
Remember me

We have carefully reviewed the article titled “Risk of pneumonia-related hospitalization after initiating angiotensin-converting enzyme inhibitors compared with angiotensin II receptor blockers: a retrospective cohort study using LIFE Study data” by Ryosuke Uemura et al. [1], which presents an intriguing comparison between ACEIs and ARBs in the context of pneumonia-related hospitalization risk. While the study provides valuable insights, I have identified several areas that could benefit from further clarification or methodological refinement.
Firstly, the study’s reliance on claims data, while pragmatic for a retrospective cohort study, may introduce potential biases and inaccuracies in both the exposure and outcome ascertainment [2]. It would be beneficial if the authors could discuss the possible impact of such data limitations on their findings and how they might affect the internal validity of the study. Secondly, while the Fine-Gray method is appropriately used to account for death as a competing risk in the Cox proportional hazards model, it would be informative to understand more about the proportional hazards assumption. The authors should provide evidence or diagnostic tests to confirm that this assumption holds true throughout the study period [3]. Thirdly, while propensity score matching was used to balance the covariates between the ACEI and ARB groups, the adequacy of this matching should be assessed statistically [4]. The authors should present balance diagnostics, such as standardized mean differences or t-tests, to demonstrate that the covariates are well-balanced after matching.
In terms of covariates, the study adjusted for a range of demographic and clinical factors. However, the potential influence of unmeasured confounders such as smoking status, influenza vaccination, and socioeconomic status cannot be overlooked [5]. The authors have conducted a sensitivity analysis to address this, but a more detailed discussion on these unmeasured variables and their potential impact on the study’s conclusions would be valuable. Another area for improvement is the handling of missing data. The study does not provide details on the mechanism of missingness or the potential impact of missing data on the analysis [6]. A more comprehensive approach to handling missing data, such as multiple imputation or pattern-mixture models, could have been employed to assess the robustness of the results.
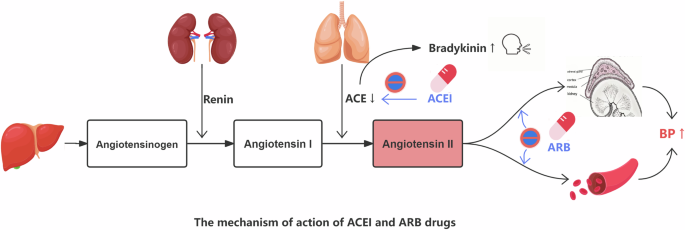
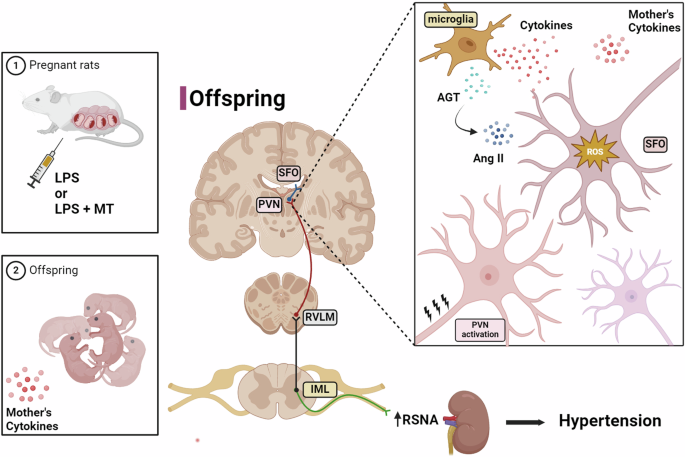
Lastly, the study’s conclusion states that there is no significant preventive effect of ACEI initiation against pneumonia-related hospitalization. While this conclusion is supported by the data presented, it would be beneficial to discuss the biological plausibility of ACEIs potentially reducing pneumonia risk through the induction of a dry cough (Fig. 1) and the implications of these findings for clinical practice and future research [7].
Fig. 1
The mechanism of action of ACEl and ARB drugs
In conclusion, Uemura et al.‘s study contributes to the literature on ACEIs and ARBs in relation to pneumonia risk. However, the points raised above, if addressed, could further strengthen the study’s methodology and the confidence in its findings.
Comments (0)