
Remember me

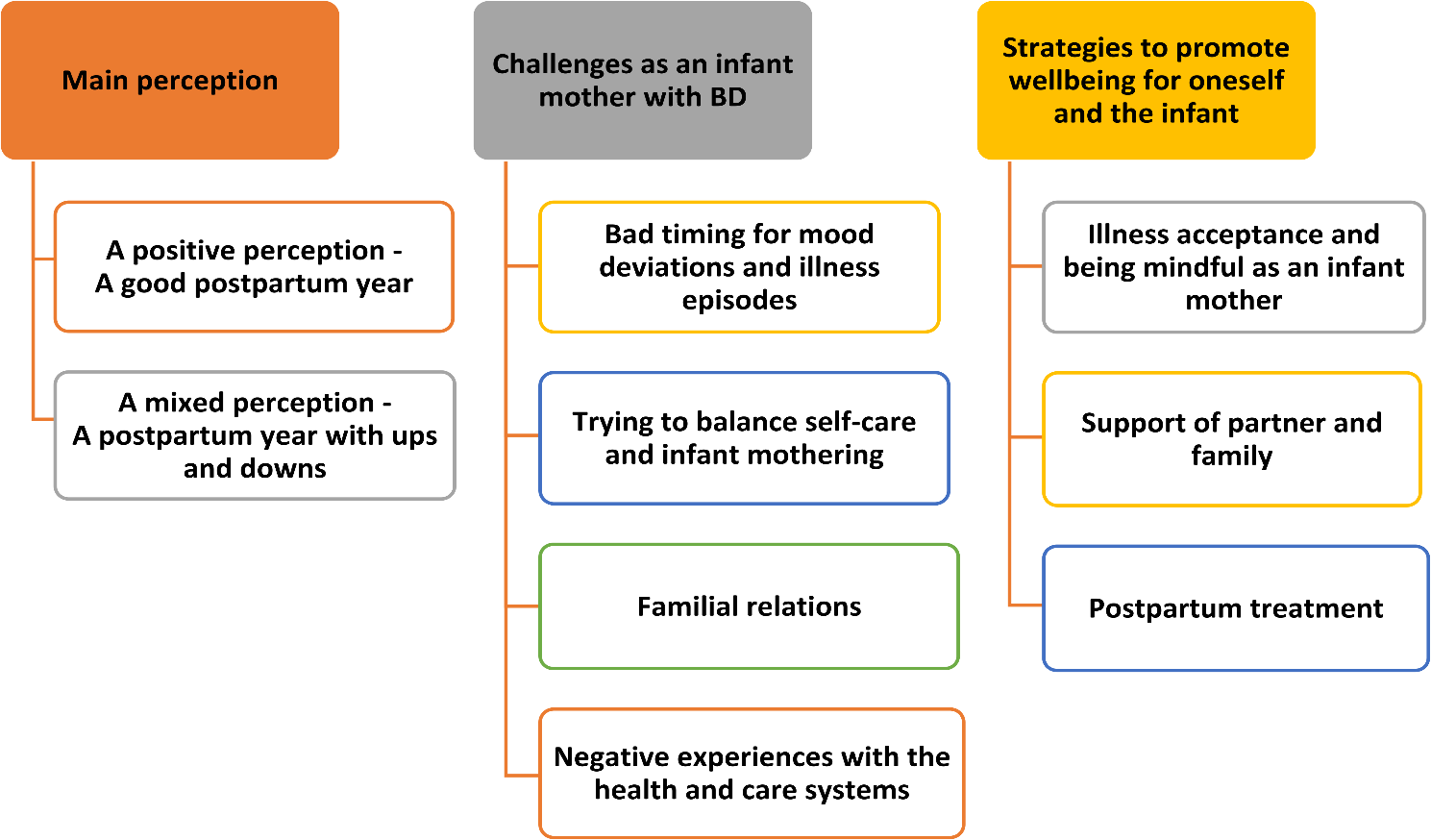


Table 1 shows the demographic and clinical characteristics of the sample. All women lived with the infants’ biological father.
