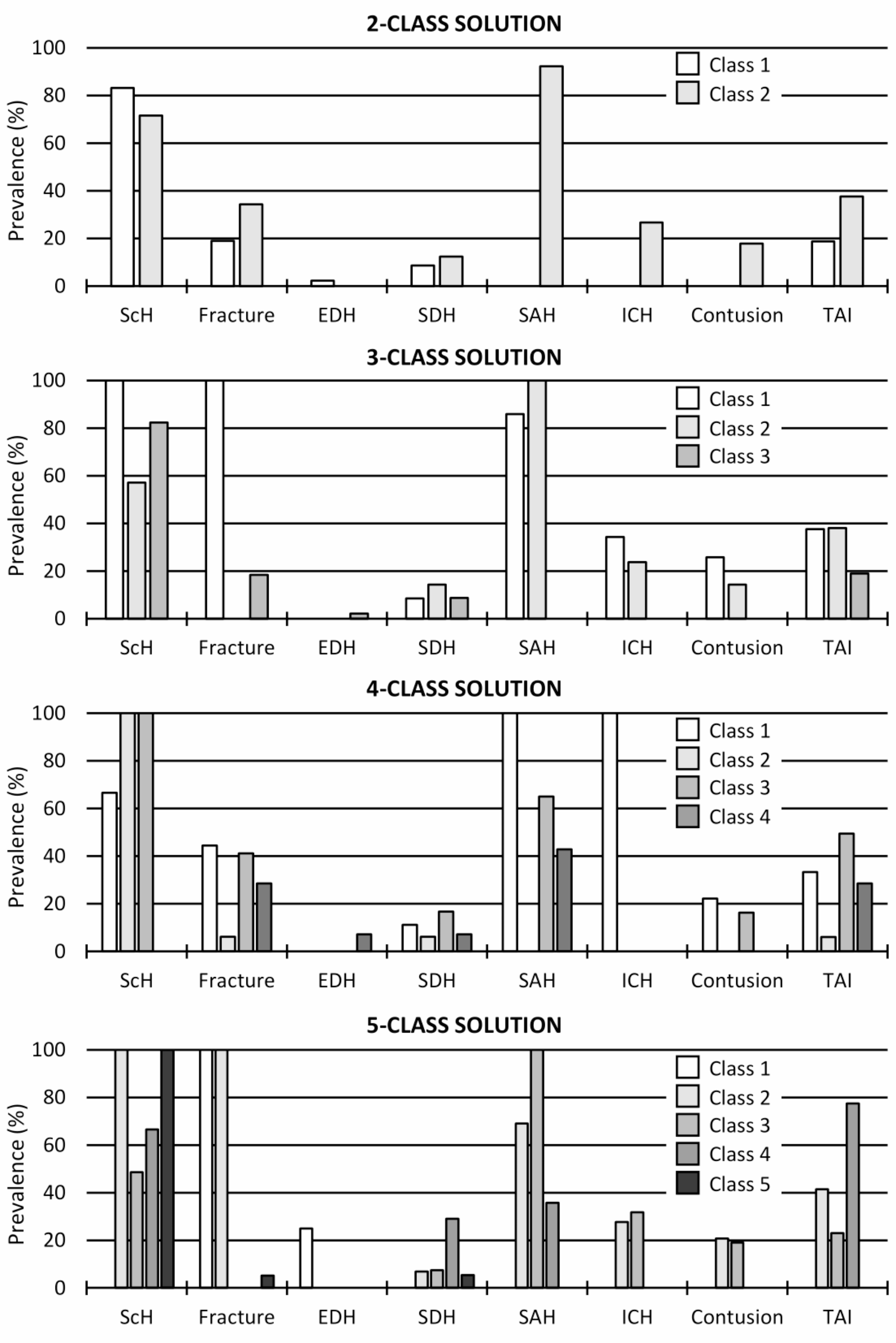
A total of 78 neuropathologically examined medico-legal autopsy cases, all of whom had suffered a head injury prior to death, were involved in this study. The objectives were to describe the application of LCA in a medico-legal TBI dataset, and to report the best-fitting latent class solution in the present dataset. Latent class solutions with two to five classes were explored. The complexity of the models increased along with the number potential of classes. In this relatively small dataset, the two-class solution showed the best fit statistics and was selected as the final solution. The two classes of the final model showed distinct characteristics and statistically significant differences in the prevalences of underlying CNS disease, SAH, intracerebral/ventricular haemorrhage and contusion. As such, our analysis gives grounds for several remarks.
