
Remember me

Clinical, pathologic, and molecular features of low-grade NET and high-grade metastases from five patients are summarized in Table 1 and Supplemental Table 1. Tumors from all patients demonstrated diffuse keratin and synaptophysin expression, as well as focal, patchy, or diffuse expression of another neuroendocrine marker (chromogranin and/or INSM1). The primary NET site was the pancreas in three patients (patients 1–3), the pituitary in one patient (patient 4), and unknown in one patient (patient 5). The median patient age at initial NET diagnosis was 53 (range 38–59 years old). Four patients were male and one was female. Patients 1 and 5 had both low-grade NET and G3 NEN present at the time of initial diagnosis, without receiving any NET-related therapy prior to high-grade progression. Patients 2–4, on the other hand, received multiple NET-related treatments prior to high-grade progression, which occurred many years after the initial low-grade NET diagnosis. All five patients developed metastatic disease and died of disease. Three patients (patients 1, 2, and 5) had liver metastases at the time of the first NET diagnosis; patient 3 developed liver metastasis 8 months after the first diagnosis; patient 4, with a pituitary primary, developed intracranial metastasis 54 months after the first NET diagnosis. Median overall survival from the time of the first metastatic disease to the time of death was 41 months (range 12–171). The median overall survival from the time of G3 NEN diagnosis with Rb loss and aberrant p53 to the time of death was 12 months (range 4–41). Detailed descriptions of tumor progression are described for each patient below.
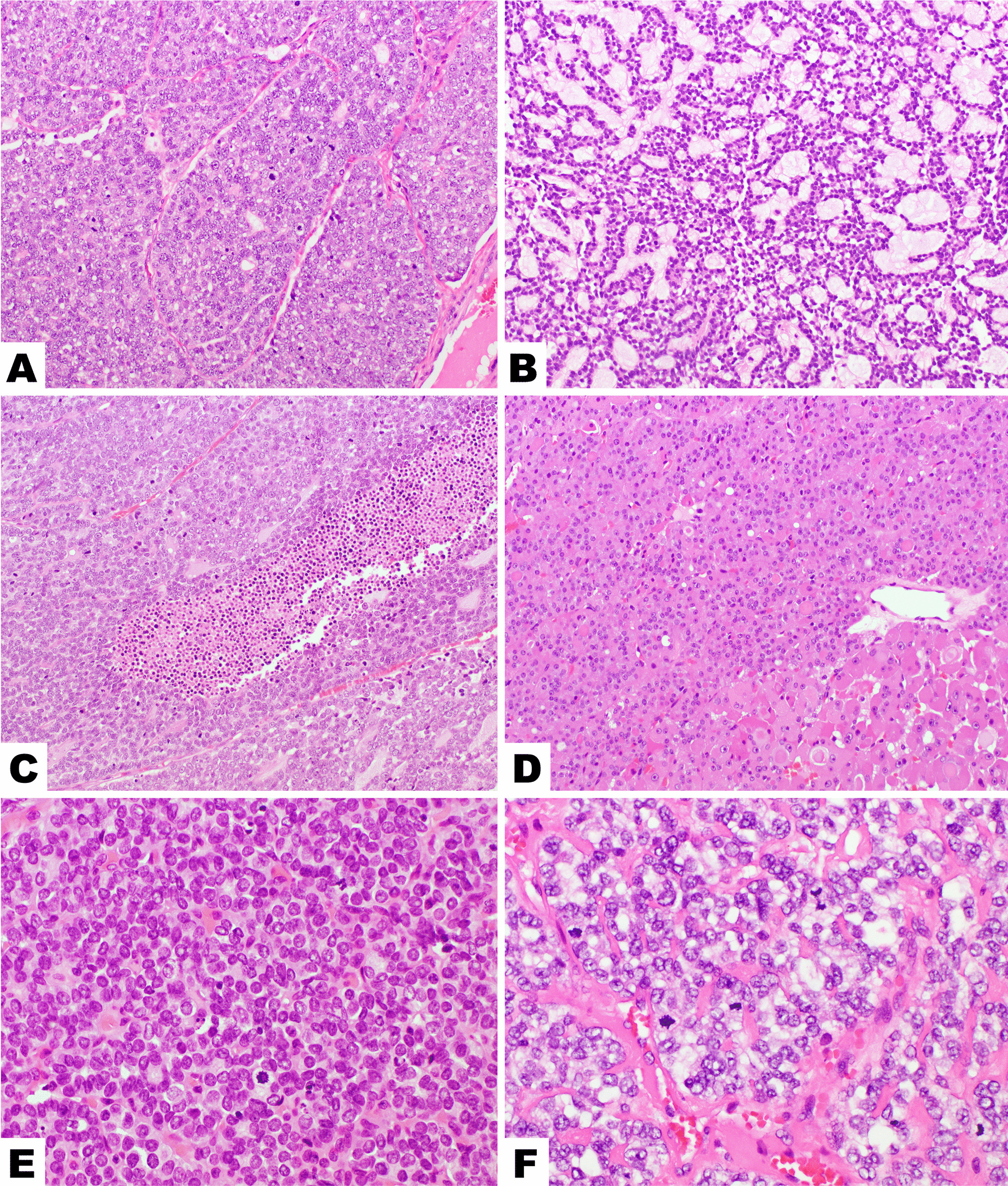
Pancreatic Cases (Patients 1–3)Patient 1, a 59-year-old male, presented with abdominal pain and weight loss. He was found to have a 15 cm heterogeneously enhancing pancreatic mass and multiple liver masses on a CT scan. Biopsy of a liver mass demonstrated a high-grade NEN with well-differentiated nested morphology, oncocytic cytoplasm, uniform nuclei, a mitotic count of 23 per 2 mm2, and Ki-67 index of 45%, suggestive of G3 NET, but IHC demonstrated aberrant p53 positivity and loss of Rb expression, suggestive