
Remember me
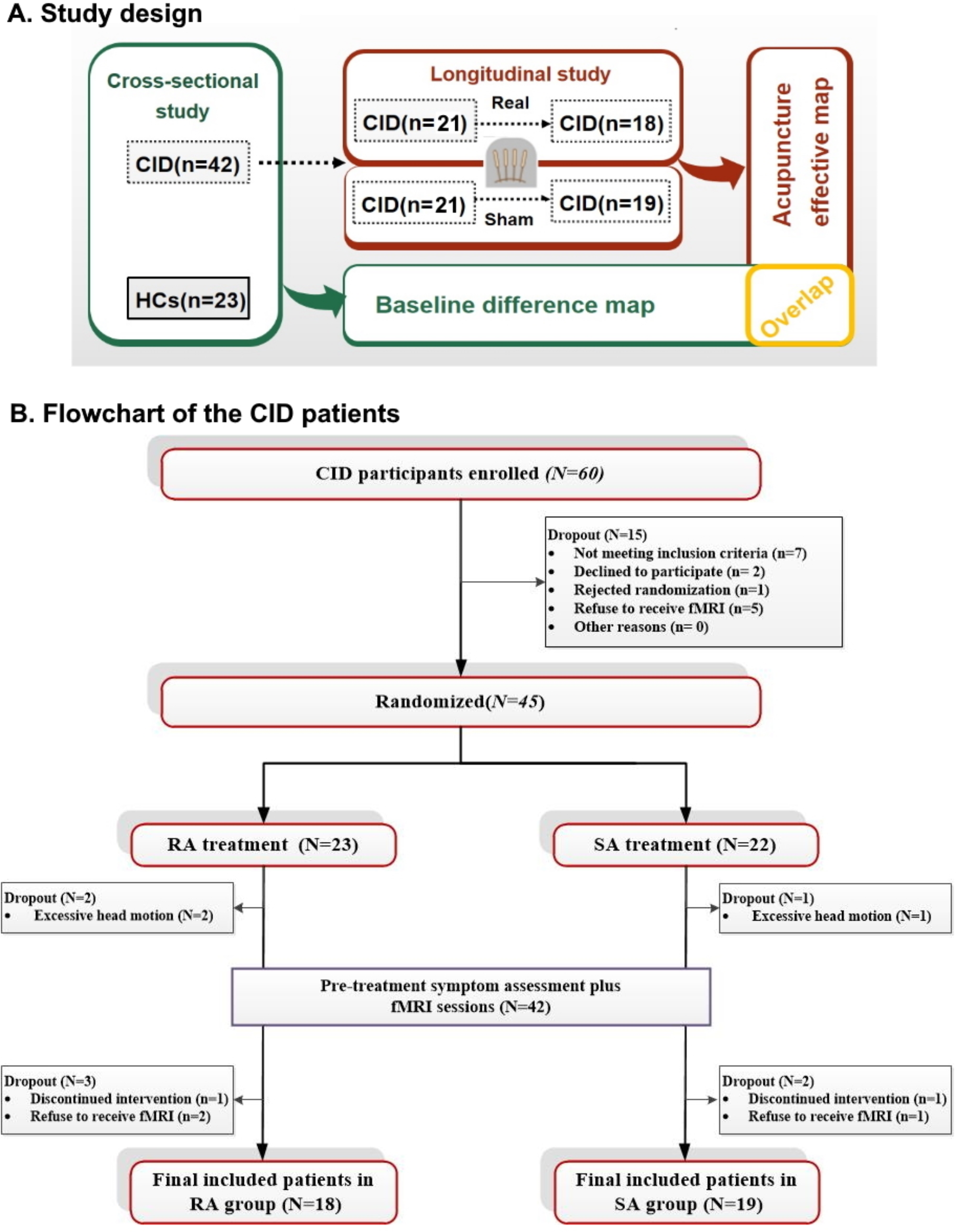
This study was comprised of two experiments: a cross-sectional and a longitudinal experiment (Fig. 1A). The cross-sectional experiment examined the neural substrate of CID by comparing the hypothalamus-based rsFC maps between CID patients and HCs. The longitudinal experiment investigated the clinical efficacy of acupuncture and its underlying neurological mechanism by comparing the hypothalamus-based rsFC map before and after treatment. Finally, a spatial overlap map was produced using the rsFC findings of both experiments to evaluate the mechanism of acupuncture therapy in relation to baseline abnormalities. The longitudinal acupuncture experiment was approved by the Institutional Review Board of Chengdu University of Traditional Chinese Medicine (2018KL-041) and submitted to the Chinese Clinical Trial Registry with the identifier (ChiCTR1800017092). All participants provided written informed consent before the initiation of any study procedures. The study adhered to the CONSORT guidelines for reporting.
Fig. 1
Study design and flowchart
(A) Study design and analytic strategy. (B) Flowchart of the CID patients.
