
Remember me
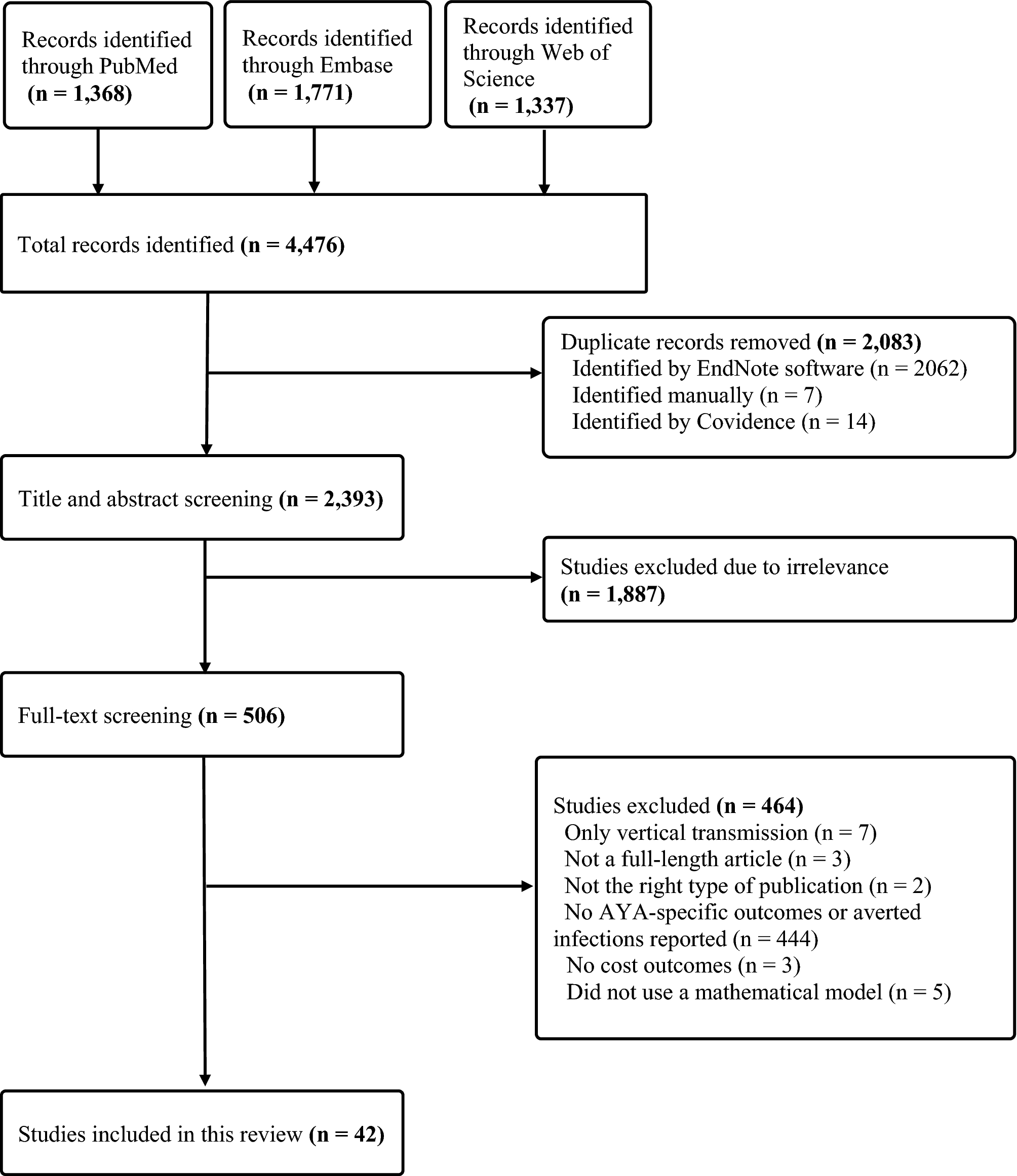




The database search yielded 14 relevant economic evaluations, as shown in the PRISMA diagram (Fig. 1). The key characteristics of the included studies are summarised in Tables 1 and 2. All the included economic evaluations but one [19] conducted a cost-utility analysis (CUA), and Markov-based modelling was applied in nine studies. The perspective was stated as provider in most studies, with just two evaluations adopting a societal perspective [20, 21]. Studies usually had a short time horizon and seven covered lifetime [14, 20,21,22,23,24, 37].
Fig. 1 Table 1 Summary of included studiesTable 2 Technical specifics and main findings of the included studies3.1 Health Outcomes
Table 1 Summary of included studiesTable 2 Technical specifics and main findings of the included studies3.1 Health OutcomesThe key outcomes considered included survival probability, duration of initial hospitalisation following the implant and the probability of hospitalisation per year after the initial discharge, and QALYs in CUA studies (n = 13). In the absence of clinical studies performing a direct comparison between medical management and contemporary LVADs, all evaluations relied on comparing single arms from different studies of LVAD and medical management. Although the studies mostly used clinical data from the HeartMate II Destination Therapy (n = 3) and Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) (n = 7) trials or the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) registry (n = 4), utilisation of the data differed substantially. For example, studies utilised different assumptions and methods when extrapolating mortality risks. The mortality risks assumed for LVAD recipients beyond 24 months was estimated by averaging the changes in the last 6 months by Lim et al. [25] while the risk for the 24th month was used for the remaining cycles by Beese et al. [14], although both used the mortality risks reported in the MOMENTUM 3 trial [26]. The impact of major events on mortality was incorporated only in one model for stroke, gastrointestinal bleeding and driveline infection [23].
