
Remember me





The current study was conducted in Immunology and Molecular Medicine in collaboration with the Department of Internal Medicine, Division of Rheumatology, Sher-I-Kashmir Institute of Medical Sciences (SKIMS), Soura, Srinagar (J&K), a tertiary care referral hospital in North India. Proformas were used to document clinical characteristics at the time of evaluation.
Inclusion and exclusion criteriaA total of 50 naïve SSc cases were recruited into the study. At the entry, patients were profiled into dcSSc and lcSSc subgroups linked to distinct clinical consequences and prognoses were made at the point of admission using the criteria proposed by Van den Hoogen et al. 2013 and updated by the European League Against Rheumatism [2]. All the patients followed American Rheumatological Criteria in our study, and hospital investigations were used to determine the clinical profile of these individuals. Following internationally agreed guidelines, SSc was defined. SSc with skin injury can be classified as either limited cutaneous SSc (lcSSc), in which the injury does not go beyond the elbows and knees, or diffuse cutaneous SSc (dSSc) in which skin injury affects the proximal limbs, trunk, and/or both. Standard assessment exams include respectively: Rodnan score, cardiac ultrasound, lung CT scan, PFT, and capillaroscopy. Sc-ILD was defined by a combination of specific HRCT images of at least 10% of all parenchyma (reticulations, honeycombing and/or ground glass opacities) with clinical signs or symptoms (cough, shortness of breath) and alteration of PFTs. Following multiple discussions with clinicians, all cases were validated to determine whether or not SSc-ILD was present. Echocardiography, the forced vital capacity (FVC)/ diffusion capacity for carbon monoxide ratio (DLCO) were used to achieve early diagnosis of SSc-PAH. All of the patients’ clinical, laboratory, and demographic information was recorded using our standard protocol. The anti-topoisomerase I (ATA), anti-centromere antibody (ACA), and anti-nuclear antibody (ANA) data of an autoantibody profile in SSc patients were obtained from the test results of the patients.
The study excluded immunosuppressed patients, those with overlapping syndromes (SSc with Systemic lupus erythematosus or SSc with Rheumatoid arthritis), and also pregnant or nursing women.
Control subjectsThirty healthy Kashmiri volunteers who were matched for age, geographical region, gender, and ethnicity and had no history of autoimmune, inflammatory, or other disorders were included in the study.
Isolation of primary human peripheral blood mononuclear cellsAfter the diagnosis, peripheral blood was extracted by venipuncture, collected into ethylenediaminetetraacetic acid (EDTA) tubes, centrifuged for 10 min at 1500× g at 4 °C by using density centrifugation using Ficoll (Ficoll Isopaque, HIMEDIA).
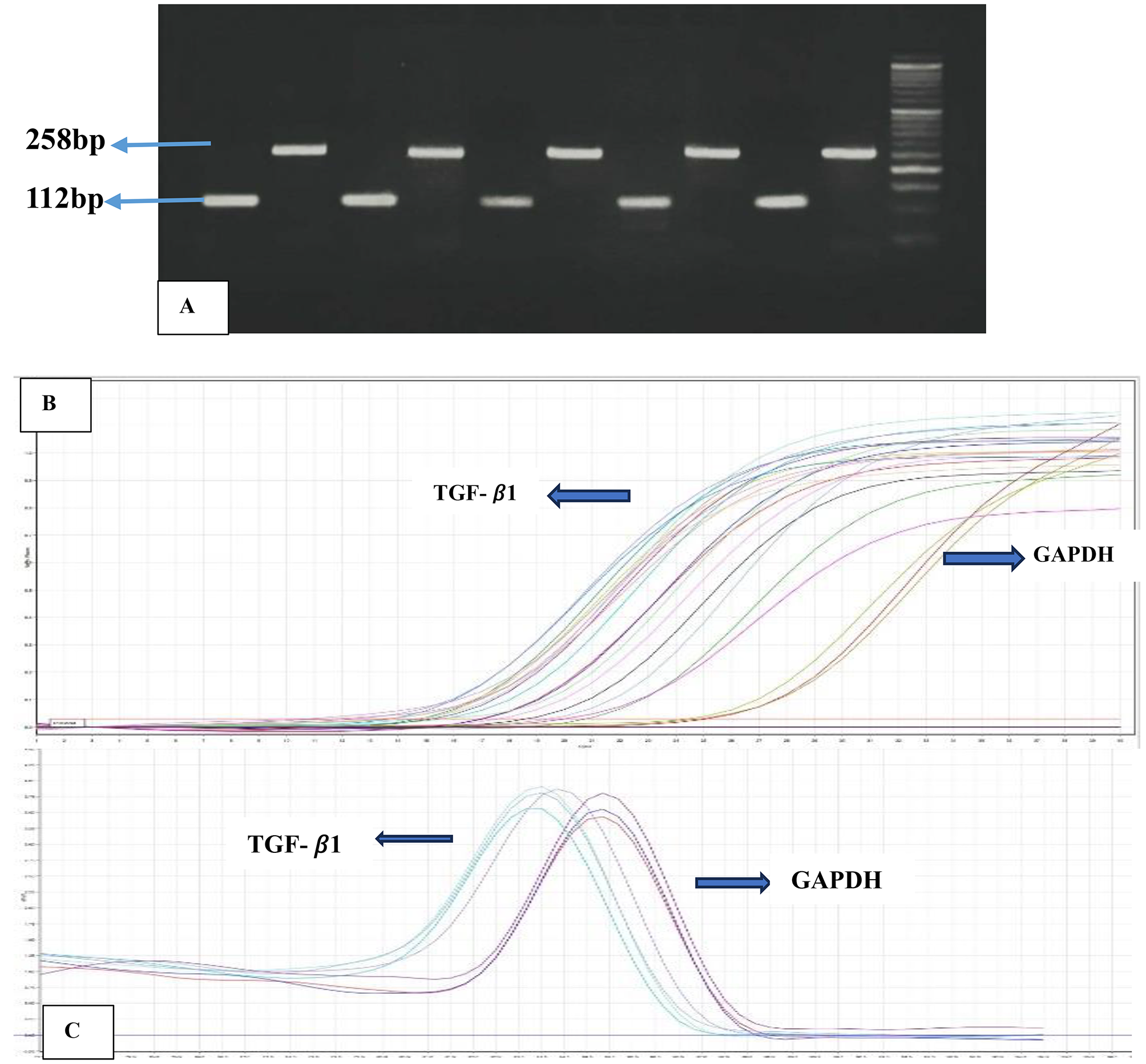