Abbreviations: CID, chronic insomnia disorder; fMRI: functional magnetic resonance imaging; HCs, healthy controls; RA: real acupuncture; SA: sham acupuncture;
ParticipantsFrom Augest 2018 to Augest 2020, patients with CID were recruited from the hospital of Chengdu University of Traditional Chinese Medicine (CDUTCM), Chengdu second people hospital, and via online advertisements. The diagnosis of each CID patient was determined by a trained psychiatrist using the International Classification of Sleep Disorders-Third Edition (ICSD-3) [23]. Subsequently, to refine the diagnosis and exclude other neuropsychiatric disorders (such as anxiety and depression), the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) was used as part of our assessment protocol by the same psychiatrist. To be eligible for inclusion in the study, patients must meet the following criteria: (1) be of any gender, between 18 and 65 years of age, and right-handed; (2) meet the diagnostic criteria of ICSD-3 and have experienced difficulty with falling asleep, staying asleep, or early awakening for a minimum of three months; (3) meet the diagnosis of spleen and stomach disharmony in Chinese medicine (see Supplementary Materials); (4) have a score of 7 or above on the Pittsburgh Sleep Quality Index (PSQI); and (5) sign an informed consent form to voluntarily participate in the study. Patients were excluded from the study if they had the following conditions: (1) serious primary diseases affecting the liver, kidney, cardiovascular, cerebrovascular, or hematopoietic systems; (2) a history of other neuropsychiatric disorders, such as major depression or generalized anxiety; (3) systemic illnesses, such as pain, fever, cough, or surgery; (4) insomnia resulting from alcohol and/or psychotropic substance abuse and dependence, including the use of sleeping pills; (5) significant headache, migraine, or history of head trauma; (6) recent use of antibiotics, glucocorticoids, immunosuppressants, or herbal medicines within the past month; (7) pregnancy, preparation for pregnancy, or breastfeeding; (8) typical contraindications to magnetic resonance imaging (MRI) scanning, such as claustrophobia; or (9) participation in another clinical trial within the past month.
Healthy controls were recruited who met the following inclusion criteria: (1) reporting good sleep quality; (2) passing neuropsychological tests; and (3) passing a physical examination without any functional or organic disease or a history of head injury. The exclusion criteria for HCs were the same as for patients with CID.
Acupuncture interventionsA researcher who was not involved in the process of patient recruitment and treatment, used the SAS 9.2 software (SAS Institute Inc., Cary, NC, USA) to generate random numbers. All CID patients were randomly assigned to one of two groups according to the table of random numbers: real acupuncture (RA) or sham acupuncture (SA). The grouping information was blind for CID patients, recruiting researchers, and statisticians. Due to the particularity of acupuncture operation, acupuncturists were not blinded in grouping information of CID patients.
All acupuncture treatments were performed by two licensed acupuncturists. According to traditional acupuncture practices and several clinical studies [21, 24,25,26], both groups underwent a total of 20 sessions spanning a four-week treatment duration, with five consecutive daily sessions per week followed by two days off. The selected acupoints for the RA group were Baihui (DU20), Zhongwan (RN12), and Zusanli (ST36) according to a previous similar study [27]. Among them, DU20 is a commonly used acupoint to improve sleep [28, 29], while RN12 and ST36 are commonly used to regulate gastrointestinal function [30, 31]. More importantly, a recent study has found that ST36 can regulate not only GI symptoms but also sleep [32]. The acupuncturist inserted disposable stainless-steel needles vertically into the selected acupoints at a depth of 0.5 to 1.5 cun (a special unit of measurement in acupuncture; 1 cun = 25 mm) and gently twisted, lifted, and pushed the needles with consistent amplitude, force, and speed to induce the Deqi sensation. Deqi refers to the subjective feelings of soreness, numbness, heaviness, and distension experienced by the patient, as well as the sensations of heaviness, astringency, and tightness felt by the acupuncturist. After the patient reported that they had a feeling of Deqi, the needles were left in place for 30 min. Referring to a previous study [33], the SA group adopted the operation method of shallow needle insertion (depth of 2–3 mm) at non-acupoints. The non-acupoints in the SA group were located near the real acupoints (2 cm lateral to DU20, RN12, and ST36), which were not part of any known meridian or traditional acupoint. After the needle was inserted into the skin, no needle manipulation was performed, and the needle was left for 30 min.
Clinical outcome measurementThe primary outcome measurement employed was the Pittsburgh Sleep Quality Index, a well-recognized 7-item inventory to quantify the severity of insomnia symptoms. Additionally, the anxiety levels of CID patients were measured using the Self-Rating Anxiety Scale (SAS), and the depression levels were measured using the Self-Rating Depression Scale (SDS). Clinical assessments were conducted at two-time points: baseline (week 0) and post-treatment (week 4).