of NEC (Supplemental Fig. 1). The patient was started on carboplatin and etoposide followed by Lu177-dotatate PRRT prior to pancreatectomy. Sections of the bulky tumor in the pancreas demonstrated variable morphologies: approximately half of the tumor was highly sclerosed, other areas were trabecular, and other areas demonstrated nested architecture within the hyalinized stroma and scattered pleomorphic nuclei, but mitoses were rare (Fig. 1; Supplemental Fig. 1). In the pleomorphic areas, the Ki-67 index was 6.5%, p53 staining was wild-type, Rb protein was intact, and p16 staining was absent (Fig. 1e–h), consistent with G2 NET. High-grade metastases were identified in two peri-pancreatic lymph nodes. The metastases had nested architecture, but some nests were larger and irregular; tumor cellularity, nuclear-to-cytoplasmic ratio, and mitoses were markedly increased compared with the primary pancreas tumor, and nuclear atypia was also increased (higher nuclear size, more hyperchromasia) (Fig. 1i). Thus, this neoplasm had some NEC-like features, but also some NET-like features (nested architecture), and so was considered morphologically ambiguous. One lymph node metastasis had a Ki-67 index of 60% and mitotic count of 59 per 2 mm2 and, like the liver metastasis, demonstrated aberrant positive p53, loss of Rb, and p16 overexpression (Fig. 1m–p). Sequencing of the G2 NET pancreas primarily demonstrated a nonsense mutation in DAXX (p.E221*) and a missense mutation in MEN1 (p.D418Y). Sequencing of the G3 liver metastasis and the G3 lymph node metastasis both showed the identical DAXX mutation (p.E221*) as seen in the G2 pancreas NET. Both liver and lymph node metastases also harbored identical variants in RB1 (p.S780*) and TP53 (p.R158H) not seen in the G2 pancreas NET, which correlated with the Rb loss and aberrant positive p53 seen by IHC in both G3 specimens. Interestingly, the MEN1 variant was not seen in either G3 neoplasm, suggesting loss of the mutant MEN1 locus on chromosome 11q in the G3 neoplasms. None of the three samples was hypermutated. Postsurgical treatment included FOLFOX, radiation, and irinotecan plus cisplatin, but the patient died 8 months after surgery (22 months after initial diagnosis).