RNA isolation and real-time polymerase chain reaction (qRT-PCR)In both cases and controls, total RNA was isolated from Primary Human PBMCs using TRIzol (Invitrogen), as per the manufacturer’s instructions. After extraction, DNA contamination was removed by using DNase treatment (ThermoScientific). Relative absorbance values (A260/280) were used to evaluate the extracted RNA’s purity, and the ratio was found to be ~ 2. The extracted RNA’s integrity was checked on a 1% Agarose gel prepared in DEPC-treated water. 200 ng/sample of total RNA was reverse transcribed, by using the Maxima First strand cDNA synthesis kit (ThermoScientific K1641) as directed by the manufacturer. After that, by using gene-specific primers, 2 ul of cDNA as a template, and Maxima SYBR Green/ROX qPCR Master Mix (Thermo Scientific K0221), TGF-β1 mRNA levels were determined by quantitative real-time Polymerase Chain Reaction (qRT-PCR) (Rotor-Gene Qiagen thermocycler). Primer concentration and annealing temperature were first standardized by a routine gradient PCR utilizing cDNA as a template. The absence of non-specific amplification products and primer dimers was ensured for proper quantification. To determine the relative expression of each target for the qPCR data analysis, the internal GAPDH expression level was normalized using the 2−ΔΔCt method [18]. GAPDH was selected as the reference gene as it showed a lesser deviation of Ct values as compared to the other two housekeeping genes- β-actin and HPRT that were tested in our study. The successful RT-PCR amplification was assessed by resolving the amplicon on 3% agarose gel shown in Fig. 1A and the amplification plot is shown in Fig. 1B). A post-amplification melting-curve analysis was performed (Fig. 1C) to ensure reaction specificity and assess real-time PCR reactions for primer-dimer artifacts. Representative pictures of TGF- β1 qPCR analysis are shown in Fig. 1.
Fig. 1
Representative pictures of TGF-β1 qPCR analysis in 50 SSc cases: A-qPCR post amplification gel picture of TGF-β1 (112bp) and GAPDH (258bp), lane M: 100bp marker. B-Amplification plot of TGF-β1 and GAPDH. C-Melting curve analysis of TGF-β1 and GAPDH
Assessment of serum TGF-β1 levelsBlood samples were centrifuged and serum was separated from the samples. Before usage, all serum samples were kept at -70∘C. Using a particular ELISA kit, the amounts of active TGF-β1 in serum and culture supernatants were measured per the manufacturer’s instructions (DRG, UK). As directed by the manufacturer, serum samples were acidified with HCl for one hour while being run in duplicate. This enables the release of the naturally active form of TGF-β1 from the biologically inactive complex that is created when a mature TGF-β dimer and a second dimer (latency-associated protein) bind non-covalently.
Statistical AnalysisPrism 8 software (Graphpad Inc., San Diego, USA) and SPSS version 21.0® (IBM, Chicago, USA) were used for data analysis. The parametric tests (student t-test and one-way ANOVA were used to assess the statistically significant difference among two and multiple groups, respectively), and the Shapiro-Wilks test was used to confirm the normality of the samples. Serum cytokine levels were compared using the Mann-Whitney U test. The correlation between the variables was assessed using the Pearson or Spearman correlation test. A statistical significance threshold of 5% (p < 0.05) was used.
Comments (0)