Utility values varied substantially, depending on the source used. For example, Shreibati et al. [20] used 0.40 for MM based on Grady et al.[27] while Chew et al. [22] used 0.53 based on Göhler et al. [28]. Only five studies applied utility values specific to DT patients [14, 20, 24, 25, 29]. One study converted US utilities to UK values using an algorithm [24]. Utilities reported for BTT patients by Moskowitz et al. [30] were used in four studies while one study applied values for bridged patients in the first month as estimated by Sharples et al. and used 1-year utility values estimated for DT patients in the following months [23, 31]. Other utility sources did not distinguish between DT and BTT patients. Given that DT patients usually have lower quality of life than BTT patients, studies relying on utility values from BTT patients might be overestimating the health benefits of LVADs. However, utility values also varied substantially across the studies which used DT-specific values, ranging from 0.40 to 0.64 for MM [14, 20, 24, 25, 29].
3.2 Resource Use and CostsDirect medical costs considered in the studies included the device and initial hospitalisation, re-admissions, and outpatient visits. Most studies also considered the cost of an LVAD replacement in the case of a device failure [20, 22,23,24, 29, 32]. Additionally, Neyt et al. [21] adopted a wider perspective, taking into account travel and ‘social work’ costs, although it was not clear what ‘social work’ entailed.
The largest cost component was the initial cost of LVAD implantation and in 2023 prices, it varied from £104,764 in the UK [24] to £194,098 in the US [33] (Fig. 2). There was no clear trend in the index costs over time. For example, older studies by Adang et al. [34] and Clegg et al. [35] presented costs similar to more recent ones, such as Lim et al. [25]. The variations in the estimates were caused by the differences in the setting, device and methodology of the studies (e.g. included costs, time horizon).
Fig. 2
Index cost of left ventricular assist device (LVAD) implantation in 2023 prices. *Included device cost only
Many studies used cost data for BTT patients since LVAD was not part of the standard care for DT patients in the Netherlands and the UK [14, 21, 24, 35, 36]. All studies used the same discount rate for costs and benefits except for Neyt et al. [21] and Clegg et al. [35], who applied different discount rates for costs (4% and 6%, respectively) and outcomes (1.5%).
3.3 Cost Effectiveness of Left Ventricular Assist Devices (LVADs) as Destination TherapyMost of the reviewed studies (n = 9) found that LVADs were unlikely to be cost effective compared with MM as DT while two UK-based studies reported the opposite [24, 25]. In addition, one US-based study estimated an ICER per QALY that was just above the usually accepted $100,000 threshold in the USA [29]. The findings were not clear in the remaining two studies [19, 37]. The study by Canadian Conseil d'évaluation des technologies de la santé (CETS) estimated an ICER per life year and did not state whether this would be considered cost effective [19]. The estimated figure (CAD$67,883) was much higher than the usually accepted threshold of CAD$50,000 per QALY [38]. The study by Messori et al. [37] was not a traditional cost utility study. It estimated the average reimbursement for patients at €82,426, which aligned closely with HeartMate's price of €75,000, which was found financially viable by the authors.
Most studies (n = 13) reported incremental cost per QALY gained as the main outcome and incremental cost per life-year gained was used as the key measure in one study [19]. Cost effectiveness was estimated over a time horizon of 5 years or longer in 10 studies (Fig. 3), and the estimated incremental cost per QALY ranged between £52,425 and £273,975 in 2023 prices [24, 35]. More recent studies (published between 2019 and 2024) reported a substantial improvement in the cost-effectiveness estimates [14, 24, 25, 29]. The studies conducted in the UK estimated a range of ICER per QALY values, but mostly remained more moderate compared with the studies in the USA.
Fig. 3
Incremental cost per QALY estimates in economic evaluations with a time horizon of 5 years or longer. ICER incremental cost-effectiveness ratio, QALY quality-adjusted life-year
The impact of disease severity on cost-effectiveness findings was estimated in two evaluations based on INTERMACS profiles. In the study by Lim et al., this was based on varying survival data in for the MM arm while survival data for the LVAD arm was constant [25]. ICER per QALY was lower for the patients with an INTERMACS profile 1–3 (£52,423) and higher for those with an INTERMACS profile 4–7 (£74,720) compared with the base-case estimate (£54,428) in 2023 prices. The second study estimated different mortality probabilities and quality of life estimates for INTERMACS profiles 1, 2–3, and 4–5, for both the LVAD and MM arms, although the estimates for the MM arm included expert views and important assumptions [14]. Findings of this analysis was similar to the study by Lim et al. [25], suggesting that the use of LVADs might be more cost effective in patients with less severe heart failure (£72,121 for INTERMACS 2–3 and £64,775 for INTERMACS 4–5) than those with a more severe condition (£93,393 for INTERMACS 1).
