The main finding of our study is that MS is significantly impaired with increasing severity of CKD in patients with ICM and in our cohort this finding was independent of LV-EF, the extent of myocardial scarring, diabetes, hypertension, age, gender, LV mass or LV mass index.
CKD is considered a serious global public health problem with an estimated global prevalence of 13.4% [7, 30, 31]. Deteriorating renal function has been shown to be associated with an exponential increase in all-cause and cardiovascular mortality. Thus, CKD represents one of the most relevant risk factors for the occurrence of CVD [7, 32]. The development of CVD in CKD-patients is not only related to traditional cardiovascular risk factors, but also to CKD-induced vascular and myocardial remodeling, resulting in myocardial fibrosis, hypertrophy and valve disease [7, 14]. In this context, CMR feature tracking to assess MS is an accurate and reliable non-invasive tool to analyze functional consequences of these myocardial changes. Previous studies already showed that increasing severity of CKD is associated with worsening MS in patients without a history of cardiovascular disease [25]. Remarkably, even in patients without known cardiovascular disease, an increasing number of cardiovascular risk factors, including CKD, has been shown to result in a decrease of GLS [33]. Furthermore, CKD further aggravates the impairment of LV strain in T2DM patients [23]. However, in the mentioned studies, patients with known cardiovascular disease and/or ICM were excluded. Thus, the relationship between CKD and MS specifically in patients with coronary artery disease and ICM due to prior myocardial infarction and scarring is still unclear. In this study, we extend the current knowledge by showing that in patients with known ICM, increasing severity of CKD significantly impairs ventricular contractility, reflected by worsening MS. This is demonstrated by the association of established markers of renal dysfunction—such as creatinine, urea and eGFR—with impairment of MS. Besides, this association was independent of clinical parameters with a known association with MS, such as diabetes, hypertension, LV mass or LV mass index as demonstrated by a persistent relationship between increasing severity of CKD and impaired MS following adjustment for the mentioned parameters in multivariable analyses.
Demonstrating a reduced myocardial contractility in patients with CKD explains on one hand at least partially the high prevalence of CVD in this population [1,2,3,4,5, 34]; on the other hand, it highlights the importance of early diagnosis, prevention and effective therapy of CKD in order to potentially avoid its effects on cardiovascular morbidity and mortality.
Once demonstrated that patients with CKD and ICM have a reduction of myocardial contractility which is directly proportional to the severity of their CKD stage, it is interesting to speculate about the mechanisms leading to this phenomenon. A possible explanation could be a more pronounced scar burden in patients with more advanced CKD, which may be due to accelerated atherosclerosis; in fact, it is well known that scarred segments present worsened MS compared to normal, viable myocardium [18, 21, 22]. However, in our study, cohort patients with higher stages of CKD did not show a more extensive left ventricular scar burden. Furthermore, the impairment of MS throughout stages of CKD was sustained even following adjustment for LV-EF and myocardial scar burden, suggesting that the negative effect of increasing severity of CKD on myocardial contractility may be at least in part independent of LV function or the extent of myocardial scarring. It is well known that MS is affected by scar transmurality, since transmurally scarred segments exhibit a more pronounced impairment of MS than non-transmural segments [35]. However, in the light of our findings, it is tempting to speculate that a more extensive myocardial scarring as a consequence of accelerated atherosclerosis may not be the key mechanism leading to the reduced myocardial contractility in patients with CKD.
A possible explanation may lay in a direct, non-atherosclerotic mediated effect of CKD itself on myocardial function. For instance, it is well known that CKD induces a systemic, chronic proinflammatory state [7]. The CKD-related release and accumulation of hormones, enzymes, cytokines and mediators as well as CKD-associated hemodynamic alterations are implicated in characteristic changes of the myocardium and the vasculature contributing to the high cardiovascular risk of CKD-patients [12, 16,17,18,19,20,21,22,23]. Besides, it is well known that CKD is associated with characteristic alterations of myocardial structure such as pathological myocardial fibrosis, with collagen deposition between capillaries and cardiomyocytes, and cardiac hypertrophy, leading to the development of uremic cardiomyopathy [7, 14]. Therefore, it is tempting to speculate that the ventricular dysfunction detected by impaired MS in our patient population reflects these CKD-related damages on the myocardium. However, typical parameters of myocardial fibrosis in CMR, such as T1 values and extracellular volume, were not available in our patient cohort, so that future studies are needed to further assess the role of myocardial fibrosis in the association between CKD and MS in patients with ICM.