Table 1 Demographic and clinical characteristics of the sampleSixty-five percent of the women (n = 17/26) initiated breastfeeding at birth and 46% (n = 12/26) continued to breastfeed until at least six months. Breastfeeding was mostly chosen by the women who were medication free (n = 7/8) or on Lamotrigine monotherapy (n = 6/6) at birth. In addition, two women breastfed with antipsychotic medication (one on monotherapy, and one on polytherapy with antidepressants), and two women breastfed with Lamotrigine polytherapy with antidepressants. 35% of the women (n = 9/26) did not initiate breastfeeding, mainly due to Lithium medication (n = 6/6). Most of these women (n = 4/6) expressed sadness over the decision, as it conflicted with their desire to breastfeed. Moreover, an intention to secure sleep was a reason for three women not to breastfeed (n = 3). These women seemed to be content with their decision. The prioritising of sleep was also a common reason for women to combine breastfeeding and formula, or to cease breastfeeding after some few months.
Mood symptoms in the first yearIn Table 2, the sample is divided into four subgroups based on symptom severity at 3 and 12 months. The table also displays each participant’s BD type, type and duration of use of main medication, type and duration of use of specialist mental health services, and the women’s main perception of the first year.
Table 2 Participants’ BD type, symptom severity at 3 and 12 months, main BD medication, use of specialist mental health services and main perception of the first yearSubgroup 1: 42% of the sample (n = 11/26) were either euthymic or had only mild mood symptoms at 3 and 12 months. In the interviews, 91% of the women in the subgroup (n = 10/11) evaluated these measures as representative of their general mood state during the first year. One woman (no. 7) revealed having had mild to moderate depressive symptoms for approximately one month at eight months.
Altogether, apart from one woman, subgroup 1 was identified as having had a relatively stable first year in terms of mood symptoms.
Subgroup 2: 23% of the sample (n = 6/26) had moderate mood symptoms of depressive polarity at 3 and/or 12 months. None of the women confirmed having had hypomanic/manic symptoms. The two women (nos. 12 and 13) who were euthymic at three months dated the initiation of their depressive symptoms to eight (no. 12) and ten (no. 13) months. For woman no. 14, the moderate depressive symptoms at three months gradually alleviated to milder symptoms, which persisted at 12 months.
The three women (no. 15, 16 and 17) who had moderate symptoms at both time points described recurring struggles with depressive symptoms over the first year.
Overall, subgroup 2 was identified as a group with moderate depressive symptoms of various lengths during the first year.
Subgroup 3: Another 23% of the sample (n = 6/26) had severe mood symptoms of depressive polarity at 3 and/or 12 months. Two women (no. 18 and 19) had hypomanic symptoms at three months, and in all, 83% of the subgroup (n = 5/6; all women except no. 21) confirmed mood shifts of both polarities during the first year in their interviews.
Overall, subgroup 3 was identified as a group with severe depressive symptoms of various lengths during the first year.
Subgroup 4: The last subgroup included three women (12%) who had postpartum psychosis of mixedFootnote 3 (no. 24), depressive (no. 25) and manic (no. 26) characteristics and was identified as a group with a heavy illness load throughout the first year.
See Supplementary file 1 for more information on the participants’ postpartum medication, and Supplementary file 2 for more information on the distribution of the participants’ scores at 3 and 12 months on extracted IDS items and on YMRS.
Thematic resultsOur research questions yielded an overarching thematic structure for the infant mothers’ experiences of the first year, with nine associated main themes (Fig. 1):
Fig. 1
Each main theme contains between none and four subthemes, as reported below. We present representative quotes to illustrate the key qualities of each theme and to demonstrate how the themes were grounded in the data.
Main perceptionA positive perception—A good postpartum year38% (n = 10/26) of the women reported a main perception of the first year as a positive and good experience and were defined as a positive group (Pos. Gr). Six of the ten women described the experience as better than expected. The women used phrases such as “It has been a very nice experience.” (no. 1) and “It has come out much better than I feared.” (no. 9).
The main storyline in a large majority of the women’s narratives centred on an experience of positive development and mastery. Primiparous women accentuated a sense of growth and enrichment in accomplishing the role as a new mother: “It has been a lot of new learning and new values, as a mother. I am very positively surprised that it has gone so well to have a baby.” (no. 13) Most multiparous women (n = 3/4) described a sense of reparation in relation to previous tough postpartum experiences: “In all, it has been a ‘boom’, because after my first birth I had a postpartum psychosis. This time it didn’t happen, so now I feel that it has been normal. The way it should be.” (no. 2).
