
Remember me
Dear Editor,
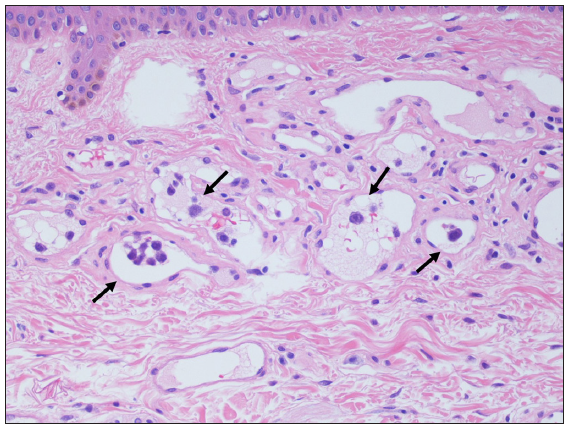
Random skin biopsy is a useful and popular method of taking specimens from mainly normal skin for the diagnosis of intravascular lymphoma. It has been reported that the serum levels of lactate dehydrogenase and soluble interleukin-2 receptor can be a selection criterion for random skin biopsy,1–4 although they can be high in other diseases. Random skin biopsy may occasionally be performed on patients with potential diseases other than intravascular lymphoma.1-3 In this study, we evaluated patients who underwent random skin biopsy in our department to assess the association between final diagnosis and the serum levels of lactate dehydrogenase and/or soluble interleukin-2 receptor. Fifty Japanese patients, who underwent random skin biopsy between April 2010 and February 2024, were enrolled. Clinical symptoms, laboratory data and final diagnosis were reviewed by the medical records. In most patients, the three biopsy sites were the abdomen and the bilateral anterior thighs.3,4 If a senile haemangioma was present in the areas, the biopsy specimen included it [Figure 1].3,5 Statistical analysis was performed using PASW Statistics (version 18.0; SPSS INC., Chicago, IL, USA).
Export to PPT
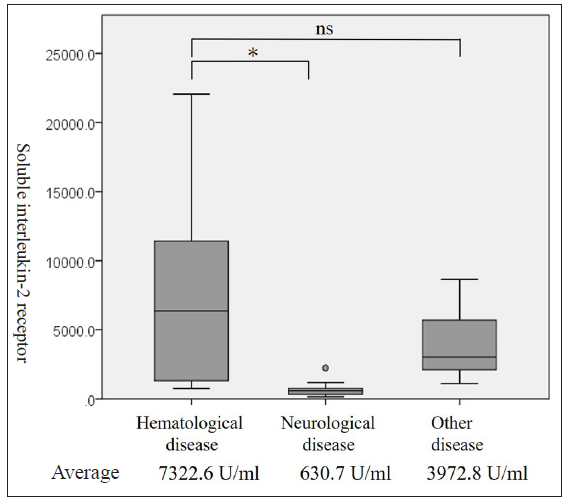
Eight of the 50 patients were diagnosed with intravascular lymphoma histologically [Table 1]. Seven of the eight patients were diagnosed with intravascular large B cell lymphoma and the eighth was diagnosed with intravascular T cell lymphoma. The final diagnosis in the negative group of random skin biopsy was a haematologic disease diagnosed by the other tissue specimens in six cases. Only one of the six cases in the negative group of random skin biopsy was diagnosed with intravascular large B cell lymphoma by the specimen from bone marrow. The 26 out of the remaining cases were diagnosed with neurological disease, including multiple cerebral infarction (four cases) and glial fibrillary acidic protein astrocytopathy (three), and ten cases were diagnosed with other diseases, including thrombocytopenia, anasarca, fever, reticulin fibrosis and organomegaly syndrome (TAFRO syndrome) (two), and adult Still disease (two). The levels of lactate dehydrogenase and soluble interleukin-2 receptor were significantly higher in the haematological disease than in the neurological disease in the Mann-Whitney U test. However, the levels of lactate dehydrogenase and soluble interleukin-2 receptor were not significantly different between the haematological disease and other diseases [Figure 2a and 2b].