This study is among the first to apply LCA in a forensic neuropathology and medico-legal TBI context. As certain TBI subtypes are more likely to co-occur than others (e.g. fractures, SDH and SAH in road traffic fatalities [7], or SDH and dTAI in acceleration-deceleration scenarios [4]), further data on typical brain injury combinations could expedite cause-of death investigations and potential judicial proceedings in TBI cases. These aspects provide us with a theoretical justification for the explorative application of LCA in the forensic neuropathology context.
In our dataset, the latent class solutions appeared reasonable from the practical point of view; each class appeared to represent a distinct TBI profile. As is often the case, the models became more complex as the number of classes was increased [15]. The two-class solution showed the best fit statistics and was selected as the final model. Of note is the fact that our dataset was relatively small and our primary injury variables were dichotomous; the present solution should not be interpreted as “ground truth”, but instead further research is needed. Multicenter efforts with detailed TBI variables (e.g. estimation of survival time by means of immunohistochemical stains [17]) may produce valuable datasets for future use. Future research should also aim to take into account the location, accumulation, severity and extent of head injuries. However, as the two-class solution was selected as the best for the present dataset, we introduce its classes and discuss the class differences below.
As for medical history, underlying CNS disease was more prevalent in Class 1, affecting 52.2% of the cases. The association between accidental deaths and CNS diseases, particularly Alzheimer’s and vascular dementia, has been shown previously [18]. Neurological and cognitive impairment significantly affect balance predisposing patients to falls [19]. Similarly, these impairments may affect driving ability, increasing the risk of traffic accidents. Previous research has identified older age combined with a CNS disease as a significant risk factor to falls [19], consistent with our finding of a 10-year higher median age in Class 1.
The circumstance of the recent head injury was often assault or traffic accident in Class 2, possibly indicating a greater force of trauma than in Class 1, in which falls and unspecified circumstances prevailed. We speculate that undocumented events mainly comprise fragile patients’ simple falls at home, which are not reported to the healthcare services and, consequently, do not appear in our records. However, our dataset did not differentiate between falls from different heights, which prevents us from determining whether the falls in Class 2 could have been more severe and have caused worse injuries. In general, we speculate that cases in Class 2 have encountered on average greater traumatic forces, leading to more diverse primary head injury combinations.
SAH was a prominent finding in Class 2, affecting 96.9% of the cases. Acceleration, deceleration and twisting movement are typical causes of SAH that may present in varying severity, intensity and distribution [2]. In previous studies, SAH has been the commonest injury in falls [20], assaults [21], homicides [22], and traffic accidents [23, 24]. However, no significant differences in the incidence of SAH between the injury circumstances have been found [20].
Consistent with the observations in this study, contusion and SAH are associated with each other [2]. Similar to SAH, contusions were seen in Class 2 only, affecting 18.8% of the cases. Contusion has been reported to be more prevalent in traffic accidents than falls [20], which corresponds to our findings indicating that contusions were only observed in Class 2, where traffic accidents were more prevalent. Moreover, traumatic intracerebral/ventricular haemorrhage was solely seen in Class 2, with a prevalence of 28.1%. Both intracerebral and intraventricular hemorrhages are associated with dTAI and mainly observed in severe head injuries [2]. This and previous research [25] align with our hypothesis on the potentially greater traumatic forces encountered by the cases of Class 2.
Knowledge on typical injury combinations related to specific circumstances and case profiles could facilitate the work of police and forensic pathologists estimating the course of events leading to a person’s unnatural death. For clinicians, knowledge of co-occurring injuries may provide the opportunity to make evidence-based predictions and treatment decisions, aiming to prevent disability and death.
A strength of the study were the comprehensive neuropathological examinations performed by a board-certified neuropathologist. The dataset comprised medical history, general circumstances of TBI, as well as primary and secondary head and brain injuries documented during the general autopsy and neuropathological examination, enabling comparisons between classes. Additionally, LCA provided an objective approach to the dataset; it has rarely been utilized as a statistical method in forensic neuropathology before. The main limitations were the relatively small sample size and lack of details on the severity and extent of head injuries. Unfortunately, specific details on injury circumstances were also limited; for example, falls from significant height and from standing position were grouped into the same category, and the detailed mechanisms of assaults were not available to us. Finally, we did not have data on injuries to other parts of the body than the head.





Comments (0)