MRI data acquisitionThe MRI scans of CID patients were conducted both before treatment and after the completion of either real or sham acupuncture treatments. In contrast, the MRI scans for healthy controls were performed only once. All MRI data were collected using a 3.0T MRI scanner (GE Discovery 750, Milwaukee, WI) at the MRI Research Center of the University of Electronic Science and Technology. Structural images were obtained using a high-resolution T1-weighted brain volume MRI sequence with the following parameters: repetition time (TR)/echo time (TE) of 5.964/1.976 ms, slice thickness of 1 mm, 157 slices, flip angle of 9°, field of view (FOV) of 256 × 256 mm [2], and voxel size of 1 × 1 × 1 mm [3]. Functional images were acquired using an echo-planar imaging (EPI) sequence with the following parameters: TR/TE of 2000/30 ms, flip angle of 90°, acquisition matrix of 64 × 64, matrix size of 3.75 × 3.75, FOV of 240 × 240 mm, slice thickness of 4 mm, 35 slices, voxel size of 3.75 × 3.75 × 3.2 mm [3], and total volume of 255. Participants were instructed to close their eyes, remain still and quiet, avoid any head movements during the scan, remain awake, and try not to think about anything.
Demographic and clinical data analysesThe demographic and clinical outcome analyses were carried out using SPSS 22.0 software. In the cross-sectional study, two-sample t-tests and Chi-square tests were utilized to compare the baseline characteristics of participants between CID patients and HCs. In the longitudinal study, the changes in clinical symptoms (PSQI, SAS, and SDS scores) were compared before and after treatment in each group separately using paired t-tests. Subsequently, a 2-way (grouped by time) analysis of variance (ANOVA) was used to examine the differences in clinical symptoms before and after treatment between the real acupuncture and sham acupuncture groups. A p value < 0.05 was considered statistically significant.
MRI data preprocessingPreprocessing of MRI images was performed using the DPARSF (http://rfmri.org) and SPM 12 (www.fil.ion.ucl.ac.uk/spm) toolkits in MATLAB 2014b (MathWorks, Natick, MA). The steps of the preprocessing process including: (1) removal of the first 10 volumes to reduce noise interference; (2) slice timing; (3) realignment of the images to correct for any head movements; (4) co-registration of T1 images with functional images; (5) normalization of T1 images to Montreal Neurological Institute (MNI) space, and segmentation into gray matter, white matter, and cerebrospinal fluid; (6) smoothing of the images using an isotropic Gaussian kernel with a full width at half maximum of 6 mm; (7) temporal filtering using a bandpass filter with a range of 0.01–0.08 Hz, and (8) regression of nuisance signals such as global mean, white matter, cerebrospinal fluid signal, and six motion parameters.
Seed-based functional connectivity analysesTwo subregions of the hypothalamus were selected as the regions of interest (ROIs): the bilateral medial hypothalamus (MH) seed (MNI [x, y, z] = ± 4, -2, -12 mm) and the lateral hypothalamus (LH) seed (MNI [x, y, z] = ± 6, -9, -10 mm) with a 2 mm radius sphere, which had been used in previous studies [34] (Figure S1).
In the first-level analysis, the functional connectivity between the two ROIs, bilateral MH and LH, and the rest of the brain was computed. This was achieved by extracting the blood oxygen level-dependent time course from each ROI, separately, and calculating Pearson’s correlation coefficients between the time course in the LH/MH and every voxel in the whole brain. The correlation coefficients were then transformed to z-scores using Fisher’s z-transformation to improve their normality and enable better analysis using the General Linear Model in the second-level analysis.
For the cross-sectional experiment, the hypothalamus rsFC maps between patients with CID and HCs were compared using a two-sample t-test. For the longitudinal experiment, a paired t-test was used to compare the within-group statistical maps, and a 2-way ANOVA was used to compare the between-group statistical maps. A threshold of p < 0.005 at the voxel level and p < 0.05 at the cluster level, corrected for false discovery rate (FDR), was applied to the group analysis, in accordance with our previous studies [35, 36]. In FDR-corrected clusters, the minimum voxel value was set to 20. If the results did not survive correction for FDR, a small volume correction was applied to the regions associated with sleep and insomnia. The disease-related brain regions were defined as ROIs and generated using the Anatomical Automated Labeling Atlas. To correct for multiple comparisons, Monte Carlo simulations were performed using the 3dFWHMx and 3dClustSim tools from the AFNI software (https://afni.nimh.nih.gov) and applied to the ROIs.
A conjunction analysis was conducted to determine if the altered hypothalamic rsFC in patients with CID would be modulated by acupuncture treatment. The conjunction analysis compared the rsFC alteration maps of CID patients and the effect maps of acupuncture in the RA and SA groups, respectively.
Finally, to explore the association between clinical outcomes and rsFC, we also performed correlation analyses between the significantly altered hypothalamus-based rsFCs (‘post’ minus ‘pre’) and the corresponding PSQI changes in the RA group.
Comments (0)