Hepatocellular carcinoma (HCC) and cholangiocarcinoma (CCC) are distinct, yet partially overlapping, diseases. Both come with a dismal prognosis for the majority of affected patients, although the advent of targeted therapies and checkpoint inhibitors have improved the chance of prolonged survival for some.
Hepatocellular carcinoma
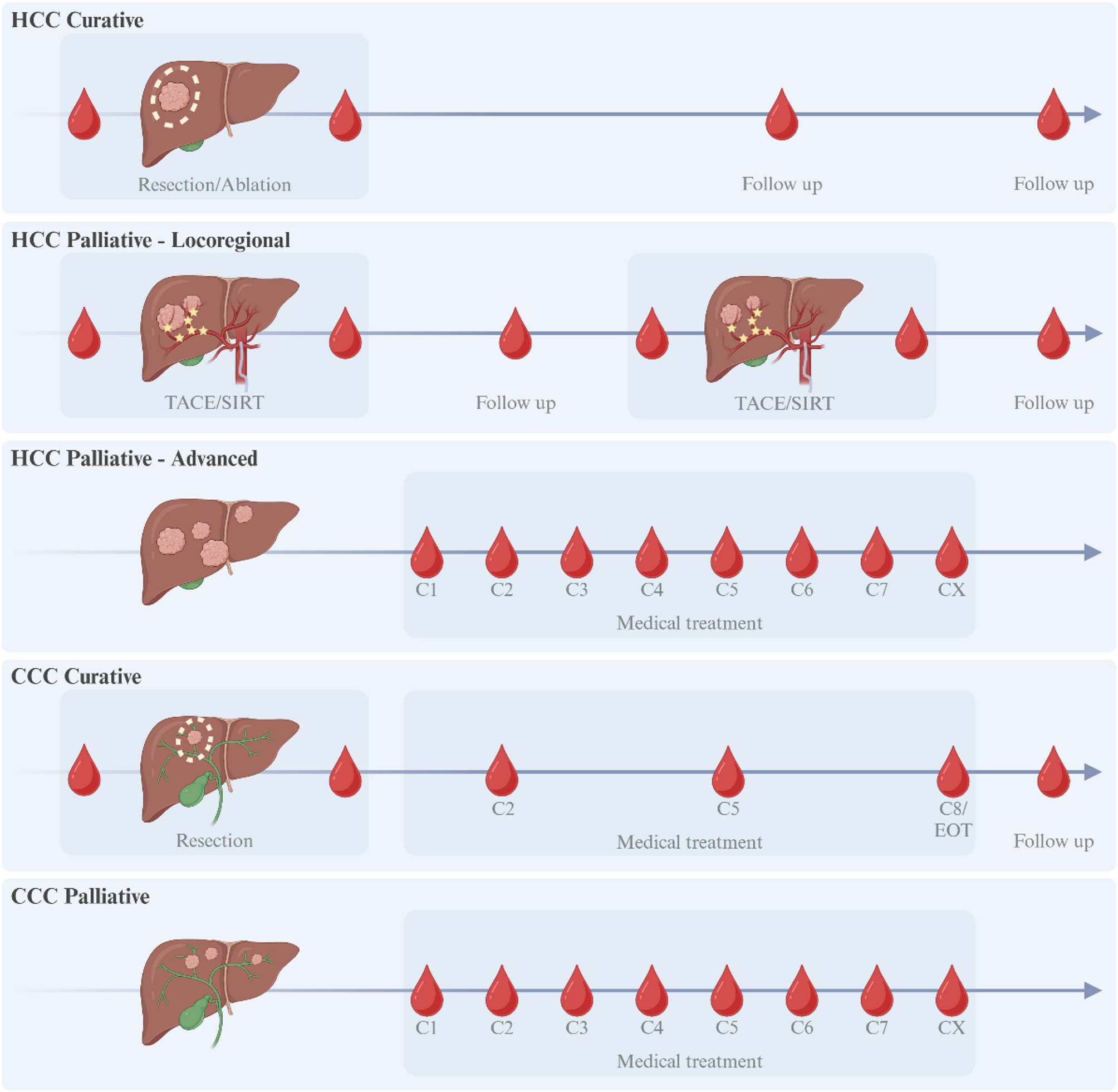
HCC comprises 75–85% of primary cancers in the liver [1] and the incidence is rising. Primary risk factors are chronic infection with hepatitis B or C virus, metabolic dysfunction-associated steatotic liver disease (MASLD) with or without diabetes mellitus type 2 and alcoholic liver disease [2]. The past decades have seen considerable epidemiological and geographical changes due to the advent of powerful antiviral therapies and lifestyle changes, but an increase in obesity and MASLD. The yearly incidence in Sweden is approximately 500 cases, and is increasing, particularly among men aged 50–65 years [3]Curative treatment includes resection, ablation or transplantation, with resection being the primary choice in patients with non-cirrhotic livers. In patients with smaller tumors (< 3 cm), resection and ablation appear to render similar survival rates, while ablation is associated with a shorter tumor free survival [4]. Even with seemingly radical resection, recurrence rates are high. Adjuvant or neoadjuvant systemic therapy does not yet have a clear place in HCC. Trials are ongoing in these settings. In disease beyond curative treatment but still liver confined, transarterial chemoembolization (TACE) or selective internal radiation therapy (SIRT) can be considered. In advanced disease, prolonged survival may be achieved with palliative systemic treatment with atezolizumab and bevacizumab in combination or tyrosine kinase inhibitors (TKI: s; sorafenib/lenvatinib), the former being superior both in terms of response rate, progression free survival (PFS) and overall survival (OS) compared to sorafenib [5]. Durvalumab and tremelimumab in combination has also been shown to be superior to sorafenib regarding response rate and OS, but not PFS [6], and ipilimumab in combination with nivolumab was superior to lenvatinib/sorafenib, with prolonged OS, in the Checkmate-9DW study [7]. These three regimens have not yet been compared head-to-head. The overall response rates with the three combination regimens were 30%, 20% and 36% respectively (atezo-bev, durva-trem, ipi-nivo) meaning that the majority of patients did not benefit from these treatments.
