Study Participants
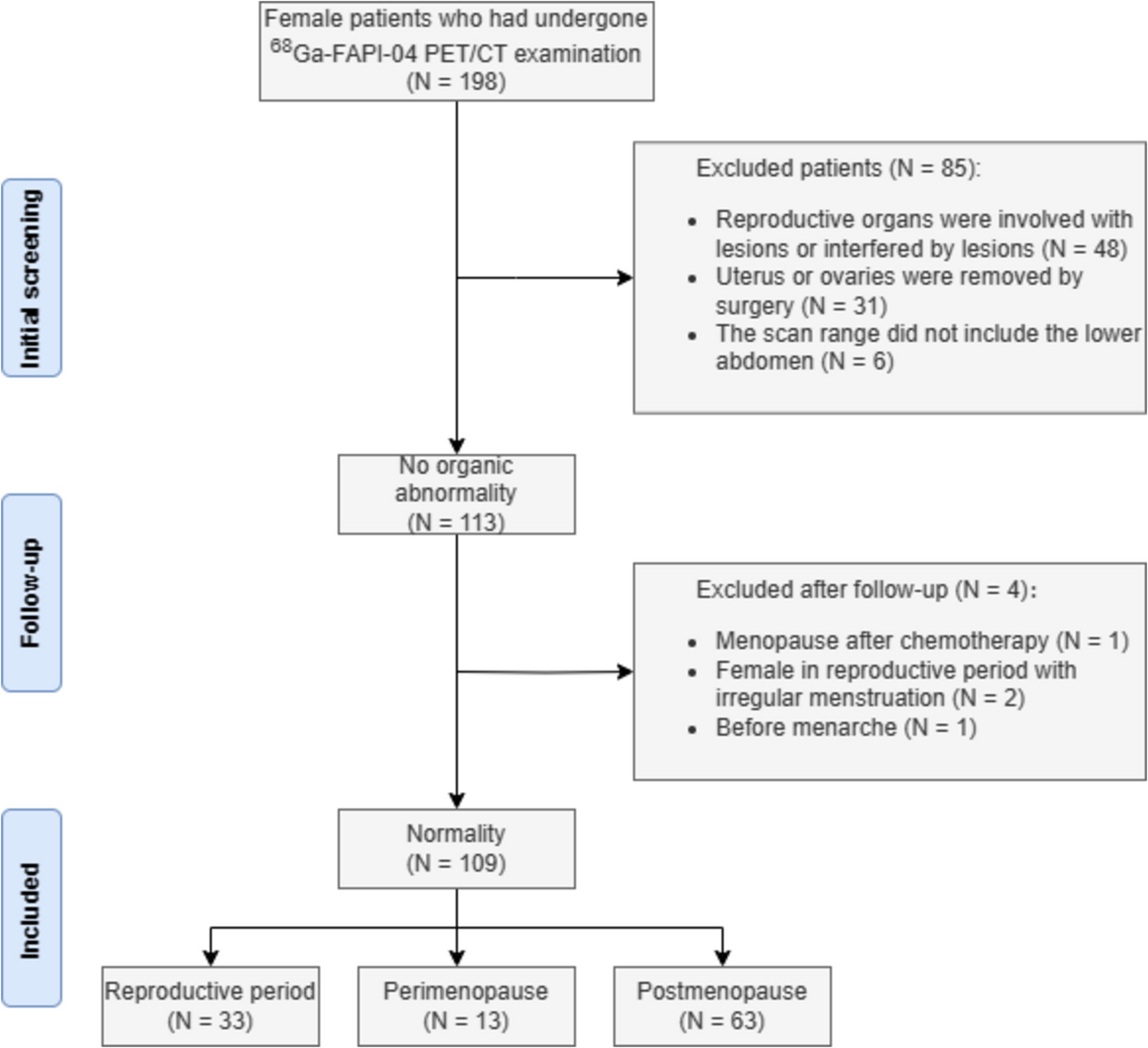
Twenty participants were consecutively recruited for enrollment in this study between October 2021 and September 2022. Written informed consent was obtained from all patients before their inclusion in the study. The eligibility criteria were as follows: (1) age > 19 years, (2) newly diagnosed potentially resectable PDAC by imaging and/or histologic examination, and (3) written informed consent in accordance with institutional and federal regulations. Participants were excluded if they (1) were pregnant, (2) had trouble providing informed consent (3) had serious comorbidities, (4) had undergone previous major abdominal surgery within four weeks of the trial, or (5) were suspected of distant metastasis.
According to the institutional protocol, all included participants underwent pancreatic CT, [18F]FDG PET/CT, and blood tests including carbohydrate antigen 19 − 9 (CA 19 − 9, normal range [between 0 and 37 U/mL] and non-secretors [< 2 U/mL on at least 3 examinations]) for initial evaluation; furthermore, [18F]AIF-FAPI-74 PET/CT was conducted at the time of diagnosis [18]. After the initial evaluation of PDAC, resectability, staging, and the participant’s overall condition were all carefully considered while choosing the appropriate treatment strategies. Among the 20 participants, 18 (90.0%) underwent surgery and two (10.0%) received chemotherapy. Among the participants who underwent surgery, 1 underwent negative exploration because distant metastasis at the colon mesentery was identified during surgery. Therefore, pathological data from surgical specimens were available for only 17 participants who underwent curative-intent surgery (Fig. S1).