As a group, the women gave voice to a pleasure in having become a mother, enjoying their infant and having a daily life that they viewed as normal and stable: “It gives pleasure to have a child. My priority has been a quiet daily life.” (no. 1), and “It has all fallen into place.” (no. 10).
90% (9/10) of the women with a positive perception were either euthymic or had only mild mood symptoms during the first year (see Table 2). One woman (no. 13) deviated from this pattern and developed moderate depressive symptoms at ten months, as described in the previous section.
A mixed perception—A postpartum year with ups and downs62% (n = 16/26) of the sample reported a mixed perception of the first year, defined as apparent positive and negative accounts by each woman. This group was defined as a mixed group (Mix. Gr), although one woman tilted towards a mainly negative perception (no. 17) (see Table 2). The women’s descriptions included phrases such as “Actually, it has varied, with a lot of ups and downs. It has been everything: times with deep depression, times when I and my husband have struggled, and times when it has been really nice.” (no. 20).
When talking about their negative experiences, mood deviations and the consequences of having been ill were at the forefront for most women: “It has been heavy. Being on maternity leave was tough. I had a period with heavy depression and then the depression went somewhat up and down.” (no. 17).
Echoing the Pos. Gr, most women in the Mix. Gr described the value of having become a mother, a (bigger) family and a joy over the infant as dominant positive experiences: “It’s a joy that we have him (i.e., the infant). He is a nice little boy, and we enjoy being with him together as a family.” (no. 26) However, contrasting the Pos. Gr, only a minority of the women in the Mix. Gr (25%, n = 4/16) reported a sense of growth and mastery as a mother. These women revealed that the stresses of new motherhood together with episodes of illness made for a difficult process. “I would have done it again. Yeah, actually. Many think it’s strange, since I have been so ill. But it has been very good and developing for me.” (no. 25).
88% (14/16) of the women with a mixed perception of the first year had moderate or severe mood symptoms at 3 and/or 12 months, including postpartum psychosis (see Table 2).
Challenges as an infant mother with BDBad timing for mood deviations and illness episodesWomen in both the positive and mixed groups gave accounts of how mood deviations can be significant postpartum challenges. However, the portion of women conveying this was higher in the Mix. Gr (94%, n = 15/16) than in the Pos. Gr (30%, n = 3/10), and their accounts were more salient and richer in detail, based on their prominent experiences of mood deviations after childbirth.
The women’s narratives revealed how mood deviations are experienced differently and as being particularly unwelcome when being an infant mother. For instance, when women are euthymic during pregnancy, a postpartum relapse can be perceived as especially harsh: “The pregnancy was so nice. I have never been so well from my illness as when I was pregnant. And then, it’s so dramatic and heavy to be ill afterwards. Quite simply shit!” (no. 22, Mix. Gr).
In more than one-third of the sample (Pos. Gr: 10%, n = 1/10 vs. Mix. Gr: 50%, n = 8/16), the narratives implied that mood deviations had a negative impact on the women’s sense of being a mother and their mothering confidence: “I felt that being a mother was two, or even four, sizes too big for me. (…) I just couldn’t understand what that ‘little thing’ wanted, what she needed and what she expected from me. (…) And I can still feel as if I am acting.” (no. 15, Mix. Gr).
At its extreme, postpartum episodes could be felt as “too much”, causing feelings of regret in a few women: “I have felt it as a really bad idea to have children. Some days, I just want to leave. I want to be alone. I cannot take being with them. Nothing I do works.” (no. 17, Mix. Gr). Even suicidal ideation was triggered in a small minority of three women (12%) during severe depression and near-psychotic states. “I have had thoughts of suicide when in deep depression. But it’s no longer a choice, because of her (i.e., the infant).” (no. 20, Mix. Gr).