Fig. 1
Representative images from patient 1’s low-grade primary pancreatic NET (a–h) and high-grade peri-pancreatic lymph node metastases (i–p). a High-magnification H&E image of the patient’s well-differentiated G2 NET in the pancreas shows the tumor growing in irregular variably sized nests with hyalinized stroma. Tumor cells had predominantly round to ovoid nuclei with salt and pepper chromatin, inconspicuous nucleoli, and rare mitoses, but there was notable pleomorphism with some tumor cells exhibiting larger, more atypical, irregular, and vesicular nuclei, known as degenerative atypia or endocrine atypia. IHC on the pancreas G2 NET demonstrated diffuse expression of b synaptophysin, c chromogranin, and d INSM1. e A Ki-67 index of 6.5%. The G2 NET also demonstrated f wild-type p53 staining, g intact Rb expression, and h essentially absent p16 expression. A high-grade peripancreatic lymph node metastasis (i–p) still maintained a predominantly nested growth pattern though some nests were larger and irregular as seen in panel i and tumor cellularity was increased with a higher nuclear-to-cytoplasmic ratio. Tumor cell nuclei were still predominantly round to ovoid but were slightly larger and darker than the G2 NET in the pancreas and mitoses were frequent; scattered large pleomorphic cells were still present. This high-grade lymph node metastasis also demonstrated diffuse expression for j synaptophysin, k chromogranin, and l INSM1 and had a m Ki-67 index of 60%, n aberrant-positive p53 staining, o loss of Rb expression, and p overexpression of p16
Patient 2, a 50-year-old female, had a longstanding history of pancreatic G2 NET with liver metastases since the time of initial NET diagnosis. High-grade progression was seen on the biopsy of a fast-growing liver metastasis 13.3 years after initial diagnosis. She received numerous treatments for NET in the years preceding high-grade progression, including surgical resection, octreotide, bevacizumab, everolimus, lanreotide, liver embolization, pembrolizumab, sunitinib, and transarterial chemoembolization (TACE). Sections of the high-grade neoplasm (Fig. 2j–k) showed well-differentiated morphology with nested and trabecular architecture, delicate vasculature, and monotonous ovoid nuclei resembling the initial primary pancreatic G2 NET (Fig. 2a–b), with the only significant difference on H&E stain being a brisk mitotic count of 44 mitoses per 2 mm2. Immunohistochemistry performed on the pancreas primary and high-grade liver metastasis demonstrated a marked increase in the Ki-67 labeling index from 7% in the primary to 82% in the G3 NEN. Furthermore, while the primary had wild-type p53, intact Rb, and patchy p16 (Fig. 2g–i), the high-grade liver metastasis demonstrated aberrant positive p53, loss of Rb, and overexpression of p16 (Fig. 2p–r). Sequencing of the G3 liver metastasis demonstrated mutations in ATRX, MEN1, TP53, and RB1 without hypermutation. The patient was treated with carboplatinum and etoposide and then everolimus after high-grade progression, but passed away 11 months later.