Thus, CMR in general and more specifically MS may represent a useful tool in the assessment of CKD-related myocardial damage, possibly paving the way for the initiation and assessment of therapeutic strategies in the treatment of cardiovascular disease in patients with ICM and CKD, e.g. with high dose statins or potentially heart failure medications.
Limitations
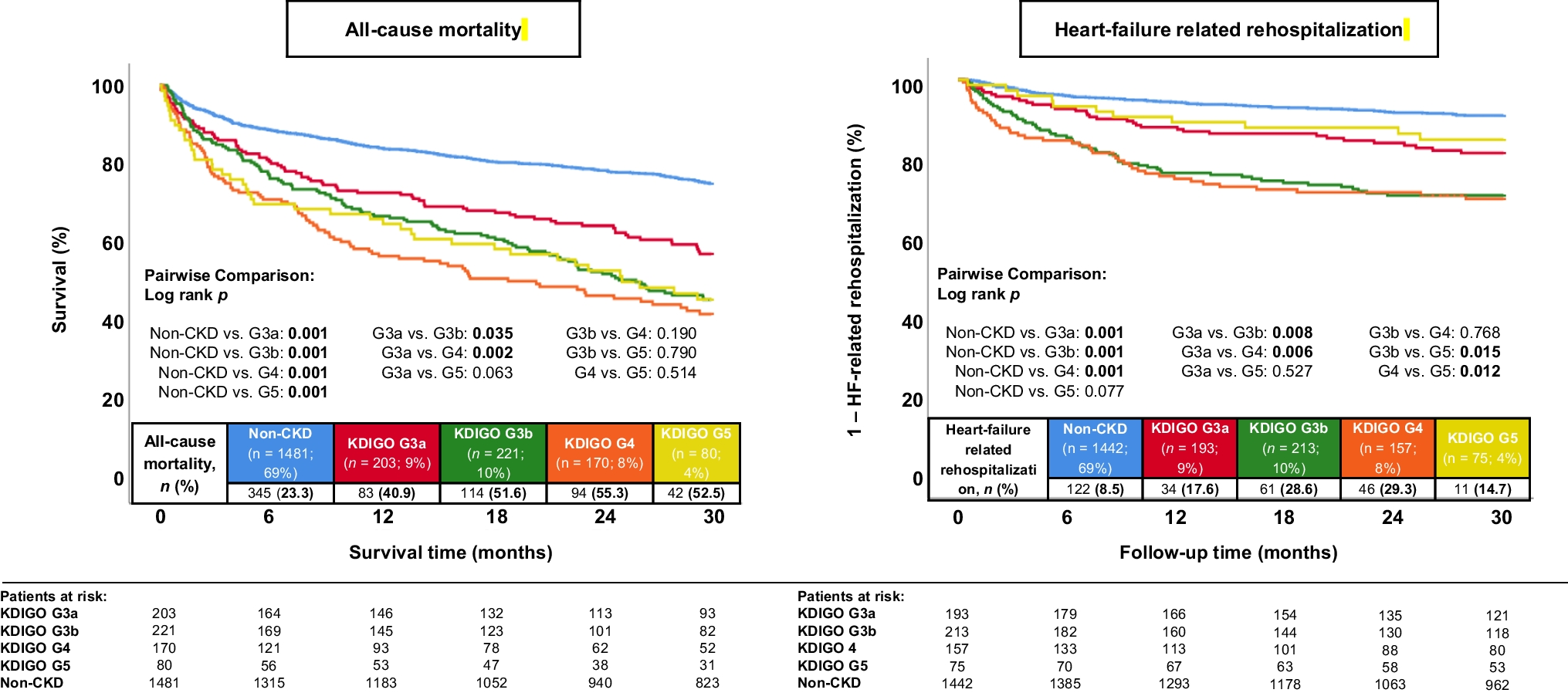
Although being, to the best of our knowledge, the first study analyzing the association between different stages of CKD and MS as determined by CMR in patients with ICM, our study population is relatively small and the statistical differences between KDIGO stages may be limited by low patient number. For example, the strain in KDIGO stage 5 was numerically impaired compared to KDIGO stage 3, but this did not reach statistical significance. Thus, our results need to be confirmed in larger study cohorts.
For patients on dialysis, eGFR may be imprecise due to the method of eGFR calculation.
Furthermore, our study focused on patients with ICM; consequently, further studies are required to analyze the effects of increasing severity of CKD on MS in patients with different types of cardiomyopathies. Due to the study design, we are unable to draw any conclusions regarding the prognostic impact of our results on patients with ICM and increasing severity of CKD. Finally, as previously described, absolute strain values are not generalizable, due to variability among vendors [35, 36].




Comments (0)