Fearing postpartum mood deviationsThe narratives revealed a recurring fear of becoming ill related to “bad timing”. Notably, such accounts were more common in the Pos. Gr (60%, n = 6/10) than in the Mix. Gr (19%, n = 3/16). The fear could either be provoked by symptoms, “I had hallucinations a couple of times, and got really afraid that I might develop a depressive psychosis.” (no. 16, Mix. Gr), or by situations commonly viewed as symptom triggers, “When I get tired, I have this fear of becoming depressed. Then, all the time, there is this fear of ‘What’s happening?’, ‘Is this the start of becoming ill?’. These worries are an extra burden. (…) I am so afraid of becoming ill!” (no.9, Pos. Gr). A taxing loop of fear, vigilance and stress was disclosed by some of the women.
Depressive mood deviationsOf the mood polarities, depressive deviations were the most common, with 54% (n = 14/26) of the women having IDS scores at 3 and/or 12 months in the moderate to severe range (Table 2). 62% of the women (Pos. Gr: 40%, n = 4/10 vs. Mix. Gr: 75%, n = 12/16) described how depressive mood deviations may impact their mothering. A recurring feature was a sense of something missing, an absence of something that should have “been there” in their mothering. This included a sense of not being mentally present and available for the infant: “Sometimes I must pull myself together to be present with him. Because I am gone. In my mind.” (no. 13, Pos. Gr). Furthermore, women described a lack of energy in their mothering: “It was all quite heavy. I didn’t have the energy for almost anything. It was not possible for me to be alone with him all day, to bear all the responsibility.” (no. 17, Mix. Gr), as well as a lack of patience, “This time, when I was deep down, I couldn’t handle it. For example, when she was whiny and couldn’t fall asleep. I didn’t handle it the way I usually do, with patience, like nowadays.” (no. 7, Pos. Gr). Some women experienced challenges as even more severe as the infants grew older. Coping with depression while caring for an infant who was more awake during the day, interactive and mobile could be considered incompatible endeavours: “I don’t think I would have managed to have him at home the whole day now. I would have become even more depressed. It went well when he was little. But I feel that if he demands too much of me, if I must, you know, pay attention all the time, then it gets too much for me.” (no. 23, Mix. Gr).
Hypomanic mood deviationsWomen with hypomanic symptoms (Mix. Gr: 31%, n = 5/16) talked about irritability, agitation, racing thoughts and “being carried away” in different activities as particular mothering challenges. One woman described the ironic nature of her absorption in baby accessories on the internet while missing out on her infant’s bids: “When I was hypomanic-manic, I began with all these baby-accessories on the internet. (…) I got all caught up. I bought a lot of things and spent a lot of time on the net. You are in these chat-groups, and it’s really easy to get hooked. But then I found out that ‘Hey, this is wrong!’. I kind of buy all these nice baby-things and chat with others about baby-stuff, while my baby is crying beside me. And I don’t notice! That’s not the point! I should be with my baby!” (no. 19, Mix. Gr).
Postpartum psychosisBeing ill with postpartum psychosis was described as an overwhelming experience (Mix. Gr: 19%, n = 3/16), which profoundly contrasted with women’s prenatal expectations of new motherhood. A deep concern for the impact on the mother-infant relationship was evident, intensified by the separation when being hospitalised: “The worst, it’s almost like I cannot forgive, is that I felt it as if they robbed my son away from me. (…) To see them (i.e., father and son) leaving me, ruined me. Time after time. I held, I just held my son close to me the whole time when they were present. Just held.” (no. 25, Mix. Gr).
In addition to the acute phase of psychosis being highly stressful, the recovery phase represented more drawn-out maternal challenges in terms of repairing the bonding with the infant, processing the grief of what had been lost, and dealing with worries: “It took me at least six months before I felt that ‘This is ok.’ (…) I was so worn out of everyone telling me about ‘Attachment, and mother, mother, mother.’ ‘That he will be damaged, get ADHD, be totally crazy.’ I thought, ‘Oh, my God, with his BD genes! How will everything end?’ (…) My husband has ensured me that ‘You have had your maternal instinct all the time.’ And I do feel that I have had it. To protect him, feed him, give him dry diapers. But the maternal love, to feel that he is mine and that I love him. It wasn’t there, I couldn’t feel it.” (no. 25, Mix. Gr).