Table 1: The breakdown of the random skin biopsy-positive patients
Age Sex Senile haemangioma in biopsy sites Intravascular lymphoma-positive senile haemangioma Number of intravascular lymphoma-positive specimens Fever Abnormal haematology Lactate dehydrogenase level (U/L) Soluble interleukin-2 receptor level (U/mL) Neurological symptoms 76 Male - 1 + Anaemia 364 1870 + 81 Female - 1 + Thrombocytopenia 1029 15,000 + 80 Female + + 1 + Anaemia thrombocytopenia 684 8148 - 74 Male + + 1 + Anaemia thrombocytopenia 960 7128 - 74 Male - 3 - Thrombocytopenia 717 1315 - 73 Male + - 2 + Anaemia thrombocytopenia 493 11,428 + 55 Male - 2 - Pancytopenia 3676 969 + 72 Female + + 2 - Pancytopenia 876 5627 +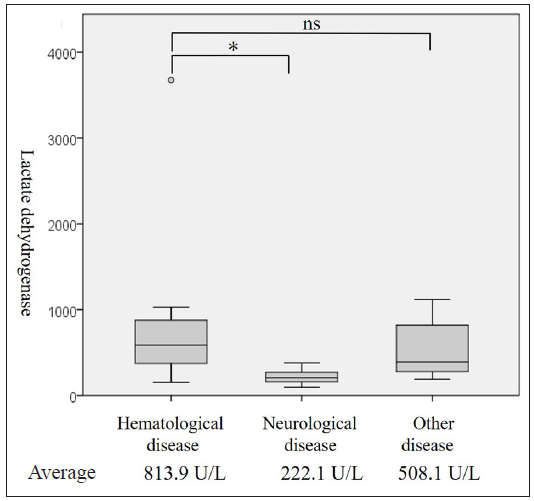
Export to PPT
Export to PPT
In general, while random skin biopsy is requested by haematologists or neurologists, the positive rate is never high.1,2,4,6 In this study, the positive rate of random skin biopsy was 16%. The patients with negative random skin biopsy were frequently diagnosed with neurological disease in this study. In previous reports,1–3 patients with negative random skin biopsy were diagnosed with infectious disease, collagen disease or others, in addition to neurological diseases. Neurological disease presented with low levels of both lactate dehydrogenase and soluble interleukin-2 receptor in this study. However, it is appropriate to perform random skin biopsy if levels of both lactate dehydrogenase and soluble interleukin-2 receptors are high in addition to neurological symptoms. Five of the eight random skin biopsy-positive patients developed neurological symptoms, including consciousness disturbance, hand tremor, dysarthria and paraplegia.
Sumi-Mizuno et al4. in their study reported that serum soluble interleukin-2 receptor levels were over 2000 U/mL for all random skin biopsy-positive patients. Matsue et al2. reported the level of lactate dehydrogenase > 800 U/L or the level of soluble interleukin-2 receptor > 5000 U/mL as predictors for random skin biopsy positivity. In the case series by Shimada et al.,7 they reported that 104 of the 106 intravascular large B-cell lymphoma patients presented with a high level of lactate dehydrogenase, and 63 of the 96 intravascular large B-cell lymphoma patients presented with a high level (>5000 U/mL) of soluble interleukin-2 receptor. In this series, the minimal levels of lactate dehydrogenase and soluble interleukin-2 receptor in the positive group for random skin biopsy were 364 U/L and 969 U/mL, respectively. If a haematologist or neurologist requests random skin biopsy for cases with higher levels of lactate dehydrogenase and soluble interleukin-2 receptor than reference ones, we believe that it is necessary to perform random skin biopsy regardless of the absolute levels of lactate dehydrogenase and soluble interleukin-2 receptor.
Limitations of this study include the limited number of patients and single centre study. In addition, insufficient consideration for the potential comorbid conditions that may influence the levels of lactate dehydrogenase and soluble interleukin-2 receptor.
In conclusion, since levels of both serum lactate dehydrogenase and soluble interleukin-2 receptor are significantly higher than reference ones in patients with haematological disease, including random skin biopsy-positive intravascular lymphoma, low levels of lactate dehydrogenase and/or soluble interleukin-2 receptor may be a sign that examination of neurologic disease should be a priority before performing random skin biopsy.
Comments (0)