Although the estimates are not directly comparable due to methodological differences, all studies with a time horizon of 5 years or longer concluded that the incremental cost of LVAD as DT per QALY was higher than the standard thresholds accepted in relevant settings, except two studies which estimated an ICER per QALY of just below NICE’s former threshold of £50,000 for end-of-life treatments in the UK in 2019 prices [24, 25].
3.4 Uncertainties Around the FindingsAll the included studies conducted sensitivity analyses to explore the uncertainties around their findings. It was not possible to identify a specific parameter as the main source of uncertainty across studies because the cost-effectiveness estimates were sensitive to different parameters in each study. For instance, estimates were most sensitive to re-admission rates and costs in one study [20] and to LVAD implant cost and survival expectancy in another [22]. The probability of cost effectiveness at different willingness-to-pay thresholds was explored in six studies. It was estimated as 0%, 33% and 44% in three different US-based analyses, at a $100,000 threshold per QALY [20, 22, 29]. It was 50% at a €100,000 threshold per QALY in the Netherlands [21]. In the UK-based evaluations, this figure was 0% at a threshold of £30,000 [14], 63% and 97% at £50,000 [24, 25] and 90% at £60,000 per QALY [14]. The specific parameters that had a great impact on the probability of cost-effectiveness estimates were not reported in the studies. Therefore, it is not clear what caused this variation across studies. Different model structures and inputs, selection of distributions as well as assumptions could contribute to that.
3.5 Quality of the Economic EvaluationsSome important issues were identified in terms of the quality of the studies, using the CHEC and Philips criteria. Findings of the quality assessment are provided in Tables 1 and 2 in the ESM. The study perspective was defined as societal in one study although only direct medical costs were included [20]. Most studies used a time horizon of 5 years or longer, which is considered acceptable given the life expectancy in patients with AHF, while two studies used a shorter time horizon [34, 36]. Regarding the model structure, two studies applied 3-monthly cycles with no justification although all the other models used monthly cycles [22, 25]. Some studies did not explicitly provide all the parameters used in the models. For instance, the estimated mortality risks beyond 2 years were not reported in two studies [21, 22], despite using extrapolated data. Additionally, most studies did not justify the sources of parameters selected; just one used a systematic review to identify the mortality risk and health utilities within the first 2 years [21].
The long-term impacts of the complications on DT patients were not widely considered as only three studies modelled some complications as separate health states, and the studies assumed that after a month, the impact of the complications would be reversed [14, 21, 23]. Only two studies considered the impact of INTERMACS profiles or age on mortality, morbidity or quality of life [14, 25].
The studies generally used data from small numbers of patients from a single centre to identify the cost inputs. Moreover, some studies did not consider all important cost components; for example, all of the trial-based evaluations omitted the cost of complications. Although hospitalisation costs were included in all studies, the details of how complications were incorporated were not fully explained.
3.6 Changes in Study Design and Evidence Base Over TimeThere have been substantial developments regarding LVADs and the available evidence since the publication of the first economic evaluation included in this review in 2007. In parallel with the increasing evidence base, more recent studies were more likely to incorporate distinct adverse events in the evaluations. Recent studies were also more likely to have used utility values specific to DT patients. However, there were some cases contrary to the general trend of improvement in the structure and quality of the economic evaluations over time. For example, some recent studies did not incorporate a utility decrement due to adverse events while it was included in some older ones.
Overall, studies published recently were more likely to have used a higher survival rate for the patients living with an LVAD. For example, 1-year survival rate ranged between 0.50 and 0.68 in studies published between 2007 and 2013 while it was between 0.58 and 0.85 in the studies published between 2014 and 2021. Despite the evidence showing that survival was longer and adverse events were lower with newer technologies, one of the more contemporary devices (HeartWare HVAD) was withdrawn due to safety concerns. Some recent economic evaluations used clinical data that were entirely based on this device, and others used data that might have included people using this device [24, 29]. This should be considered when interpreting the outcomes of these studies. Although there is no study that compared HVAD with the other new-generation device available (Heartmate III), the economic evaluation of Heartmate III reported similar results to the economic evaluation of HVAD in the UK.
The persistent gaps in data for critical areas have ongoing implications for economic evaluations. Although the evidence base seems to be expanding on the LVAD arm, substantial gaps remain on the MM arm. Firstly, in the absence of a clinical trial of direct comparison between Heartmate and MM, evaluations had to rely on an indirect comparison estimated in a network meta-analysis, which involved significant assumptions and uncertainty. Secondly, there is limited and inconsistent data on QALYs estimated for DT patients, with studies utilising values between 0.40 and 0.64. Additionally, due to a lack of data on the quality-of-life impacts of adverse events after LVAD implantation as DT, most evaluations did not consider this or relied on expert opinion. There is not sufficient data regarding the impacts of LVADs for patients with different severity of disease (e.g. INTERMACS profiles) to be able to accurately incorporate this into economic evaluations and estimate cost effectiveness for different groups, although one recent study attempted this [
Comments (0)