Trying to balance self-care and infant motheringA large group of women (Pos. Gr: 50%, n = 5/10 vs. Mix. Gr: 81%, n = 13/16) spoke about the challenges in trying to maintain self-care and preventive measures while practising mothering and attending to the infant’s needs: “It’s more difficult now, because you have someone else to think about. He takes a lot of my energy, or it’s more like you want to give him what you have. (…) Anyway, it’s difficult to ‘refuel’, because you give what you have during daytime, or even at nighttime. When he needs it.” (no. 12, Mix. Gr).
The main challenge was to secure sleep—night awakenings and possible sleep deprivation are inherent in caring for an infant: “I had to get up every second to third hour (i.e., to feed the infant). I had too little sleep, and you know, that can result in me becoming hypomanic.” (no. 18, Mix. Gr) Trying to avoid exhaustion and stress was also difficult, “I am afraid of getting exhausted, because I know that then I am more vulnerable. But, you know, the first year with a baby, you get exhausted.” (no. 6, Pos. Gr).
Some women on medication found that side effects could negatively affect their ability to mother: “I think it’s difficult to be on medication. So many of the medicines make me lethargic or make me sleep too tight. And it can’t be that way when I have a baby. So, actually, now I don’t use them (i.e., her prescribed medication).” (no. 16, Mix. Gr).
Familial relationsChallenges in their familial relationships (i.e., infant, partner and grandparents) were most prominent in the reports of women in the Mix. Gr (75%, n = 12/16), who often disclosed challenges in at least two types of familial relationships. Familial challenges were less common in the Pos. Gr (40%, n = 4/10) and were mainly associated with one type of relationship. The common subject in both groups was concern about the familial impact of postpartum mood deviations: “When I become depressed it’s like it ‘contaminates’ the others around me. The total lack of energy and the mood swings affect everybody.” (no. 20, Mix. Gr).
Moreover, there were various challenges and concerns related to different family members.
The infantEven though the women explicitly talked about mood deviations affecting their mothering, only a minority of the women (Pos. Gr: 20%, n = 2/10 vs. Mix. Gr: 25%, n = 4/16) acknowledged that their infant had been subjected to overt mood symptoms, such as the mother’s apparent anger or sadness. This was troubling for the women to think about, “He has been present in situations where I haven’t been stable. There has been shouting and yelling, or, like hard negative talk. So, he has noticed, and I think it’s like ‘What happens now?’ for him, because he isn’t used to it. (…) It’s not alright. No, it isn’t. So, you try to avoid such situations.” (no. 23, Mix. Gr).
The partnerHalf of the women in both groups (Pos. Gr: 50%, n = 5/10 and Mix. Gr: 50%, n = 8/16) highlighted the partner as the main person affected by their BD postpartum. This comprised the women’s need for support in euthymic phases (i.e., to maintain self-care measures) and aid in illness phases (i.e., partner taking over care responsibilities for the infant). Typically, women in both groups saw this as a challenge—he had to be prepared to make more effort than what was “his share” as a new parent: “He takes a lot of responsibility, even at nights. Also, other things to relieve me, so he does a lot. Does the cooking, fixes and arranges. He really does everything.” (no. 13, Pos. Gr).
The narratives also revealed strained and conflicted couple relationships in the first year, mainly in the Mix. Gr (Pos. Gr: 10%, n = 1/10 vs. Mix. Gr: 50%, n = 8/16). A common reason was the stress inflicted by episodes of illness and the woman’s altered behaviour: “We have had rough times, but most of the time it has been good. (…) A couple of times it has been because of money. It comes easy for me to spend a lot of money, and not to think over it. (i.e., when ill in hypomania)” (no. 19, Mix. Gr).
The grandparentsThe main challenge in relationships with grandparents was that they were not available or supportive when needed (Pos. Gr: 20%, n = 2/10 vs. Mix. Gr: 44%, n = 7/16). Some women reported sadness when grandparents lived far away but expressed it as a straightforward and manageable feeling. A more complex and disappointed feeling was displayed when the lack of support was either contrary to promises given during pregnancy or because of intergenerational conflicts: “It’s like my parents drain me of energy. (…) It has to do with our family history. (…) It’s not good for me to have to depend on my mother.” (no. 15, Mix. Gr). Notably, for some women, the transition to motherhood could reactivate troubled childhood memories of having lived with a parent with BD or other mental disorders and complicate the current parent–grandparent relationship: “My father is rather ill from time to time (i.e., BD). (…) It was an unstable family situation, without safety. We never knew what the next day would be like. (…) After I had my own children, memories have returned and become stronger. So, my relationship with my mother and father has become more complicated.” (no. 16, Mix. Gr).