The pathogenicity of HCC differs between the various etiologies and give rise to different mutations and genomic alterations [8]. Viral hepatitis induced HCC tend to be more susceptible to treatment with TKI: s and PD-L1/VEGFR antibodies, but the precise biological mechanism for this has not been established [5, 9]. There is currently no established biomarker with the purpose of predicting response to immunotherapy or TKI: s in HCC.
Cholangiocarcinoma
CCC encompasses a heterogenous constellation of tumors that can arise anywhere in the biliary tree. CCCs are divided into subgroups based on their anatomical origin; intrahepatic (iCCC), perihilar (pCCC), distal (dCCC) and gall bladder (GBC). The molecular characteristics differ significantly depending on the anatomic location. The yearly incidence in Sweden is approximately 500 cases, with a slight predominance for women, in particular regarding gall bladder cancer. Several risk factors have been linked to CCC; choledochal cysts, bile duct and gall stones, primary sclerosing cholangitis (PSC), cirrhosis, liver fluke, chronic hepatitis B or C [10,11,12]. Some risk factors apply to all subtypes whereas other are more specific to one subtype and more relevant in certain geographical areas. Many risk factors share the common feature of being linked to chronic inflammation in the biliary epithelium and bile stasis [13].
Neoadjuvant chemotherapy does not yet have a place in CCC except for within clinical trials. Published data indicate a benefit in particular for patients with risk factors, but there is still a great need for prospective trials [14]. As of yet, platinum combinations have not been shown to be superior to 5-FU regimens in the adjuvant setting [15]. In the palliative setting, cisplatin combined with gemcitabine appears to be superior to other regimens in terms of both OS and PFS [16], with oxaliplatin being a viable option to cisplatin [17]. The addition of PD1/PDL1-inhibitors (pembrolizumab/durvalumab) to gemcitabine plus cisplatin further enhance treatment efficacy, though modestly [18, 19].
Isocitrate dehydrogenase 1/2 (IDH1/2) mutations and Fibroblast growth receptor 2 (FGFR2) alterations are common in intrahepatic and perihilar CCC, and targetable with specific drugs, albeit with moderate effect [20, 21]. In contrast to other solid cancers, there are however no established markers predicting response to immunotherapy, except for dMMR/MSI-H tumors [22]. In certain countries, tumor mutational burden (TMB) ≥ 10 mut/Mb is approved as a selector for immunotherapy [23, 24], although such a threshold has not been shown to be appropriate for biliary tract tumors specifically.
Less common targetable genomic mutations and alterations occur in cholangiocarcinoma, with phase II studies with small sample sizes suggesting clinical efficacy, including BRAF V600E mutations [25], HER2 amplification [26,27,28] and TRK fusion [29].
Mixed tumors
Mixed HCC-CCC are considered a separate entity. They are rare, arise in the liver, and have a particularly aggressive biology [30, 31]. There is a morphological spectrum between HCC and intrahepatic CCC, reflecting a common progenitor cell in a proportion of cases. Mixed tumors are classified as intrahepatic CCCs according to TNM8.
Objectives
The aim of the BILe duct and LIver cancer: ON-treatment Surveillance of Tumor evolution And Response to Systemic treatment (BILLIONSTARS) study is to gain a deeper understanding of the molecular biology of HCC and CCC, and to delineate clinically relevant subgroups and novel diagnostic approaches to improve personalized treatment, and, ultimately, patient outcome. In parallel, we will study how the diseases and their medical interventions affect patients’ quality of life, to improve personalized care.



Comments (0)