Fig. 2
Representative images from patient 2’s low-grade primary pancreatic NET (a–i) and high-grade liver metastasis (j–r). Patient 2’s low-grade G2 pancreatic NET demonstrated trabecular architecture (a–b), diffuse c synaptophysin, d chromogranin, e keratin expression, and f Ki-67 proliferative index of 7%. IHC for g p53 was wild-type, h Rb was intact, and i p16 was patchy. A high-grade liver metastasis was biopsied 13 years later and demonstrated j–k similar well-differentiated morphology with trabecular and nested architecture and moderate eosinophilic cytoplasm, uniform ovoid nuclei with small nucleoli and frequent mitoses. IHC demonstrated diffuse l synaptophysin, m chromogranin, and n cytokeratin 8/18 expression. This liver metastasis had o Ki-67 index of 82%, p aberrant positive p53 staining, q loss of Rb expression, and r p16 overexpression
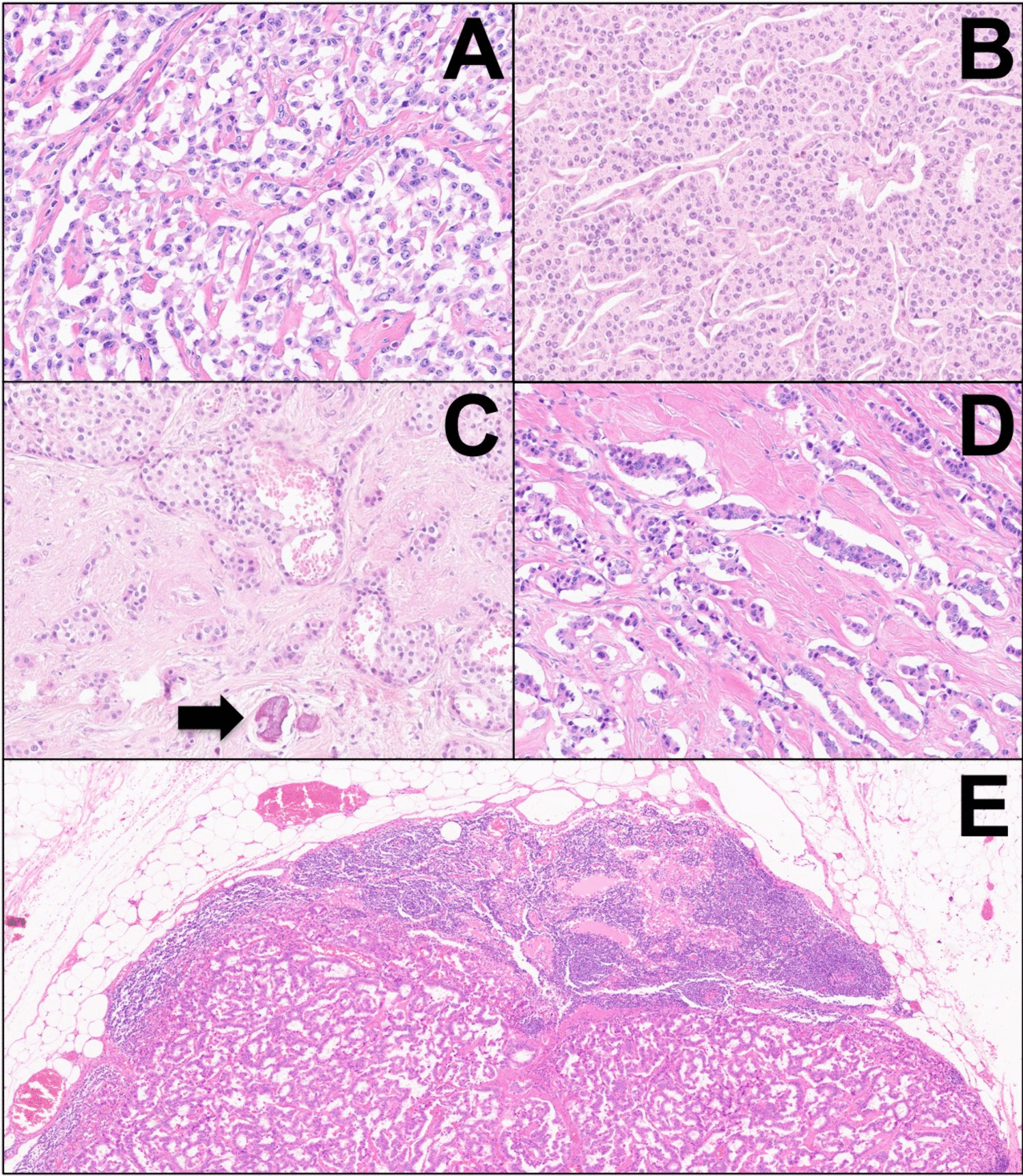
Patient 3, a 57-year-old man, similarly had a longstanding history of metastatic pancreatic low-grade NET many years prior to high-grade progression. His initial primary pancreatic NET was G1 at diagnosis (Fig. 3a–e); his first lymph node (Fig. 3f–g) and liver metastases were G2 when resected 8 months after his pancreas resection and 11 years prior to having high-grade progression documented on fine needle aspiration (FNA) biopsy of a fast-growing liver metastasis (Fig. 3h–n). He received numerous treatments for NET in the years preceding high-grade progression, including surgical resection, octreotide, liver microwave ablation, liver Y90 selective internal radiation therapy (SIRT), everolimus, liver TACE, sunitinib, and capecitabine/temozolomide. The FNA cell block was scant and difficult to evaluate as the neoplastic cells were extensively dissociated. Some neoplastic cells appeared to have plasmacytoid morphology typical of NET (Fig. 3h), but overall, we considered this case not informative regarding morphology due to the limited material. Immunohistochemistry on the cell block demonstrated a Ki-67 index of 94% and a loss of both p53 and Rb (Fig. 3l–n). Sequencing of the G3 liver metastasis demonstrated mutations in ATRX and MEN1 and deep deletions in CDKN2A/2B, TP53, and RB1. Sequencing of a G2 periaortic lymph node metastasis from 11 years prior to high-grade progression demonstrated identical variants in ATRX and MEN1, but no alterations in TP53 or RB1. Neither sample was hypermutated. The patient was treated with capecitabine and temozolomide after high-grade progression but died of the disease 4 months later.