Negative experiences with the health and care systemsUnfortunately, instead of feeling supported and helped, about a quarter of the women (Pos. Gr: 30%, n = 3/10 vs. Mix. Gr: 25%, n = 4/16) disclosed unwanted negative experiences with the health and care systems. Women did not report dissatisfaction with professionals’ medical or psychiatric knowledge. Rather, they described experiences of feeling denigrated and met with prejudiced assumptions as infant mothers with BD. For instance, when care information was presented normatively without individual adaptation, it could cause a feeling of having failed and not belonging “as a mother amongst mothers”, “I had to quit attending these ‘mother-baby-groups’ and the community well-baby clinic. And I avoided the internet. Well, just everyone who said that ‘the mother is the most important’ (…) and declared proper daycare, etcetera. I have had help and babysitters since he was three weeks old! Not because I wanted, but because it was urgent and vital! And the focus on breastfeeding and the immune system. We have given him infant formula from day one! Everything that I felt I had done wrong was only confirmed.” (no. 25, Mix. Gr).
Furthermore, encounters with the care systems could be considered suspicious surveillance, resulting in remorse for having reached out for help: “They came from the child protection services and observed me. I needed help. They said that the children had to be shielded. I was stunned by their language because people in child protection have power. So, I wondered what their solutions were. They meant that I had to contact people in my network, that family and friends had to come and help me. I said that ‘I don’t have anyone to step up 24 hours a day!’ (…) So, they observed and observed and concluded that they had to come back and observe. (…) It was a very tough situation, I really must say.” (no. 21, Mix. Gr).
Notably, based on their experiences, some of the women revealed regret about having disclosed their BD to health professionals: “I didn’t think so much about it in the beginning. But now, when I feel like I am myself again, it’s a label that isn’t so easy to relate to. (…) In the beginning it was important for me to be open. And I regret that now. (…) For instance, at the well-baby clinic, I feel that I must accept assumptions about my situation, when I actually want to protest: ‘But honestly, it isn’t like that.’ Things that are tough to hear when you are a new mother and want to be safe and good for your baby. (…) In a way, it’s kind of humiliating. So, I think that having disclosed is what I regret the most.” (no. 6, Pos. Gr).
Strategies to promote wellbeing for oneself and the infantIllness acceptance and being mindful as an infant motherA personal acceptance of “how things are” when having a recurring mental illness and being an infant mother seemed to be a primary process for health-promoting priorities to become integral in postpartum daily life and to include both the mother and the infant. All women in the Pos. Gr (n = 10/10) provided explicit reports on trying to be mindful of their illness and their daily priorities for their own and their infant’s wellbeing and needs. The same was evident for 75% (n = 12/16) of the Mix. Gr, “I have become more conscious about different things. I think I have accepted and reconciled with my illness in another way now. (…) All has become calmer and more natural. I take more precautions. For instance, no computer or screen devices before bedtime. And I am better at planning ahead, to avoid stress. Before the baptism, I made a list. I think and organise ahead, so I don’t have to do everything at the same time. And I am better at ‘leaving things at that’. Before, I didn’t want to relate to the illness, I denied and trivialised. And it went bad.” (no. 2, Pos. Gr).
Despite the inherent challenges in practising self-care as an infant mother, several women spoke about a maternal responsibility to try to stay well. Keeping their infant in mind added motivation to health-promoting priorities: “You must be aware of your own limitations and think ‘Now it’s not only about me.’ I must take extra good care of me, to take care of my baby. I must have consideration for her wellbeing. Therefore, I make sure that I sleep and eat well, you know, live healthy.” (no. 1, Pos. Gr) What health-promoting priorities each woman was mindful of could differ based on individual needs. For instance, “I am very sensitive for stress. I need to prioritise. What appointments can I cancel? What can be downgraded and be more basic?” (no. 6, Pos. Gr).
