This study represents the largest cohort to date comparing melanoma-specific outcomes for patients having cartilage-sparing surgery of the ear with those who have cartilage resected for management of invasive melanoma. In this cohort, cartilage resection did not confer an MSS advantage and did not result in lower recurrence rates. This study suggests that the decision to perform a cartilage-sparing procedure is unlikely to compromise oncological safety and could be considered if the resulting reconstruction will provide an improved functional and cosmetic outcome to the patient.
The largest cohort to date prior to this study was by Truong et al.11, which described 156 patients with external ear melanomas, of whom 18.6% had a cartilage-sparing operation. In their cohort, there was no RFS advantage for patients who had cartilage resection, with a 5-year RFS and OS of 84.5 and 79.0% respectively, and a median follow-up of 5.5 months. However, there were several limitations of this study, including the inclusion of melanomas of the non-cartilaginous earlobe and the definition of cartilage-sparing surgery as any operation that was not described as a wedge resection in the procedure report, which is likely to overestimate the number of cartilage-sparing procedures. In our study, we defined a cartilage-sparing procedure as one where cartilage was not identified in the histological analysis, as well as the lack of description of a cartilage resection in the procedure report, which we believe to be a more accurate reflection of the true number of cartilage-sparing procedures. Likewise, in the retrospective review by Truong et al. only early-stage melanomas were included, with a median Breslow thickness of 0.86 mm, which represents a majority of patients who would ordinarily have a lower risk of recurrence and melanoma-specific mortality. The present study had a greater median Breslow thickness of 1.3 mm and 9.5% of patients had stage III disease, which represents a cohort of more advanced-stage disease than these previous studies.
To date, there have been 11 studies describing a cartilage-sparing approach to the surgical management of external ear melanoma, as summarized in Table 6.3,4,5,6,7,8,9,10,11,12,13 While only small retrospective series and case studies, they all demonstrate acceptable RFS and MSS outcomes. Of the six studies that compared cartilage resection with cartilage-sparing surgery, none reported invasion of melanoma into the cartilage.3,4,5,7,9,11 This mirrors the findings in the present study in which none of the 330 patients who had cartilage resected had evidence of melanoma invasion on histopathology, and only 6 demonstrated tumor abutting perichondrium. In these 6 patients, all but one had T4a primary lesions, which could suggest that thicker primaries may still benefit from cartilage resection. However, in this cohort, 39 patients with T4a or T4b lesions had cartilage resected, with 34 (87%) not abutting perichondrium. Therefore, despite a small number probably needing cartilage resection, the majority will achieve clear margins even for thicker primary tumors. To our knowledge, there has only been one published report of invasion into cartilage.13 In that study, Benmeir et al. report a cohort of thick melanomas in which 8/13 patients demonstrated invasion into the cartilage. Our findings, together with the majority of similar published literature, refutes this finding and suggests that the overwhelming pattern of local invasion of melanoma of the ear is a peripheral pattern along fascial planes, superficial to the cartilage, rather than penetrating deep to perichondrium.
Table 6 Previously published studies comparing cartilage resection with cartilage-sparing proceduresThe decision to resect cartilage is not solely based on oncological negative margins but should also consider patient factors such as skin quality and potential inhibitors of wound healing, such as smoking, diabetes, and immunosuppression, which may inhibit the healing of skin grafts and local flaps. Functional aspects should also be considered, including the need to wear glasses or hearing aids. This study demonstrates that a cartilage resection is not essential to achieve good oncological outcomes for patients with invasive melanomas, even if presenting with high-risk primary lesions.
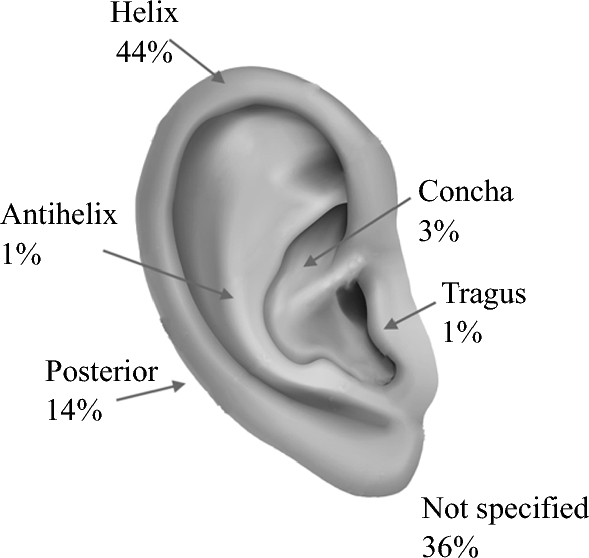
Limitations of this study include the retrospective design, which resulted in some missing data points, including 36% of patients who did not have the exact location of their lesions described in the database, clinical notes, or histological report. However, we hypothesize that the proportion of patients in each anatomical site would remain relatively similar and in keeping with the distribution of tumors described in other studies, with the helix being the most common site of occurrence.
Despite this, we report a large cohort of a relatively uncommon melanoma location. To our knowledge, this was the first study to compare melanoma-specific outcomes between patients who have cartilage resection and those who have a cartilage-sparing procedure. In addition, in this large cohort of ear melanomas, we confirm the findings of previous studies that have demonstrated no invasion beyond the perichondrium. The assumption is that cartilage-sparing procedures will lead to a more cosmetically and functionally favorable outcome. Future prospective trials including patient-reported outcomes and quality-of-life measures in these two groups would be helpful.




Comments (0)