Fig. 3
Representative images from patient 3’s low-grade primary pancreatic NET (a–e), low-grade lymph node metastasis (f–g), and high-grade liver metastasis (h–n). The low-grade G1 pancreatic NET had a a trabecular growth pattern, diffuse b synaptophysin, c chromogranin, d keratin expression, and e Ki-67 index of 2%. Eight months after the pancreas resection, the patient had a periaortic lymph node resection that demonstrated f well-differentiated NET with g Ki-67 index of 5.8%. Twelve years later, a fine needle aspiration biopsy of a liver metastasis demonstrated a high-grade neuroendocrine neoplasm with limited material that was difficult to interpret, though at least some of the tumor cells were plasmacytoid with moderate eosinophilic cytoplasm (h). IHC demonstrated diffuse-positive staining for i synaptophysin, j chromogranin, and k keratin. Although mitoses were not very frequent in the cell block, the Ki-67 index was 94% (l). Additional IHC demonstrated loss of both m p53 and n Rb expression in neoplastic cells
Pituitary Case (Patient 4)Patient 4, a 53-year-old man, underwent resection of a 2.2-cm pituitary mass. Diagnostic workup of the initial resection revealed a low-grade pituitary NET with ACTH expression. Prior to high-grade progression seen in an intracranial metastasis 4.5 years later, the patient was treated with additional resections, as well as Gamma knife radiosurgery. The initial pituitary NET (Fig. 4a–j) demonstrated sheets/trabeculae of uniform epithelioid cells with delicate vasculature, occasional rosettes, rare mitoses, Ki-67 index of 6%, wild-type p53, intact Rb, and absent p16 expression. The patient’s fourth resection (4.5 years later) demonstrated similar well-differentiated morphology though with more numerous rosettes, frequent mitoses, elevated Ki-67 index of 70%, loss of p53 and Rb, and p16 overexpression (Fig. 4k–t). After this high-grade progression, the patient survived for an additional 41 months and was treated with temozolomide and pembrolizumab, but eventually developed cerebrospinal fluid (CSF) metastases and passed away.
Fig. 4
Representative images from patient 4’s low-grade primary pituitary NET (a–j) and high-grade intracranial metastasis (k–t). a High-magnification H&E image of patient 4’s initial well-differentiated pituitary NET demonstrates tumor growth in sheets with occasional rosettes, delicate vasculature, and uniform round to ovoid nuclei with inconspicuous nucleoli and rare mitoses. IHC demonstrated significant positivity for b keratin, c TPIT, d synaptophysin, e INSM1, and f Ki-67 index of 6%. The low-grade NET also demonstrated g intact ATRX expression, h wild-type p53 staining, i intact Rb expression, and j absent p16. Patient 4 had a resection of an k–t intracranial metastasis 4.5 years after initial diagnosis, which had k similar morphologic features to the original pituitary NET, but with more numerous rosettes, mitoses, and apoptotic nuclei. The metastasis demonstrated l diffuse keratin expression with a dot-like staining pattern and m positive but more limited TPIT expression than the primary. n–o Neuroendocrine markers expression was diffuse, and p Ki-67 index was 70%. q ATRX expression was intact; both r p53 and s Rb expression were lost, and t p16 was overexpressed
