ‘Meaning of a Diagnosis’ (8 questions), ‘Emotional Management’ (8 questions), ‘Seeking Information and Support’ (7 questions), and ‘Implications and Planning’ (6 questions). The possible responses for each question were on a Likert scale of 1 = not important/well/certain/at all to 7 = very important/well/certain/much (see Appendix Fig. 1 for the survey codebook for additional details).
Data analysisThe score for each subscale was obtained by summing the Likert values (1–7) for each participant’s response. A total empowerment score was then calculated by combining the scores within each subscale.
To standardize the sub-scales for data analysis and create the participant empowerment profiles, we converted the raw subscale scores of each participant into standardized Z-scores by subtracting the mean for each sub-scale and dividing by the standard deviation of the sub-scale. Each participant was coded as having a positive Z-Score or a negative Z-Score for each sub-scale to create an empowerment profile. This method was adapted from McConkie-Rosell et al., where the names for the empowerment profiles were also derived (i.e., Confident Realist, Resigned Acceptor) (McConkie-Rosell et al. 2022). Participant empowerment profiles were determined based on the pattern of positive or negative Z-Scores of each subscale (Table 1) in the following order: Meaning of a Diagnosis, Emotional Management, Seeking Information and Support, and Implications and Planning. Empowerment Profiles included ‘Disengaged or Overwhelmed’ (-, -, -, -), Resigned Acceptor (-, +, -, -), Confident Realist (+, +, +, -), and Engaged but Worried Planner (+, -, +, +), based on the analysis method of McConkie-Rosell et al. Additionally, we created empowerment profiles based on just the first two subscales (Meaning of a Diagnosis, Emotional Management) as they are more emotion-focused compared to the action scales (Seeking Information and Support, and Implications and Planning). Utilizing this method, which we call the Cheney method, we were able to categorize all participants into one of four categories based just on their emotion-focused subscales.
Table 1 Empowerment profile categorization based on gems subscale Z-scoresTo further understand parental empowerment, we summarized parent empowerment profiles according to the following variables: LVOTO CHD versus non-LVOTO CHD, number of genetics visits, and rGS result type (diagnostic versus VUS or negative). To compare empowerment profiles of parents with infants who had a diagnostic rGS result with those that had a non-diagnostic result, negative and VUS results were both considered non-diagnostic. Lastly, we collapsed the number of postnatal genetics visits into three groups of approximately 30–40% each: those with 2 (N = 1) or 3 (N = 10) genetics visits (N = 11, 29.7%), those with 4 genetics visits (N = 14, 37.8%), and those with 5 (N = 7), 6 (N = 2), 7 (N = 2), or 11 (N = 1) visits (N = 12, 32.4%). No statistical analyses were performed due to small sample sizes in some comparison groups.
Comments (0)