Being mindful of the infant’s wellbeing included an awareness of one’s own impact on the infant: “I think I am very conscious of how I behave with him (i.e., the infant). That’s why I tell my husband or my mother-in- law when I have a bad day. They assist so that I am not alone with him.” (no. 16, Mix. Gr) This also implied prioritising energy to mothering, “It is much easier now, when he is at day care. I can rest and be alone during the day, and then I have the energy to give care in the afternoon and evening.” (no. 17, Mix. Gr).
Support of partner and familyIn the previous section on challenges, we described women’s concerns about the impact of postpartum illness on family members. These concerns were largely associated with the fact that a majority of the sample (Pos. Gr: 70%, n = 7/10 vs. Mix. Gr: 75%, n = 12/16), viewed familial aid as almost essential for wellbeing and to manage mothering in the first year.
The most reported support from the partner was of a practical nature, “I was very deep down, so he (i.e., partner) had to take over the maternity leave and take care of our daughter a lot. They were outdoors most of the days. It helped and was really important, we couldn’t have managed otherwise.” (no. 20, Mix. Gr). The partner’s assistance, allowing the mother to sleep, was precious: “You know what they say, ‘Infant parents don’t sleep at night.’. Well, I do, but my husband doesn’t. He takes the night shifts.” (no. 10, Pos. Gr).
Furthermore, the partner’s emotional support was highly valued: “In that period (i.e., when depressed), my husband emphasised, ‘Take one day at a time.’, ‘Don’t think about what will happen tomorrow.’, ‘Set up small goals for today, and then you handle tomorrow when tomorrow comes.’” (no. 9, Pos. Gr).
The way in which partner support was initiated varied within the sample. Some couples appeared to have talked about the forthcoming challenges and preventive measures during the pregnancy. In other couples, the woman had to be explicit on urgent needs for aid: “Well, I had to tell him sometimes that ‘You must take him this night. You really must, even if you are going to work in the morning.’. I don’t think he was so observant of how bad it was for me.” (no. 12, Mix. Gr). Alternatively, a health professional had to address the matter: “We were at the psychologist’s office, and she told him, ‘This doesn’t work, you must take more part in this. Even if you work, you must assist.’” (no. 15, Mix. Gr).
Although the partner’s support was primary among the women, in cases where grandparents were available for aid, it was vital, “Our family has been here. Since I haven’t been present neither physically nor mentally, it has been a huge comfort to know that my baby has been taken well care of. And my husband has received assistance from our parents.” (no. 25, Mix. Gr) Notably, when having received helpful support, there could be hints of reparation in familial relations that previously had been conflicted: “When I was little, I only wanted to be with my father. (…) I felt much safer with him. Now my mother has been baby-sitting several times and it has gone well. I have given her clear directions about things. There are so many things that I feel she did wrong in my childhood. (…) I have talked with her a lot about it, and I think she does it well now.” (no. 7, Pos. Gr).
Postpartum treatmentAlthough some women voiced challenges in dealing with the health and care systems, almost everyone (92%, n = 24/26) felt that they needed some kind of postpartum treatment, preferably at the specialist mental health care level. 31% of the sample (Pos. Gr: 40%, n = 4/10 vs. Mix. Gr: 25%, n = 4/16) felt satisfied and safe with pharmacotherapy only, “I have been very confident that my medication is effective, so I haven’t been afraid (i.e., of illness relapse).” (No. 2, Pos. Gr).
Instead of medication, 19% of the sample (Pos. Gr: 10%, n = 1/10 vs. Mix. Gr: 25%, n = 4/16) preferred psychotherapy, either individually or with an infant mental health team, “It has been very useful with help from the infant-mental health team. To talk about our experiences, without being viewed as terrible parents.” (no. 15, Mix. Gr).
Finally, several women favoured a combination of medication and psychotherapy (Pos. Gr: 40%, n = 4/10 vs. Mix. Gr: 44%, n = 7/16), “I felt that with both measures - more frequent therapy, starting medication - we retrieved it in a way, and I avoided to touch the bottom. The access to someone to talk to is very important for me. It helps me to reach an inner calm. (…) I need both.” (no. 9, Pos. Gr).
Comments (0)