Radiosynthesis of [18F]AlF-FAPI-74
Radio thin layer chromatography instant thin layer chromatography-silica gel plates were obtained from the Pall Company (New York, USA). A Bioscan AR-2000 thin layer chromatography Imaging Scanner (Washington, DC, USA) was used to perform the Radio thin layer chromatography scan. A Gilson High Pressure Liquid Chromatography system (Middleton, USA) was used for purification or the purity check of [18F]AlF-FAPI-74. C18 and QMA Sep-Pak cartridges were obtained from Waters (Milford, USA), and [18F]Fluoride was produced by the 18O(p, n)18F reaction on 18O-enriched (97%) water using a 16.5 MeV proton beam generated by a GE PETtrace™ 800 cyclotron (Chicago, USA). The precursor of [18F]AlF-FAPI-74 was supplied by SOFIE Biosciences (Dulles, USA).
[18F]AlF-FAPI-74 was prepared from its precursor (S)-(4-carboxymethyl-7--piperazin-1-yl)-acetic acid based on the previously reported method with the slight modification [19]. Briefly, an aqueous solution of [18F]fluoride in 18O-enriched water was captured on QMA light Sep-Pak cartridge, and [18F]fluoride on the cartridge was eluted with 0.9% sodium chloride solution (0.6 mL) and methyl cyanide (0.9 mL) and reacted with aluminum chloride (0.8 µg, 6 nmol in pH 3.9, 0.5 M acetate buffer (10 µL) for 5 min at 50 °C. FAPI-74 (74 µg, 0.1 µmol) in water (74 µL) was added to the reaction mixture and reacted for 10 min at 100 °C. The reaction mixture was purified with C18 Sep-Pak cartridges to give [18F]AlF-FAPI-74 (radiochemical purity: 99.5%; radiochemical yield: 25.3 ± 6.3%; molar activity: 110 ± 34.4 GBq/µmol).
[18F]FDG and [18F]AIF-FAPI-74 PET/CT Protocol
Prior to [18F]FDG PET/CT imaging, the participants fasted for at least 8 h and their blood glucose levels were measured. Participants received 5.18 MBq/kg [18F]FDG when their blood glucose level was less than 200 mg/dL. After voiding, a PET/CT scan was performed 60 min after [18F]FDG injection. For [18F]AIF-FAPI-74 PET/CT, participants received 185 MBq of [18F]AIF-FAPI-74 PET/CT scan were performed 120 min after radiotracer injection.
We used 3 dedicated PET/CT scanners (Biograph TruePoint 40, Biograph mCT 40, and Biograph mCT 64; Siemens Healthineers, Erlangen, Germany). CT scan was performed from the cranial base to the proximal thigh without contrast enhancement. The following parameters were used for the scan: 120 kVp; matrix size, 512 × 512; slice thickness, 5 mm (TruePoint 40) or 3 mm (mCT 40, mCT 60). Subsequently, PET emission scans were performed at 7 to 9 bed positions (2 min/bed, TruePoint; 1 min/bed, mCT). Attenuation-corrected PET images were reconstructed using the following parameters: TruePoint, iterations, 2; subsets, 21; 3-mm full-width half-maximum Gaussian filter; matrix, 168 × 168; mCT, iterations, 2; subsets, 21; 5-mm full-width half-maximum Gaussian filter; and matrix, 200 × 200.
Image Interpretation
PET/CT images were analyzed using an image analysis software (Syngo.via VB20, Siemens Healthineers). Semi-quantitative and qualitative methods were used to analyze the images. The semi-quantitative analysis included measurement of PET parameters such as maximum and mean standardized uptake values (SUVmax, SUVmean) and total lesion activity (TLA; total lesion glycolysis in [18F]FDG PET/CT; total lesion FAP expression in [18F]AIF-FAPI-74 PET/CT). The SUV threshold with 40% of SUVmax was used to measure volumetric parameters. To measure the background activity, the volume of interest was drawn on the right posterior side of the liver with a 3 cm diameter sphere. In qualitative analysis, lymph nodes with higher activity than that of the regional background were regarded as positive. Three nuclear medicine physicians (two senior resident physicians, and one experienced board-certified physician) evaluated the lymph node positivity on [18F]FDG and [18F]AIF-FAPI-74 PET/CT and obtained consensus data. On pancreatic CT, lymph nodes ≥ 10 mm were defined as pathological lymph nodes.
Statistical Analysis
All statistical analyses were performed using the R software, version 4.2.2 (R Foundation for Statistical Computing). Categorical variables are expressed as numbers with percentages, and continuous variables are expressed as medians with interquartile ranges (IQR). Differences in the SUV between [18F]FDG and [18F]F-FAPI-74 PET/CT were evaluated using the Wilcoxon signed-rank test (skewed variables). The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of [18F]FDG and [18F]F-FAPI-74 PET/CT were calculated by comparing the predictive nodal status with the postoperative histology in participants who underwent curative-intent surgery. The sensitivities and specificities of the imaging modalities were compared using McNemar’s test. Pearson’s correlation was used to determine the association between CA 19 − 9 and TLA, and Fisher’s Z-transformation was performed to compare the correlation coefficients. All P-values were two-sided, and P < 0.05 was considered statistically significant.





Comments (0)