Data
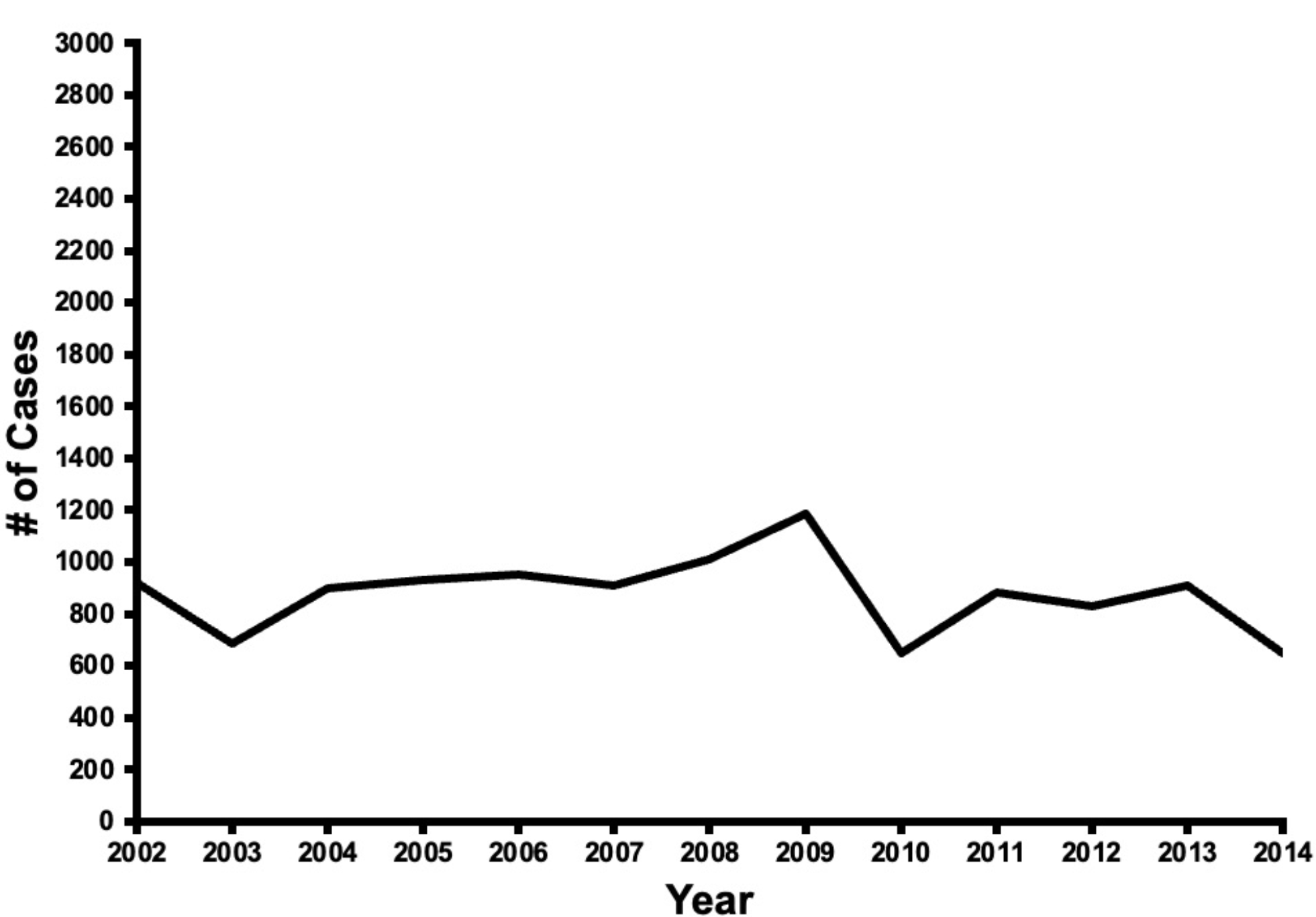
The National Inpatient Sample (NIS) Healthcare Cost Utilization Project (HCUP) database is the largest all-payer inpatient discharge database and represents a 20% stratified sample of all discharges occurring in a given year. This cross sectional analysis of the NIS was queried from 2002 to 2014 for patients undergoing cardiovascular surgery in the United States, specifically coronary artery bypass grafts (CABG), valve procedures, aortic procedures, or multi-component procedures. Patients were identified using the 2003 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis and procedure codes. Patients undergoing CVS and dementia were identified based on ICD-9-CM codes. The Institutional Review Board at Cleveland Clinic determined that the use of NIS publicly available data does not contain any identifiable information and is not considered “human subject research” and therefore does not require IRB approval.
Outcomes
Outcomes included in-hospital mortality, complications, length of stay (LOS), discharge disposition, and hospitalization cost. Complications included stroke, blood transfusion, infection, pneumonia, cardiac syndrome, respiratory, PE, DVT, gastrointestinal syndromes, mental disorder, ventilation, pain, and sepsis and were identified through secondary ICD-9 codes. Discharge disposition was defined as routine discharge to home, home with home healthcare, transfer to another inpatient facility, and transfer to another facility (e.g. long-term acute care and skilled nursing facilities). Hospitalization costs were adjusted for inflation and converted to 2019 US dollars using the Consumer Price Index.
Covariables
Patient characteristics included age, sex, race, admission status, median household income, insurance status, and comorbidities. Admission status was categorized as elective or urgent.
To stratify for surgical risk, comorbidities were derived from secondary ICD-9-CM diagnosis codes using The Elixhauser Comorbidity Score (ECS) [9]. ECS was applied instead of the risk score stratification suggested by the Society of Thoracic Surgeons (http://riskcalc.sts.org/stswebriskcalc/#/calculate), because the latter risk analysis implements variables that may not appear in the ICD-9 diagnosis code-based NIS database. For our investigation, patients were stratified by ECS into low (0–5), medium (6–15), and high-risk (> 15) categories.
Hospital-level characteristics included hospital location, bed size, teaching status, and ownership. Hospital region was classified as Northeast, Midwest, South, or West according to the United States Census Bureau. Hospital bed size was classified as small, medium, or large based on an HCUP-developed algorithm.
Statistical analysis
Chi-square tests were calculated to compare categorical variables. To assess linear trends of complications over time (years), the Mantel-Haenszel Chi-square test was used. All P-values were two-tailed and P < 0.05 was considered significant.
Patients with dementia undergoing CVS were compared to those without dementia. To adjust for possible confounding covariates, One to one greedy propensity score matching (PSM) with a caliper of 0.1 times the mean of the standard deviation of log propensity score was used to balance the groups. The model was constructed using a forward selection algorithm, with patient demographic variables and hospital volume, as a categorical variable, forced into the model. All other terms with a multivariate regression P > 0.05 were excluded from the model. To account for clustering of cases at the hospital level, the final model was constructed as a hierarchical model, in which a grouping term for hospitals was entered as a random effect. Patient-level predictor variables included patient demographics, (age, gender, and race as categories), comorbidities, and prior cardiac procedures as determined by secondary diagnoses for admission. The final propensity matched cohort included 11,294 pairs of patients with and without dementia who were well-matched. Outcomes between the dementia group and non-dementia group using differences in means with paired t tests and conditional logistic regression for in-hospital mortality and complications. Weighted estimates are reported throughout. All statistical analyses were performed with SAS.

Comments (0)