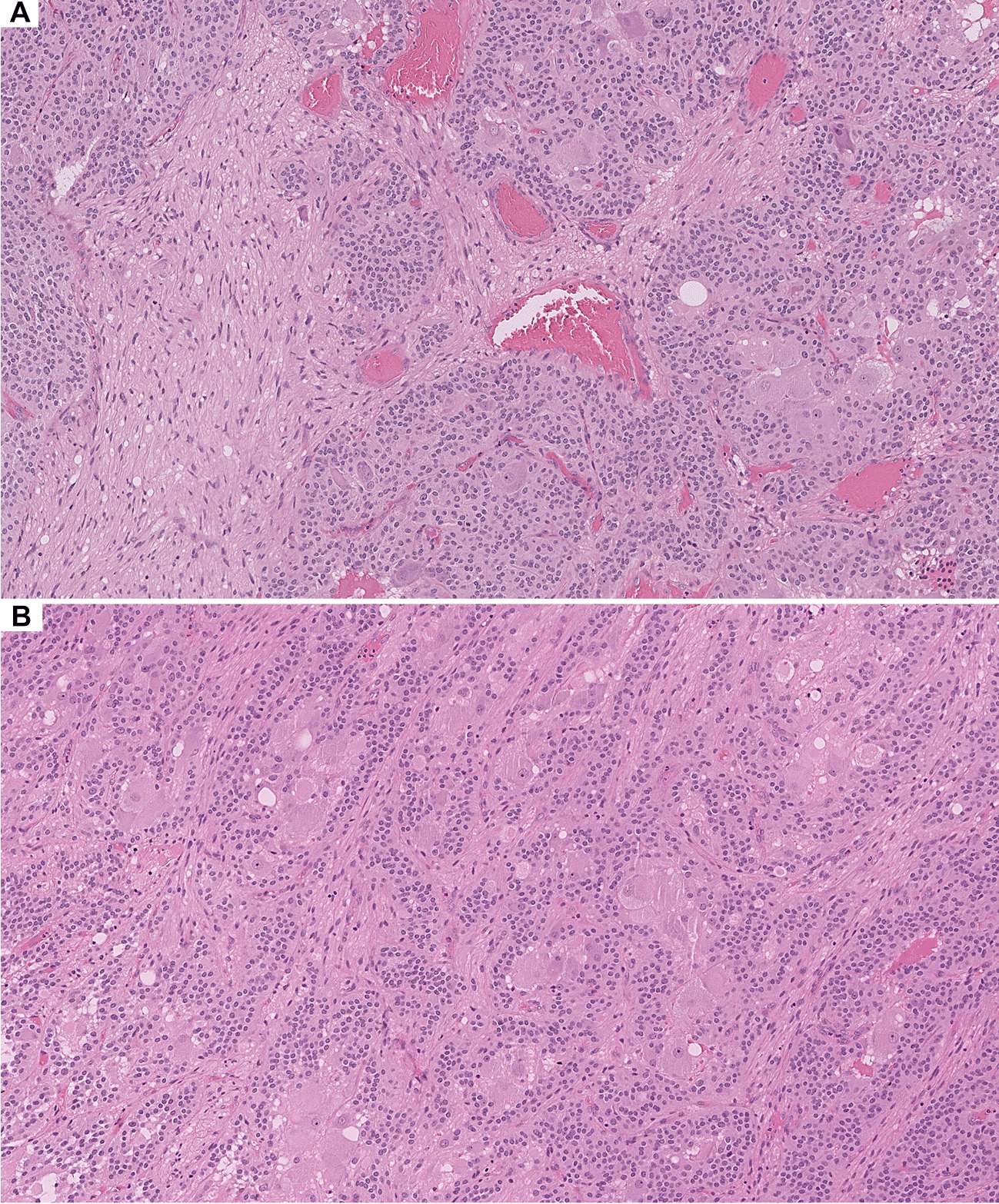
Unknown Primary (Patient 5)Patient 5, a 38-year-old male with Currarino syndrome (germline MNX1 mutation), presented with low back pain and was found to have a pre-sacral mass as well as liver metastases. Biopsy of the pre-sacral mass demonstrated a predominantly G1 NET with a distinct focus of high-grade progression (Fig. 5). The G1 NET component had organoid morphology with growth in nests and ribbons, a Ki-67 proliferation index of 2%, intact Rb, wild-type p53, and patchy p16 staining. The higher-grade component showed increased nuclear atypia (Fig. 5b), proliferation index of 75%, loss of Rb, aberrant positive p53, and p16 overexpression. The high-grade focus had some NEC-like morphologic features; it was surrounded by desmoplastic stroma, and tumor cells had a higher nuclear-to-cytoplasmic ratio and larger more atypical nuclei with increased mitoses compared with the low-grade areas. However, the high-grade tumor cells still had some NET-like architectural features with growth in trabeculae/ribbons, thus still vaguely organoid. Overall, the G3 focus was considered morphologically ambiguous. Similar to patient 1, patient 5 demonstrated G3 NEN progression at the time of initial diagnosis and therefore did not receive any NET-related treatments prior to progression. This patient was treated with cisplatin and etoposide, palliative radiation, and carboplatin/etoposide after diagnosis, but died 12 months post-diagnosis.
Fig. 5
Representative images from patient 5’s presacral mass biopsy with both low-grade and high-grade areas. a and f–i H&E and IHC stains of patient 5’s presacral mass biopsy demonstrating a well-differentiated G1 NET with growth in nests on the right side and a high-grade NEN focus on the left side with a more trabecular but irregular and infiltrative growth pattern. b A high-magnfiication image of the high-grade component only demonstrating increased nuclear atypia characterized by enlarged nuclei with irregular borders, smudgy chromatin, and frequent mitoses. Both components had c diffuse synaptophysin, d focal chromogranin, and e diffuse keratin expression. The low-grade component had f Ki-67 index of 2%, g wild-type p53, h intact Rb, and i patchy-positive p16 expression (wild-type pattern). The high-grade focus on the left side demonstrated c a marked increase in the Ki-67 index at 75%, d aberrant-positive p53 expression, e loss of Rb expression, and f overexpression of p16
Comments (0)